Article Text

Abstract
Objective To determine heart rate centiles during the first 5 min after birth in healthy term newborns delivered vaginally with delayed cord clamping.
Design Single-centre prospective observational study.
Setting Stavanger University Hospital, Norway, March–August 2019.
Patients Term newborns delivered vaginally were eligible for inclusion. Newborns delivered by vacuum or forceps or who received any medical intervention were excluded.
Interventions A novel dry electrode electrocardiography monitor (NeoBeat) was applied to the newborn’s chest immediately after birth. The newborns were placed on their mother’s chest or abdomen, dried and stimulated, and cord clamping was delayed for at least 1 min.
Main outcome measures Heart rate was recorded at 1 s intervals, and the 3rd, 10th, 25th, 50th, 75th, 90th and 97th centiles were calculated from 5 s to 5 min after birth.
Results 898 newborns with a mean (SD) birth weight 3594 (478) g and gestational age 40 (1) weeks were included. The heart rate increased rapidly from median (IQR) 122 (98–146) to 168 (146–185) beats per minute (bpm) during the first 30 s after birth, peaking at 175 (157–189) bpm at 61 s after birth, and thereafter slowly decreasing. The third centile reached 100 bpm at 34 s, suggesting that heart rates <100 bpm during the first minutes after birth are uncommon in healthy newborns after delayed cord clamping.
Conclusion This report presents normal heart rate centiles from 5 s to 5 min after birth in healthy term newborns delivered vaginally with delayed cord clamping.
- neonatology
- cardiology
Data availability statement
No data are available.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
What is already known on this topic?
Heart rate is an important clinical indicator of newborn status immediately after birth.
Centile charts of newborn heart rate after birth lack data from the first 60 s and were obtained with immediate cord clamping.
Delayed cord clamping is increasingly implemented as standard of care and may result in a smoother newborn transition with less bradycardia.
What this study adds?
A heart rate centile chart from 5 s to 5 min after birth in healthy newborns delivered vaginally and with delayed cord clamping.
The median heart rate increases rapidly and peaks at approximately 1 min after birth, earlier than previously reported.
Heart rates below 100 beats per minute are uncommon in newborns who do not need intervention and account for less than 5% of newborns at 30 s after birth.
Background
The transition from intrauterine to extrauterine life involves a series of rapid cardiopulmonary changes.1 The heart rate of the newborn infant is one of the most important clinical indicators used to determine the need for and response to resuscitation.2 A heart rate below 60 beats per minute (bpm) is considered an indication to commence cardiac compressions, and below 100 bpm is a requirement for positive pressure ventilation.2
Widely referenced heart rate centiles were published in 2010 by Dawson et al.3 These were obtained from newborns undergoing immediate cord clamping, using a pulse oximeter, and acquiring data from approximately 60 s after birth. Infants had a median (IQR) heart rate of 96 (65–127) bpm at 1 min of life, rising to 139 (110-166) at 2 min. These findings have led to confusion among clinicians, since they suggest that many ‘normal’ infants meet criteria for intervention.
It has been suggested that pulse oximetry systematically underestimates heart rate at birth compared with three-lead gel electrode electrocardiography (ECG).4 Furthermore, ECG detects heart rate much earlier compared with pulse oximetry.5–8 A novel newborn heart rate metre based on dry electrode ECG allows reliable heart rate monitoring at 3–10 s after birth,9 even earlier than previously achieved by conventional three-lead gel electrode ECG.4 6
Delayed cord clamping, defined as that occurring beyond 1 min after birth, is increasingly implemented as standard of care worldwide and might result in a smoother newborn transition at birth and less bradycardia.10 11 The International Liaison Committee on Resuscitation (ILCOR) recently suggested that ECG can be used to provide a rapid and accurate estimation of the heart rate.12 Therefore, due to changes in standard umbilical cord management practices and in the technology to assess heart rate, the pattern of normal heart rate changes during the first minutes of life requires re-evaluation.
The aim of this study was to describe the pattern of heart rate changes during the first minutes after birth in uncompromised term newborns delivered vaginally and undergoing delayed cord clamping, using a dry electrode ECG-based newborn heart rate monitor.
Methods
Setting
This study was conducted at Stavanger University Hospital, Norway, from March to August 2019. Stavanger University Hospital serves a population of 350 000 with approximately 4500 deliveries annually and is the only hospital in the region with delivery and newborn services. A midwife and a nurse assistant are present at each birth and may call on an obstetrician for assistance whenever needed. Delayed cord clamping is implemented as standard procedure.
Inclusion and exclusion process
All women admitted to the department of obstetrics in labour at term (≥37 weeks of gestation) were asked to participate in the study. Newborns delivered by caesarean section or assisted delivery (ie, vacuum or forceps) and newborns who received any medical interventions (eg, supplementary oxygen or assisted ventilation) at birth were excluded.
Data collection
Laerdal Global Health (Stavanger, Norway) developed a novel neonatal heart rate metre named NeoBeat, incorporating dry electrodes in an abdomen-shaped circlet for rapid application to the newborn. Instead of gel electrodes used in traditional three-lead ECG, NeoBeat uses dry electrodes, and thorough skin cleaning prior to application is unnecessary. The NeoBeat heart rate algorithm is based on a zero-crossing count algorithm13 that adds a proprietary layer that includes noise detection and noise handling. Motion is the primary source of ECG distortion, and the algorithm uses measured acceleration energy as well as ECG features such as amplitude and rate variability to determine when there is likely too much motion to get a reliable heart rate. A predecessor of NeoBeat, based on the same technology, was used in a study in Tanzania, and heart rate was registered within 3–10 s after birth.14 NeoBeat displays the newborn’s heart rate and can transfer heart rate data via Bluetooth Low Energy to the Liveborn tablet application (Laerdal Global Health, Stavanger, Norway).
During the study period, each delivery room was equipped with a NeoBeat. If prospective parental consent was given, the nurse assistant attending the birth carried a tablet (iPad, Apple, Cupertino California, USA) with the Liveborn application installed. The nurse assistant marked the exact time of birth (ie, time when the whole body was delivered) by starting a counter in the application, and the dry electrodes were applied to the newborn by the midwife without delay (online supplemental figure 1). Midwifes were trained in the use of the NeoBeat and the Liveborn application using manikins, and data collection was trialled during a pilot phase before study commencement. The newborn was managed in accordance with standard guidelines: drying and stimulation, immediate skin-to-skin contact and delayed cord clamping for at least 1 min. The Liveborn application recorded real-time heart rate data from the ECG every second during the data collection period. NeoBeat did not provide heart rate if it detected that the signal was too distorted with noise or motion artefacts. The nurse assistant marked the time of cord clamping in the application. The heart rate was recorded for the first 5 min after birth, or until the cord was clamped if this occurred beyond 5 min. Data collection did not interfere with the routine handling of the newborns after birth. Patient and birth characteristics were extracted from the medical record.
Supplemental material
Supplemental material

Overview of inclusion and exclusion process.
Data analysis
We excluded cases where time of birth or heart rate data were suspected to be erroneous based on the following criteria: (1) if the heart rate was registered by the ECG before the recorded time of birth and (2) less than 30 s of heart rate registered during data collection.
Statistics
Using an SD for the heart rate of 21 bpm, as reported by Linde et al,14 a sample size calculation showed that ≥68 observations were needed at each second to estimate the median heart rate with a margin of error of less than ±5 bpm. To obtain a margin of error of less than ±5 bpm for the estimate of the 10th and 90th centiles, sample size calculations showed that at least 482 observations were required.15 We planned to include 500–1000 newborns to ensure sufficient good quality data. Heart rate data were extracted using Mathlab 2019a (MathWorks, Natick, Massachusetts, USA). Data were analysed, and charts were drawn in R V.3.6.2 (R Core Team 2019, Vienna, Austria). Continuous variables are presented as mean (SD) when normally distributed, and median (IQR) when non-normally distributed. Centile charts were drawn by calculating centiles empirically and then smoothing them using the local regression method (LOESS).16
Ethics
Written parental consent was obtained prior to inclusion.
Results
In total, 1764 newborns were delivered vaginally at term during the study period. Consent was obtained for the inclusion of 1416 newborns in the data collection. Of those, 424 were excluded due to: (1) connectivity/technical issues during data collection (n=231), (2) instrumental delivery (n=142) and (3) medical interventions after birth (n=51). Another 94 newborns were excluded during data analysis because the NeoBeat registered heart rate before the recorded time of birth (n=75) or too few heart rate observations were registered (n=19). The remaining 898 newborns were included in the analysis, and their characteristics are presented in table 1.
Newborn characteristics
Time of cord clamping was recorded in 784 newborns, and umbilical cord blood values were available for 854 newborns. Figure 1 shows an overview of the inclusion and exclusion process.
A total of 227 038 individual heart rate observations were registered, resulting in a median (IQR) of 276 (243–286) heart rate observations for each newborn, and 808 (741–819) individual heart rate observations at each second during the 5 min study period. At least 68 individual heart rate observations were reached at 5 s (n=77) and at least 482 individual heart rate observations were reached at 14 s (n=510) after birth. The numbers of individual heart rate observations recorded at each second after birth are displayed in figure 2. The heart rate centiles from 5 s after birth are shown in table 2 and figure 3.
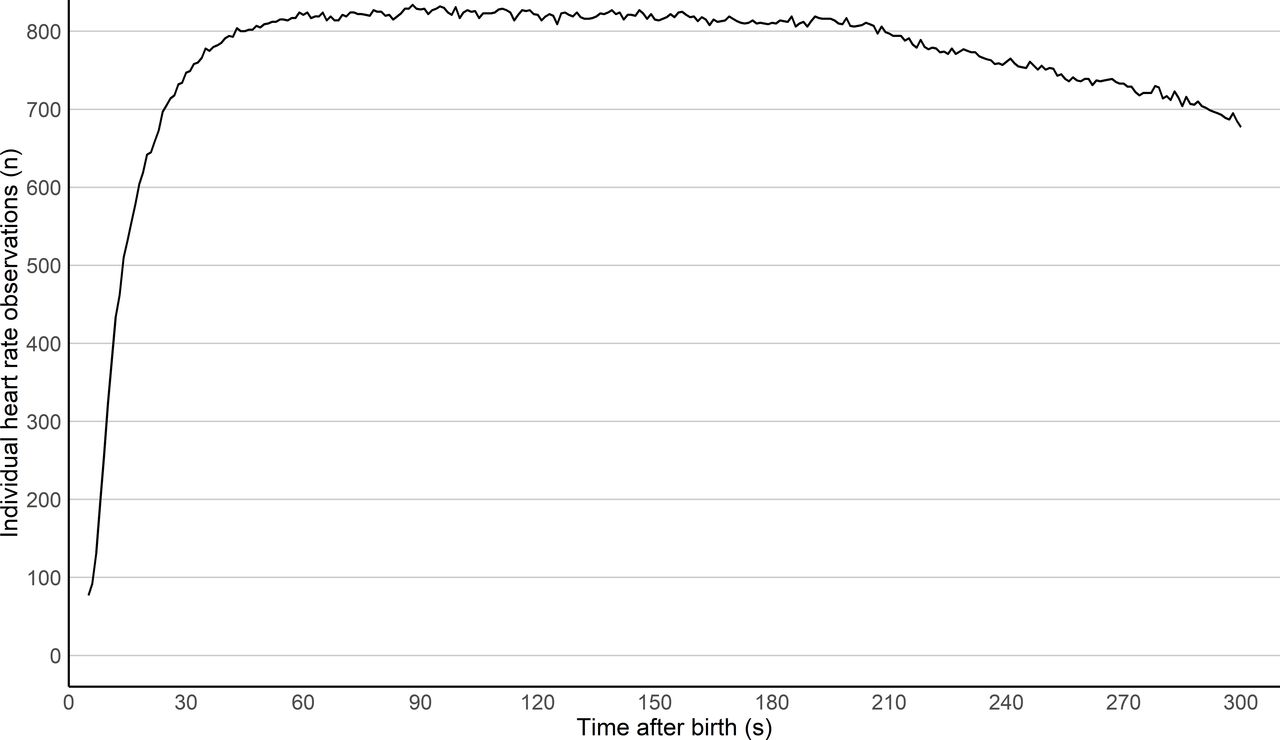
Number of individual heart rate observations at each second after birth.

{kind=link}
{kind=link}
{kind=link}
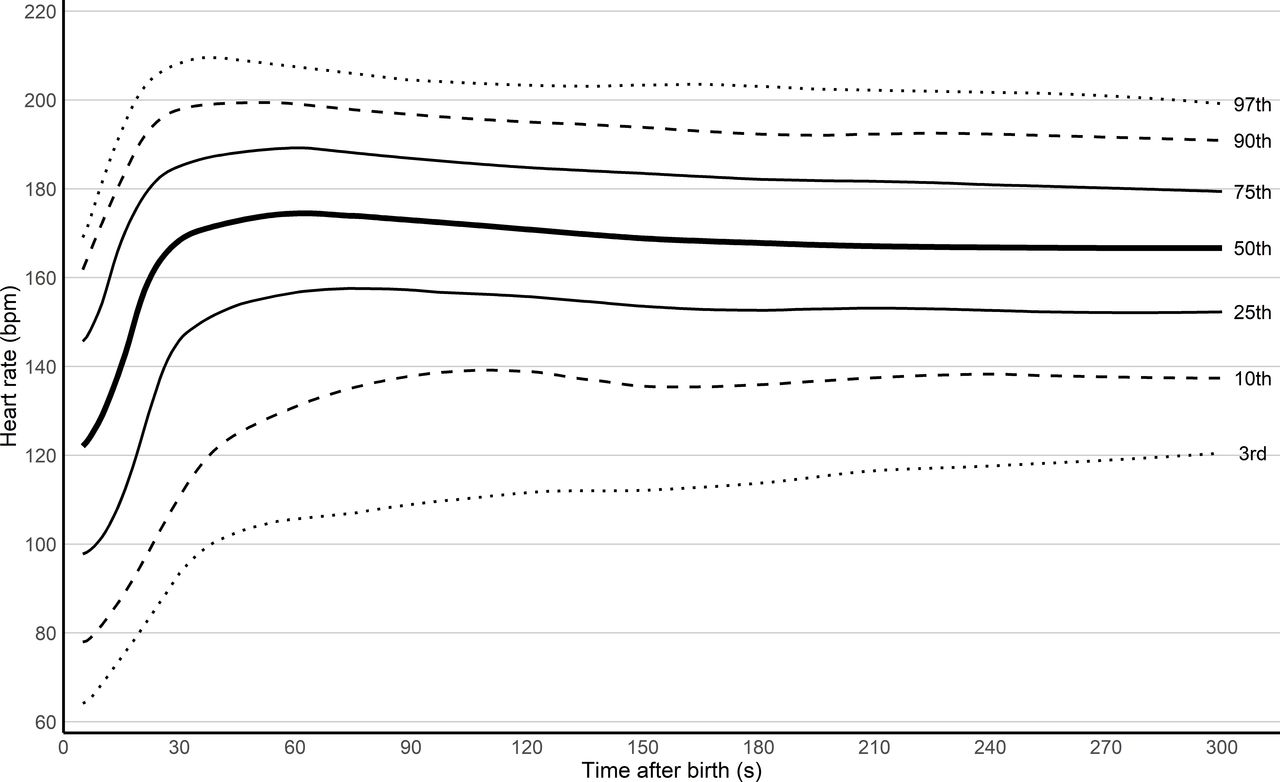
The 3rd, 10th, 25th, 50th, 75th, 90th and 97th heart rate centiles from 5 s after birth for vaginally born term newborns with delayed cord clamping and no medical intervention.
Heart rate centiles the first 5 min after birth for term newborns delivered vaginally with delayed cord clamping and no medical intervention
The median (IQR) heart rate was 122 (98–146) bpm at 5 s after birth, after which it increased rapidly to 175 (157–189) bpm at 61 s after birth. During the following minutes, the median (IQR) heart rate slightly decreased to approximately 167 (152–179) bpm at 5 min after birth. Heart rates below 100 bpm were uncommon, and the 10th and 3rd centiles crossed 100 bpm at 22 and 34 s after birth, respectively.
Discussion
In this study, we describe the pattern of normal heart rate changes using centiles during the first 5 min after birth in term newborns delivered vaginally, in a setting with delayed cord clamping as standard of care. A novel ECG application method made it feasible to achieve heart rate measurements from 5 s after birth, filling a gap in the existing literature. The heart rate centiles from Dawson et al 3 did not include the first minute after birth. This is of importance, as resuscitation guidelines recommend resuscitative actions during the first 60 s after birth based on the newborn’s heart rate as well as breathing. Most guidelines recommend initiation of positive pressure ventilation and oxygen saturation monitoring of infants with heart rates below 100 bpm.12
Our findings differ from the existing centile charts by Dawson et al,3 where heart rates below 100 bpm were commonly observed in healthy newborns during the first minutes after birth. In our study, a heart rate below 100 bpm after 30 s of life was rare. Our results may provide support for the controversial recommendation to provide respiratory support to newborns with heart rates below 100 bpm. Studies of compromised infants requiring assistance are required to progress this question.
Furthermore, Dawson et al 3 reported that the 50th centile heart rate reached a plateau of around 160 bpm at 3 min after birth, whereas our results suggest an early peak of approximately 175 bpm within the first minute after birth, thereafter slowly decreasing. The recent study of Padilla-Sánchez et al 11 assessed heart rates using pulse oximetry during the first 10 min of life after delayed cord clamping. They found an earlier stabilisation of heart rate compared with Dawson et al.3 They attributed this difference to the haemodynamic effects of delayed cord clamping. However, their results differ from ours in that they found that heart rates below 100 bpm are to be expected in at least 10% of all healthy newborns the first minute after birth.
In our study, we recorded heart rates by ECG, whereas Dawson et al 3 and Padilla-Sánchez C et al 11 conducted their studies using a pulse oximeter. Pulse oximetry may underestimate heart rates when compared with ECG, especially during the first minutes of life,4 7 and might have contributed to the lower heart rates and slower rise in heart rate measured by Dawson and Padilla-Sánchez et al. We believe that the different methods of measuring heart rates provide an important explanation for the differences between the centiles of Dawson and ours. ILCOR suggests that in babies requiring resuscitation, ECG can be used to provide a rapid and accurate estimation of heart rate. Hence, a reference range for heart rates obtained using ECG is required.
During labour, the normal baseline fetal heart rate is 110–160 bpm. Brief decelerations to 100–120 are common, attributed to vagal activation in association with uterine contractions.17 18 The same changes may occur as the newborn descends through the birth canal, and our results suggest a drop in heart rate immediately prior to birth, followed by a rapid increase during the first minute of life.
Delayed cord clamping is considered beneficial for the cardiovascular transition and newborn outcomes.19 The immediate effect of delayed cord clamping on heart rate is not clear, and randomised controlled studies on ventilated preterm lambs show conflicting results.10 20 Clinical studies on newborns confirm that delayed cord clamping results in a lower heart rate during the first minutes after birth.21 22 Importantly, these studies were conducted with a pulse oximeter. Our study did not analyse heart rate in relation to cord clamping and therefore cannot draw conclusions regarding the impact of delayed cord clamping on heart rate.
All newborns in the present study were delivered vaginally. In the study by Dawson et al,3 nearly 50% of the newborns were delivered by caesarean section. They reported a slower rise in heart rate and stabilisation at a lower level around 150 bpm in newborns born by caesarean sections compared with vaginal births (stabilising around 160 bpm). Similar findings were reported by Gonzales and Salirrosas,23 describing lower heart rate obtained by pulse oximetry in newborns born by caesarean sections compared with vaginal births. Our centile charts are only applicable to term newborns born vaginally, and studies on normal heart rate measured by ECG in newborns born by caesarean sections are required.
Limitations
The time of the first heart rate detection varied between newborns. For half of the included newborns, the heart rate was detected from 13 s, whereas for 75%, the heart rate was detected from 22 s. Even some healthy newborns require stimulation after birth, which will possibly delay the heart rate detection of the NeoBeat due to motion, and these newborns could possibly also have a different heart rate than those without need of stimulation. We have no reason to believe that this has a major impact on the results, but the presented heart rates for the first 15–20 s could be considered more cautiously.
There was a high percentage of missed registrations due to technical issues. This was mostly due to the interruptions in the Bluetooth connection between NeoBeat and the Liveborn application. However, this occurred at random and should not create a bias. To make data collection less intrusive to the parents, we assigned data collection to the attending midwives and nurse assistants. The staff therefore operated the NeoBeat and the application while carrying out other tasks, possibly contributing to the relatively high number of missed cases due to technical issues and erroneous recordings. Dispersing data collection to several individuals may affect validity. However, all personnel involved in data collection were thoroughly instructed in all procedures. Finally, the reference values presented in this study are obtained by ECG and cannot be applied as reference values for heart rates measured by pulse oximetry.
Conclusion
Using novel dry electrode ECG technology, this study describes the pattern of normal heart rate changes from 5 s to 5 min after birth in healthy, vaginally delivered term newborns undergoing delayed cord clamping. The median heart rate rapidly increased from 122 bpm at 5 s after birth to a maximum of 175 bpm at approximately 1 min after birth. The third centile crossed 100 bpm at 34 s, suggesting that heart rates <100 bpm during the first minutes after birth are uncommon in healthy newborns after delayed cord clamping.
Data availability statement
No data are available.
Ethics statements
Ethics approval
The study was approved by the regional ethical committee (REKvest 2018/338) and the hospital data protection officer.
Acknowledgments
We would like to thank all the midwives and nurse assistants in the labour units at Stavanger University Hospital and parents with their newborns participating in this study. We would also like to thank Anastasia Ushakova for statistical counselling.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors PAB, SIR, HLE and KØ designed the study protocol. PAB and SIR practically implemented, supervised and carried out the study and the data collection on site. JE extracted and PAB analysed the heart rate data. All authors participated in the interpretation of the results. PAB drafted the initial manuscript. All authors read, revised and approved the final manuscript.
Funding PAB has an unconditional PhD grant from the Laerdal Foundation (Grant Number 30026) and SR has an unconditional Post Doc grant from the Laerdal Foundation (Grant Number 50007), Stavanger, Norway. NeoBeats were provided by Laerdal Medical.
Disclaimer The external funding sources had no role in study design, data collection, data analysis, data interpretation, writing of the report or in the decision to submit the paper for publication. All authors had full access to all the data in the study and had final responsibility for the decision to submit for publication.
Competing interests JE is employed at Laerdal Medical. All other authors had no other financial relationships with any organisations that might have an interest in the submitted work in the previous 3 years or no other relationships or activities that could appear to have influenced the submitted work.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.
Linked Articles
- Fantoms