Article Text

Abstract
Objective To evaluate if nebulised surfactant reduces intubation requirement in preterm infants with respiratory distress treated with nasal continuous positive airway pressure (nCPAP).
Design Double blind, parallel, stratified, randomised control trial.
Setting Sole tertiary neonatal unit in West Australia.
Patients Preterm infants (290–336 weeks’ gestational age, GA) less than 4 hours of age requiring 22%–30% supplemental oxygen, with informed parental written consent.
Interventions Infants were randomised within strata (290–316 and 320–336 weeks’ GA) to bubble nCPAP or bubble nCPAP and nebulised surfactant (200 mg/kg: poractant alfa) using a customised vibrating membrane nebuliser (eFlow neonatal). Surfactant nebulisation (100 mg/kg) was repeated after 12 hours for persistent supplemental oxygen requirement.
Main outcome measures The primary outcomes were requirement for intubation and duration of mechanical ventilation at 72 hours. Data analysis followed the intention-to-treat principle.
Results 360 of 606 assessed infants were eligible; 64 of 360 infants were enrolled and randomised (n=32/group). Surfactant nebulisation reduced the requirement for intubation within 72 hours: 11 of 32 infants were intubated after continuous positive airway pressure (CPAP) and nebulised surfactant compared with 22 of 32 infants receiving CPAP alone (relative risk (95% CI)=0.526 (0.292 to 0.950)). The reduced requirement for intubation was limited to the 320–336 weeks’ GA stratum. The median (range) duration of ventilation in the first 72 hours was not different between the intervention (0 (0–62) hours) and control (9 (0–64) hours; p=0.220) groups. There were no major adverse events.
Conclusions Early postnatal nebulised surfactant may reduce the need for intubation in the first 3 days of life compared with nCPAP alone in infants born at 290–336 weeks’ GA with mild respiratory distress syndrome. Confirmation requires further adequately powered studies.
Trial registration number ACTRN12610000857000.
- infant, premature
- respiratory distress syndrome
- nebulization
- surfactant
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
What is already known on this topic?
Surfactant replacement therapy reduces the severity of respiratory distress in preterm newborn infants.
Until now, administration of exogenous surfactant has required instrumentation of the trachea, with bolus surfactant delivered via a laryngeal mask, tracheal tube, angiocath or feeding tube.
What this study adds?
We provide the first evidence of a successful non-invasive nebulised surfactant replacement in preterm infants with respiratory distress syndromevia a new-generation vibrating membrane nebuliser.
Early postnatal nebulised surfactant may reduce the need for intubation in very and moderate preterm infants with mild RDS.
These findings require confirmation in further adequately powered studies.
Introduction
Primary treatment of neonatal respiratory distress syndrome (RDS) with non-invasive nasal continuous positive airway pressure (nCPAP) is increasing. However, worsening of RDS may necessitate delayed intubation and bolus surfactant therapy. Delayed surfactant delivery may promote atelectrauma due to alveolar collapse, with resultant increased respiratory disease severity and prolongation of mechanical support. Brief tracheal instrumentation for bolus delivery of surfactant may reduce atelectrauma.1–4 However, tracheal instrumentation is associated with tube malposition or perforation, induces transient cardiovascular instability and a stress response, and is often accompanied by transient sedation and/or paralysis.5–8
Surfactant nebulisation offers an alternative approach consistent with a non-invasive treatment.9 10 In animals with surfactant deficiency, nebulised surfactant reduces the frequency of adverse haemodynamic effects compared with bolus surfactant instillation, and improves homogeneity of surfactant distribution,7 11 12 lung compliance, ventilation efficiency index and oxygenation.13 Nebulised surfactant to reduce the severity of neonatal respiratory distress in unventilated human infants was described in 1964, via aerosol generated within an incubator.14 Three of four subsequent studies used jet nebulisation,15–18 which is highly inefficient due to air entrainment.19 Only one of these four studies was a randomised controlled trial16: it showed no effect of nebulised surfactant on the requirement for mechanical ventilation, duration of nCPAP or ventilation, oxygenation requirements, or the incidence of bronchopulmonary dysplasia. A 2012 Cochrane review concludes there is insufficient evidence from randomised controlled trials to guide use of nebulised surfactant in preterm infants at risk of RDS.20
New miniature vibrating membrane nebulisers do not require bias flow and are more efficient than the jet nebulisers,21 reducing nebulised surfactant wastage. However, surfactant delivery remains lower when nebulisation is via a mask or nasal prongs compared with a tracheal tube.22 A pilot non-randomised study using a vibrating membrane nebuliser noted lower nCPAP failure and (bolus) surfactant replacement therapy in very preterm infants compared with contemporaneously recorded infant data.18 While encouraging, this non-randomised pilot study does not permit definitive comment about the efficacy of nebulised surfactant during nCPAP for treatment of neonatal RDS.
We aimed to evaluate the clinical efficacy and feasibility of nebulised surfactant for the treatment of RDS in very preterm infants. We hypothesised that nebulised surfactant administered in the first 4 hours of life to newborn infants with clinical signs suggestive of evolving RDS would reduce the incidence of nCPAP failure without increasing the incidence of adverse clinical outcomes.
Patients and methods
We conducted a single-centre, blinded, pragmatic, randomised controlled trial to assess the feasibility, safety and short-term efficacy of nebulised surfactant for the treatment of evolving RDS in infants at 290–326 weeks’ gestational age (GA).
Eligibility and recruitment
Inborn neonates were enrolled by the recruiting team (SM, CAB) between 14 October 2010 and 12 May 2012. The eligibility criteria for study inclusion were 290–336 weeks’ GA, <4 hours’ of age, and clinical signs suggestive of evolving mild to moderate RDS requiring treatment with nCPAP of 5–8 cmH2O and supplemental fractional inspired oxygen (FiO2) of 0.22–0.30 to maintain a peripheral oxyhaemoglobin saturation of 86%–94%. The exclusion criteria included prior intubation or surfactant treatment, known pneumothorax, cardiorespiratory instability, cardiothoracic malformation and obvious chromosomal aberrations.
Randomisation and masking
Eligible infants were randomised (SM, CAB) after obtaining written informed parental consent. Computer-generated randomisation sequences were generated with balanced block design for each GA strata (290–316 weeks’ GA and 320–336 weeks’ GA) and sealed in opaque, sequentially numbered envelopes. All infants remained behind an opaque screen with the treatment team for 20–30 min for either nebulised surfactant or sham nebulisation. Continuous positive airway pressure (CPAP) water chambers were emptied and refilled at the end of nebulisations to reduce the risk of unblinding clinicians to treatment assignment associated with surfactant deposition. The clinical team responsible for management were blinded to group assignment. nCPAP strategy was the same for both study groups: nCPAP commenced at 5 cmH2O and increased up to 8 cmH2O for increasing FiO2. nCPAP bias flow used 6–8 L/min as required to achieve active bubbling. Masked data were analysed by an investigator (JJPJJ) with minimal involvement in recruitment or treatment.
Intervention
The intervention group received 200 mg/kg body weight aerosolised surfactant (poractant alfa, Chiesi Farmaceutici SpA, Parma, Italy) via a customised vibrating membrane nebuliser (eFlow neonatal nebuliser system, PARI Pharma, Starnberg) positioned between the mask and the bubble nCPAP circuit. Nebulisation commenced as soon as possible after randomisation. Repeat surfactant nebulisation (100 mg/kg) was given for persisting oxygen requirement and/or respiratory distress (persistent tachypnoea >60 breaths/min, sternal or intercostal muscle recession, or grunting) 12 hours after initial nebulisation.
nCPAP failure criteria
nCPAP therapy failure was defined as one or more of the following criteria:
FiO2 >0.35 over more than 30 min OR FiO2 >0.45 at anytime.
More than four apnoeas/hour OR two apnoeas requiring bag and mask ventilation.
Two capillary blood gas samples with a pH <7.2 and partial pressure of carbon dioxide >65 mm Hg (or partial pressure of carbon dioxide in arterial blood (PaCO2) >60 mm Hg if arterial blood gas sample).
Intubation deemed necessary by the attending physician.
Infants who failed nCPAP were intubated and received surfactant according to normal unit practice (200 mg/kg poractant alfa, with additional 100 mg/kg poractant alfa after 12 hours if required). Extubation criteria were not defined.
Outcomes
The primary dichotomous outcome was the need for intubation within the first 72 hours of life, and the primary continuous outcome was the mean duration of mechanical ventilation at 72 hours of age. The secondary outcomes included the number of infants that remained intubated at 24 hours, 72 hours and 7 days; time to intubation; total surfactant dose per kilogram; associated neonatal morbidities; and physiological stability following randomisation.
Sample size and statistical analysis
The intubation frequency of infants commenced on nCPAP after birth at 290–336 weeks’ gestation in the preceding 12 months was 30%. A sample size of 70 patients (35 patients/group) would detect a reduction in intubation frequency from 30% to 5%, with a power of 80% and a significance level of α=0.05 (two-sided test).
Data were analysed for the whole group, and in the predefined GA strata on an intention-to-treat basis. The primary dichotomous outcomes were assessed using Pearson’s χ2 test and relative risk (RR) with Fisher’s exact test for low event rate as secondary outcomes. Continuous data were summarised as mean (SD) or median (range) for parametric and non-parametric data distributions, respectively. A t-test or Mann-Whitney U test was used to assess differences between groups in continuous data at 72 hours. Data analysed using Kaplan-Meier survival analysis included log-rank (Mantel-Cox) χ2 statistic for assessments of time-dependent differences. All reported p values are two-sided.
Results
Baseline demographics and clinical characteristics
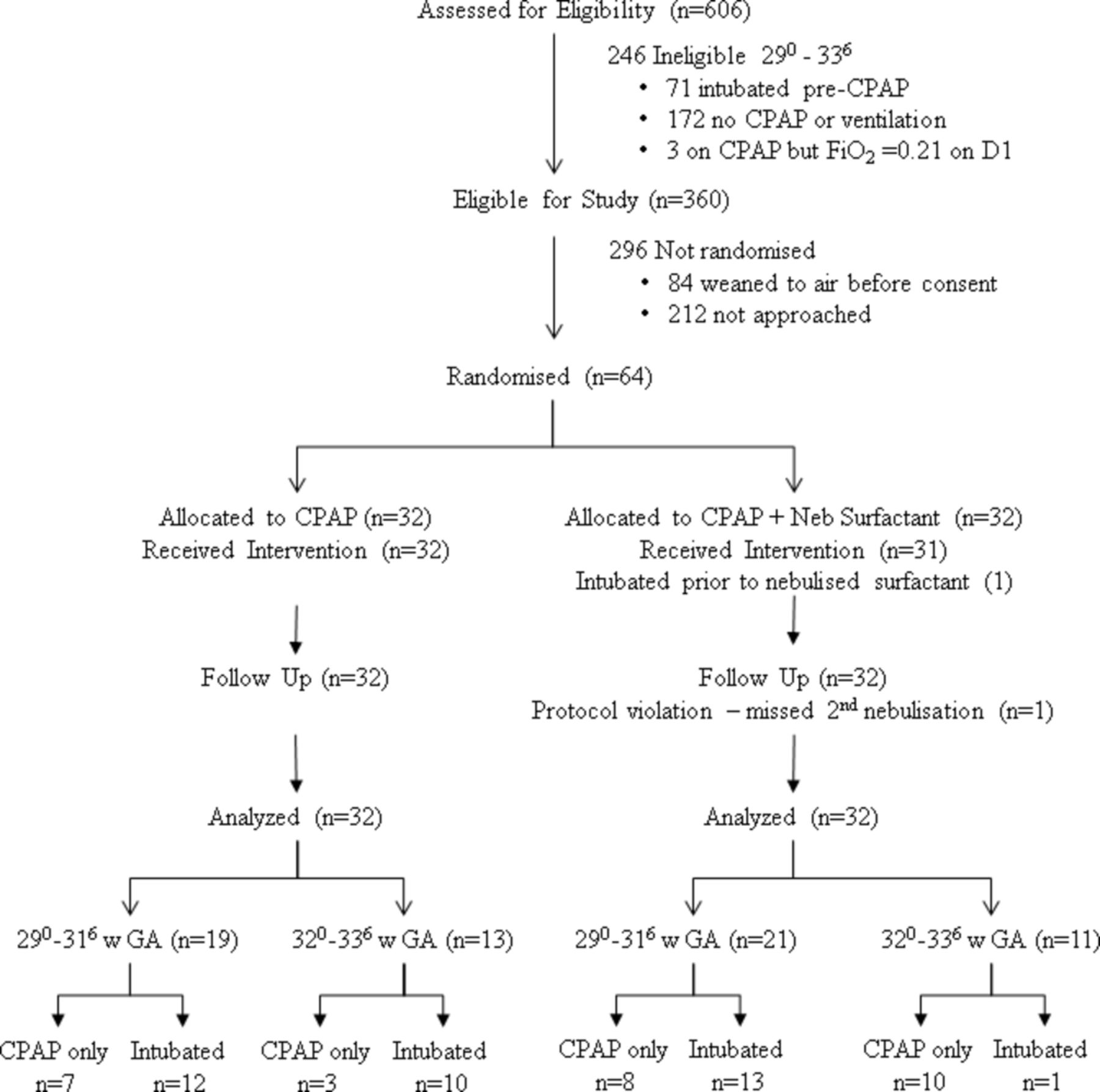
Figure 1 shows the Consolidated Standards of Reporting Trials diagram for recruitment. Sixty-four infants were recruited to the study between 15 October 2010 and 14 May 2012. One infant missed its second surfactant nebulisation despite remaining in supplemental O2 (protocol violation). One infant was intubated immediately after randomisation prior to surfactant nebulisation. Both infants were included in the full analysis (intention-to-treat). The study was closed to recruitment after 19 months due to insufficient funding/personnel.
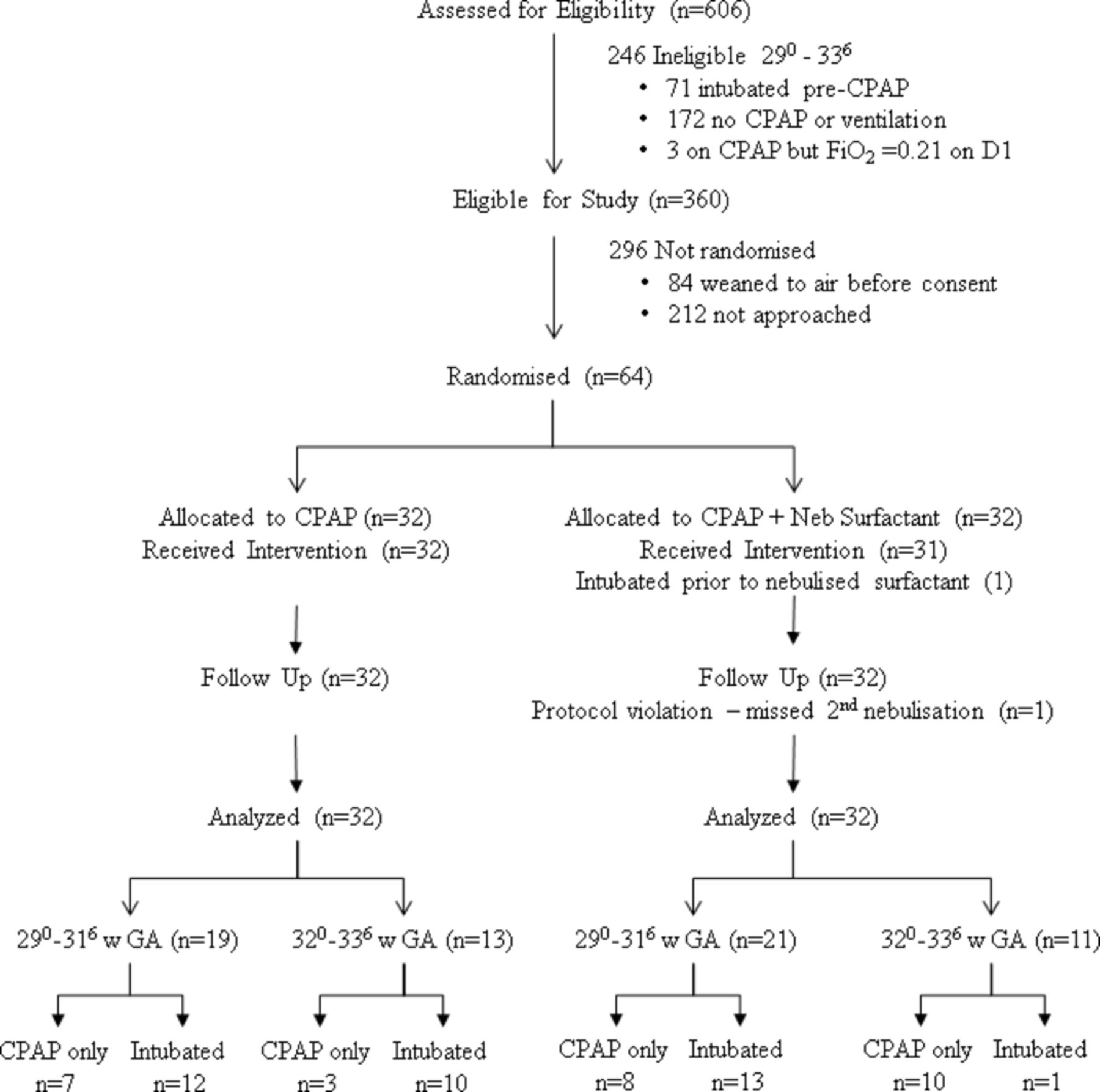
Consolidated Standards of Reporting Trials diagram for study recruitment and treatment assignment. CPAP, continuous positive airway pressure; FiO2, fractional inspired oxygen; GA, gestational age.
Only 64 of 360 eligible infants were enrolled, due primarily to non-availability of study personnel to ensure masking of the intervention. No differences were seen in baseline demographic variables and clinical characteristics of the recruited cohort (table 1). The proportion of male and caesarean section deliveries was higher in the study group versus eligible but not recruited cohort (online supplementary table 1), but no other selection bias was evident.
Supplemental material
Patient demographics
Primary outcome
Surfactant nebulisation reduced the requirement for intubation within 72 hours of birth: 11 of 32 infants were intubated in the intervention group compared with 22 out of 32 infants receiving CPAP alone (RR (95% CI)=0.526 (0.292 to 0.950)). The reduced risk for intubation was restricted to the 320–336 weeks’ GA group: 1 out of 11 infants receiving CPAP plus nebulised surfactant was intubated compared with 10 out of 13 infants receiving CPAP alone (RR (95% CI)=0.254 (0.089 to 0.727)). There was no difference in intubation risk in the 290–316 weeks’ GA group: 12 out of 21 infants receiving CPAP plus nebulised surfactant were intubated compared with 12 out of 19 infants receiving CPAP alone (RR (95% CI)=0.860 (0.389 to 1.90)). The duration of ventilation in the first 72 hours was not different between the groups: the median (range) was 0 (0–62) hour for the nebulisation group and 9 (0–64) hours for the control group (p=0.220).
Secondary outcomes
The secondary outcomes are shown in table 2. There was no difference between the groups in the total duration of any mechanical support (mechanical ventilation+nCPAP) or in the duration of supplemental O2. Surfactant nebulisation did not alter the proportion of infants remaining intubated after 24 hours, 72 hours or 7 days. The duration of mechanical ventilation in infants intubated because they met the nCPAP failure criteria was marginally longer in the nebulised surfactant group compared with those in the nCPAP-only group. However, this finding is skewed by the differences in the GA of infants failing CPAP in each group: within the 290–316 weeks’ GA substrata, the median (IQR) duration of ventilation was not different between the nebulised (25.5 (13.9–82) hours) and the control (19.2 (13.6–46.7) hours) groups (U=58.0, p=0.436). The total surfactant dose did not differ between the groups. Nine infants received a second nebulised surfactant dose after 12 hours due to persisting FiO2 requirement or clinical signs of respiratory distress. The mean (95 % CI) difference in bolus surfactant use after intubation was 9.2 (−14.5 to 32.9) mg/kg for the intervention versus the control.
Secondary outcomes
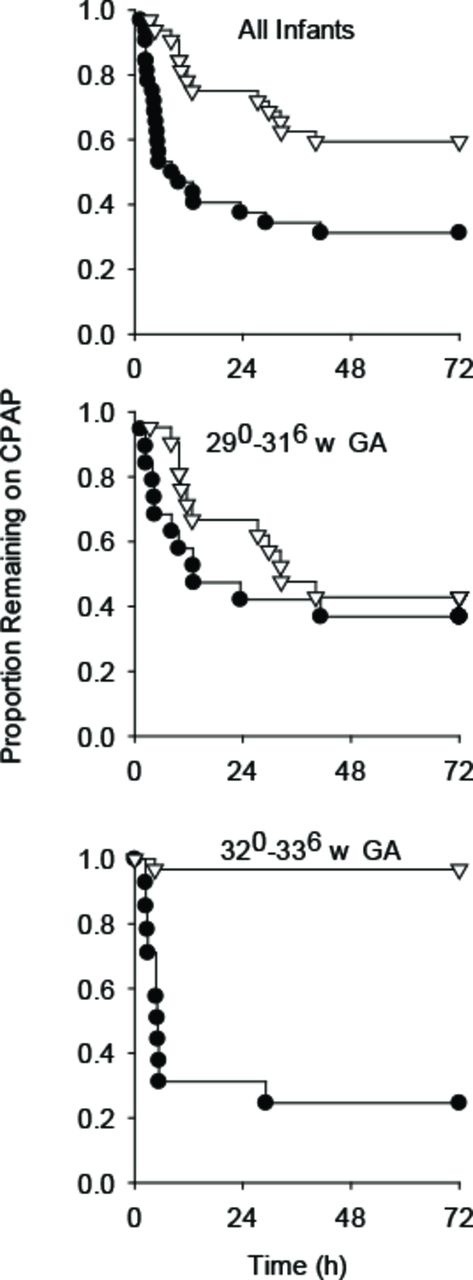
The time dependencies of the requirement for intubation (as the estimated probability of remaining on nCPAP) are displayed as Kaplan-Meier survival curves for the whole cohort and the two substrata in figure 2. For the subgroup of infants failing nCPAP, the time to meet the nCPAP failure criteria was significantly longer after nebulised surfactant (table 2). The median delay (95% CI) in time to intubation for the nebulisation group was 4.5 (−0.18 to 7.17) hours compared with the control group. While not significant, 290–316 weeks infants receiving nebulised surfactant tended to meet the criteria after a more prolonged initial nCPAP course (figure 2B).

{kind=link}
{kind=link}
Kaplan-Meier survival curves illustrating the temporal relation between the treatment assignment and the probability of remaining on nCPAP all infants (top); 29.0-31.6 w gestation stratum (middle); and c) 32.0-33.6 w gestation stratum (bottom). Solid circles: nCPAP only; open triangles: nCPAP+nebulised surfactant. Infants were more likely to remain on CPAP if they received nebulised surfactant. Stratified analysis indicated a significant benefit of nebulised surfactant was restricted to the more mature gestational age group. CPAP, continuous positive airway pressure; GA, gestational age; nCPAP, nasal continuous positive airway pressure.
Nebulisation was associated with a transient increase in transcutaneous partial pressure of carbon dioxide (TcpCO2) in some infants, which resolved immediately following face mask removal. One infant developed apnoea necessitating a brief procedural pause. No other significant change in heart rate or clinical desaturation occurred during nebulisation. The incidence of neonatal morbidities was not different between the groups. Two infants from the control group developed pneumothorax.
The main reasons for failure were exceeding the modest maximum FiO2 failure criteria or due to clinician assessment of significant respiratory distress (table 3). Clinical indicators of respiratory distress did not differ between the groups for infants requiring intubation (table 4).
Reason for failure of nCPAP
Clinical variables at failure of CPAP
Discussion
We report a preliminary, blinded, randomised controlled trial to evaluate the efficacy of nebulised surfactant in the first 4 hours of life for non-invasive clinical management of moderately preterm and very preterm neonates with evolving mild to moderate RDS. The non-invasive combination of nebulised surfactant and nCPAP is consistent with recent trends in neonatal respiratory care. Our finding of reduced risk for intubation after surfactant nebulisation with a vibrating membrane nebuliser contrasts with the only other clinical trial of nebulised surfactant in human infants, which used a jet nebuliser system.16 The vibrating membrane system used in the current study enhances the delivery of the surfactant to the infant’s respiratory system, without protein denaturation (which complicates ultrasonic nebulisation) or aerosol dilution.9 23 The therapy is simple to deliver, needing only maintenance of a patent airway with face mask nCPAP. The vibrating nebuliser system is also highly portable, optionally battery-driven and not dependent on bias gas flow. Together these features highlight the potential for effective surfactant nebulisation in the delivery room, and for initial treatment of infants in non-tertiary and/or remote centres prior to transfer.
Surfactant nebulisation is a safe procedure when undertaken with appropriate monitoring. Apnoea requiring brief interruption of nebulisation was a rare event (1 of 32), while increased TcpCO2 during surfactant nebulisation (secondary to external dead space) was temporary. The absence of differences in the incidence of adverse clinical outcomes suggests that nebulisation has minimal adverse effects within the first week of life.
Subgroup analysis showed surfactant nebulisation was only successful in reducing intubation in the more mature infant group. The single baby failing CPAP in the 320–336 intervention group was intubated only at the discretion of the attending physician for persistent respiratory distress. In contrast, 50% of infants in the control group in the 320–336 weeks’ GA strata were intubated due to impaired oxygenation, impaired ventilation or both. The apparent difference in the reason for nCPAP failure in the 320–336 weeks’ GA strata between surfactant treated and untreated groups supports a lung recruitment effect of nebulised surfactant with consequent reduced supplemental oxygen requirement. However, these findings require verification in a future, adequately powered clinical trial, as this study was not powered to detect subgroup differences.
For those infants that required intubation, infants in the nebulised surfactant group reached the CPAP failure criteria later than the infants in the nCPAP-only control group. The longer time lapse before meeting the nCPAP failure criteria in the nebulisation group was not associated with more severe lung disease at the time of intubation as the FiO2 and PaCO2 tended to be lower rather than higher than the corresponding measurements at the time of nCPAP failure in the control group. The longer time to meet failure criteria in the more immature infants implies some physiological benefit of nebulised surfactant was achieved, despite the absence of a difference in intubation risk for more immature infants. Surfactant redosing before 12 hours may be indicated for nebulised surfactant therapy given the mean time to failure was just less than 12 hours in the nebulised group.
The duration of mechanical ventilation did not differ between the two groups. The marginally longer median duration of mechanical ventilation in nebulised and subsequently ventilated infants compared with the intubated infants in the control group should be interpreted with considerable caution as extubation criteria were not mandated for this preliminary trial. Further, the failures in the nebulised group were skewed to the more immature infants, which may influence the duration of ventilation as evidenced by the absence of difference in the duration of ventilation in infants failing nCPAP in the 290–316 stratum. Importantly, there were also no differences between the study groups in the number of infants still intubated at 24 hours, 72 hours or after 7 days, or the development of gross air leak.
The failure rate for CPAP was substantially higher in this cohort than anticipated from historical data. We believe this outcome is likely a consequence of the time required for the separate recruiting team to arrive to consent and randomise, during which time many infants on CPAP were weaned to air and became ineligible for the study. Additionally, the blinded treating clinician group reserved the right to intubate infants with perceived significant respiratory distress in the absence of elevated FiO2 or PaCO2, when they considered early bolus surfactant therapy would be beneficial. This early surfactant approach reflected the routine unit practice during the study. The clinical bias towards early bolus surfactant was especially evident in the 290–316 weeks’ GA group, in which more than a third of infants who failed nCPAP failed on the basis of clinical assessment rather than due to exceeding apnoea/bradycardia, FiO2 or PaCO2 limits. While ‘clinician decision’ is not a strict intubation criteria, the clinicians should have applied this rationale equally to both groups as the clinicians were blinded to the intervention. Whether a more permissive nCPAP strategy would result in clinical efficacy of nebulised surfactant in the 290–316 weeks’ GA group remains unknown and should be considered in the design of future studies.
Our study has several limitations, including the small study group numbers and the lack of power to detect subgroup effects. As a pilot, single-centre study, sample size was targeted at a large effect size. Recruitment was halted at 91% of the planned sample size due to departure of study personnel and financial constraints. The frequency of intubation was higher than expected in the overall cohort compared with historical data due to exclusion of infants weaned rapidly to air and increased bias towards early bolus surfactant prevailing during the study period (2010–2012), even in the absence of significant oxygen requirement. The bias towards early bolus surfactant therapy as a clinician preference was especially evident in the more immature infant group: more than a third of the less mature infants who failed nCPAP failed on the basis of perceived respiratory distress rather than exceeding apnoea/bradycardia, FiO2 or PaCO2 limits. Whether a more permissive nCPAP strategy would result in clinical efficacy of nebulised surfactant in the 290–316 weeks’ GA group remains unknown and requires evaluation in an adequately powered, well-designed randomised controlled trial. Furthermore, as a pilot study, we targeted infants with evolving mild to moderate RDS and cannot exclude the possibility that some of the babies may not have had surfactant deficiency or true RDS. Future studies should target infants requiring an FiO2 of at least 0.25.
An index to ensure a consistent level of impaired oxygenation (eg, nCPAP pressure × FiO2) was not used.2 Nonetheless, the prevailing nCPAP pressure at nCPAP failure did not differ between the treatment groups. Combining nebulised nCPAP with higher nCPAP pressures may facilitate successful nebulised surfactant treatment in the atelectatic, surfactant-deficient lung.
This trial only evaluated nebulised surfactant using a face mask as the patient interface. A supraglottic mask may offer more directed and hence efficient surfactant nebulisation than the face mask, although placement is associated with transient cardiorespiratory disturbance.24–27 However, anecdotal studies and clinical trials using supraglottic masks only evaluate bolus rather than nebulised surfactant delivery.24–26 28 29 A comparison of supraglottic versus face mask as the interface for surfactant nebulisation would inform on the relative efficacy and safety for each approach.
Future trials should consider that the vibrating membrane of the nebuliser adapter used for our trial was custom-designed to optimise surfactant delivery to the 32 weeks’ GA preterm respiratory system via the upper airways, including the nares.30 Different airway dimensions could influence the number and nature of respired nebulised surfactant particles and influence treatment efficacy. Membrane design requires further evaluation before applying this methodology to the extremely preterm infant range, or to alternative delivery interfaces such as the laryngeal mask.
Conclusion
Nebulised surfactant administered in the first 4 hours of life to very and moderately preterm infants with mild RDS may promote successful establishment of non-invasive respiratory support. These findings require confirmation in a subsequent, adequately powered randomised controlled trial evaluating the benefits of nebulised surfactant in infants with mild to moderate respiratory distress. Future trials should target evaluation of the patient interface for nebulisation, and consider enrolling infants receiving contemporary ‘less-invasive’ surfactant delivery methods as a comparator group.
Acknowledgments
The authors gratefully acknowledge the babies and their families who participated in the study. We also appreciate the assistance of King Edward Memorial Neonatal Clinical Care Unit clinical staff for their willingness to enrol babies in this study. Particular thanks are extended to Dr Gayatri Jape and Dr Piyush Shah for their contributions to recruitment of study infants in the latter part of the study. We also acknowledge and thank the following colleagues who critically reviewed the study proposal and were named coinvestigators on the successful funding application: Associate Professor Sunalene Devadason, Professor Karen Simmer and Dr Ronnie Hagan.
References
Footnotes
Contributors SM conceptualised and designed the study, designed the data collection instruments, submitted the ethics application, obtained seed funding from the Women and Infants Research Foundation, was the liaison officer with PARI for provision of the nebulisation devices, was the primary recruiting officer at the main study site, reviewed and revised the draft manuscript, and approved the final manuscript as submitted. CAB assisted SM in the design of the data collection instruments, coordinated and supervised the data collection at the two study sites, critically reviewed the manuscript, and approved the final manuscript as submitted. JJPJJ assisted SM in the development of the study design and data collection instruments, assisted SM in obtaining seed funding for the study, obtained the principal funding from the State Health Research Advisory Committee, had primary responsibility for the study, drafted the initial manuscript and approved the final manuscript as submitted.
Funding Grants from the State Health Research Advisory Committee and the Women and Infants Research Foundation, WA, supported all phases of this study. SM was supported by the Swiss National Science Foundation. JJP is supported by an NHMRC Senior Research Fellowship (GRT1077691). Fisher & Paykel Healthcare provided ventilator circuits for the nebulisation but had no role in the study design, conduct, data analysis, writing of the manuscript or decision to submit it for publication. PARI Pharma provided equipment for nebulisation. PARI Pharma approved the technical description of their equipment in the manuscript but had no other role in the study design, conduct, data analysis, writing of the manuscript or decision to submit it for publication. SM (via the University of Bern, Switzerland) holds a patent with PARI Pharma for nebulisation with a vibrating membrane (EP 1818070 A3).
Competing interests JJP receives unrestricted grants of surfactant product from Chiesi Farmaceutici SpA (Parma, Italy) for unrelated neonatal ventilation research in preterm lambs. Surfactant for the current study was purchased from the hospital pharmacy at retail price using grant funding described above. JJP has also received equipment and unrestricted grant funding from Fisher & Paykel for unrelated preterm lamb research in the past. SM has a conflict of interest as disclosed above in relation to his patent with PARI Pharma.
Patient consent Not required.
Ethics approval The Human Ethics Committees of King Edward Memorial Hospital (KEMH) and the University of Western Australia approved the registered study (ACTRN12610000857000).
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement Individual de-identified participant data that underlie the results reported in this article are available on reasonable request until 5 years after publication to researchers who provide a methodologically sound proposal and whose use of the data has been approved by an independent review panel, where appropriate.
Collaborators Prof Karen Simmer, Dr Ronny Hagan, A/Prof Sunalene Devadason