Article Text

Abstract
Background When intubating newborns, clinicians aim to position the endotracheal tube (ETT) tip in the midtrachea. The depth to which ETTs should be inserted is often estimated using the infant’s weight. ETTs are frequently incorrectly positioned in newborns, most often inserted too far. Using the vocal cord guide (a mark at the distal end of the ETT) to guide insertion depth has been recommended.
Objective To determine whether estimating ETT insertion depth using the vocal cord guide rather than weight results in more correctly positioned ETT tips.
Design Single-centre randomised controlled trial.
Setting Level III neonatal intensive care unit (NICU) at a university maternity hospital (National Maternity Hospital, Dublin, Ireland).
Patients Newborn infants without congenital anomalies intubated in the NICU.
Interventions Participants were randomised to have ETT insertion depth estimated using weight [insertion depth (cm) = weight (kg) +6] or vocal cord guide.
Main outcome measure Correct ETT position, that is, tip between the upper border of the first thoracic vertebra (T1) and the lower border of the second thoracic vertebra (T2) on a chest X-ray as determined by one paediatric radiologist masked to group assignment.
Results 136 participants were randomised. The proportion of correctly positioned ETTs was similar in both groups (weight 30/69 (44%) vs vocal cord guide 27/67 (40%), p=0.731). Most incorrectly positioned ETT (69/79, 87%) were too low.
Conclusion Estimating ETT insertion depth using the vocal cord guide did not result in more correctly positioned ETT tips.
Trial registration number ISRCTN39654846.
- Neonatology
- Clinical Procedures
- Evidence Based Medicine
- Intensive Care
- Resuscitation
Statistics from Altmetric.com
What is already known on this topic?
Clinicians often estimate how far to insert an endotracheal tube (ETT) in newborns using their weight.
ETTs are often incorrectly placed in newborns, most often inserted too far.
What this study adds?
Using the vocal cord guide to estimate insertion depth instead of weight did not result in more correctly placed ETTs.
Background
When intubating newborns, clinicians aim to position the tip of the endotracheal tube (ETT) in the midtrachea to allow for symmetrical ventilation of both lungs and even distribution of surfactant. Incorrectly placed tubes increase the risk of unequal lung expansion, air leaks, asymmetrical surfactant distribution and accidental extubation.1 2 After insertion, ETT tip position is determined using chest X-ray (CXR). The tip of the ETT should appear between the upper border of the first thoracic vertebra (T1) and the lower border of the second thoracic vertebra (T2).3
A number of different methods are used to guide clinicians in estimating the correct depth of insertion at the time of oral intubation. Commonly, clinicians use a formula based on the newborn’s weight1:
ETT insertion depth (cm)=6 + wt (kg)
While this method is widely used, it has been found to frequently result in incorrectly positioned tubes, especially in infants <1000 g in weight in whom it may lead to overestimation of ETT insertion depth.4 5 The use of gestational age to estimate ETT insertion has also been proposed.6 7 In a randomised study at our centre, we found that using this method did not result in more correctly positioned ETTs when compared with the weight-based formula.8 A recent Cochrane review concluded that there is insufficient evidence to support any single method of estimating ETT insertion depth and that further randomised controlled trials are warranted.9
Many ETTs are designed with a vocal cord guide (VCG). The VCG was originally described as a 2 mm wide solid black line added to neonatal ETTs with the upper border of the line at a distance of 24 mm, 26 mm and 28 mm from the tip of size 2.5, 3.0 and 3.5 ETTs, respectively.10 It is recommended that the ETT should be advanced until the guide is visible at the vocal cords on direct laryngoscopy and secured at this depth.2 10 Use of this method has been reported to eliminate the incidence of main bronchus intubation.10
We wished to determine whether estimating ETT insertion depth using the VCG rather than the weight-based formula resulted in more correctly positioned ETT tips.
Methods
We performed this randomised controlled trial at the neonatal intensive care unit (NICU) at the National Maternity Hospital (NMH) Dublin, Ireland. NMH is a university maternity hospital with >9000 births annually and a level 3 NICU. Prior to this study, ETT insertion depth was routinely estimated using weight.
Infants were eligible for inclusion if they were intubated orally in the NICU. Delivery room intubations were not included as infants are not routinely weighed prior to resuscitation at our hospital. However, infants intubated in the delivery room who were subsequently intubated in the NICU were eligible for inclusion in our study. We excluded infants with upper airway or lung anomalies that could distort upper airway anatomy. Each infant could be enrolled in the study once only. The decision to intubate a patient was at the discretion of the treating doctor.
Where possible, parents were approached in advance to provide consent to participate in this study. However, as intubation is often performed at short notice as an emergency procedure, some infants were enrolled using a waiver of consent.11 This is recognised as an ethical and acceptable approach to enrolling patients in studies concerned with emergency care and procedures.12 13 Following enrolment, parents were approached as soon as possible to provide consent for their infant’s information to be collected and included in this study. Parents were informed that they could withdraw their child from this study at any time without explanation. Information sheets were given to all parents prior to obtaining written consent. The study protocol was approved by the NMH Research Ethics Committee and registered with Current Controlled Trials (ISRCTN39654846).
Infants were randomly assigned in a 1:1 ratio to the ‘weight’ or ‘vocal cord guide’ group. The randomisation was stratified by gestational age (<28 weeks and ≥28 weeks) to ensure equal distribution of more immature infants between the groups. We generated the group assignment schedule in blocks of 4 using a random number table and kept it concealed from caregivers and investigators. We placed cards containing the group assignment ‘weight’ or ‘vocal cord guide’ in sequentially numbered, sealed, opaque envelopes. These cards also had space where the clinician intubating the infant recorded the following data: weight and estimated insertion depth for infants assigned to the ‘weight’ group; and depth at which the ETT was secured and accidental extubation before CXR was performed for infants in both groups. The envelopes were placed in two boxes (one for each stratum) and kept in the NICU.
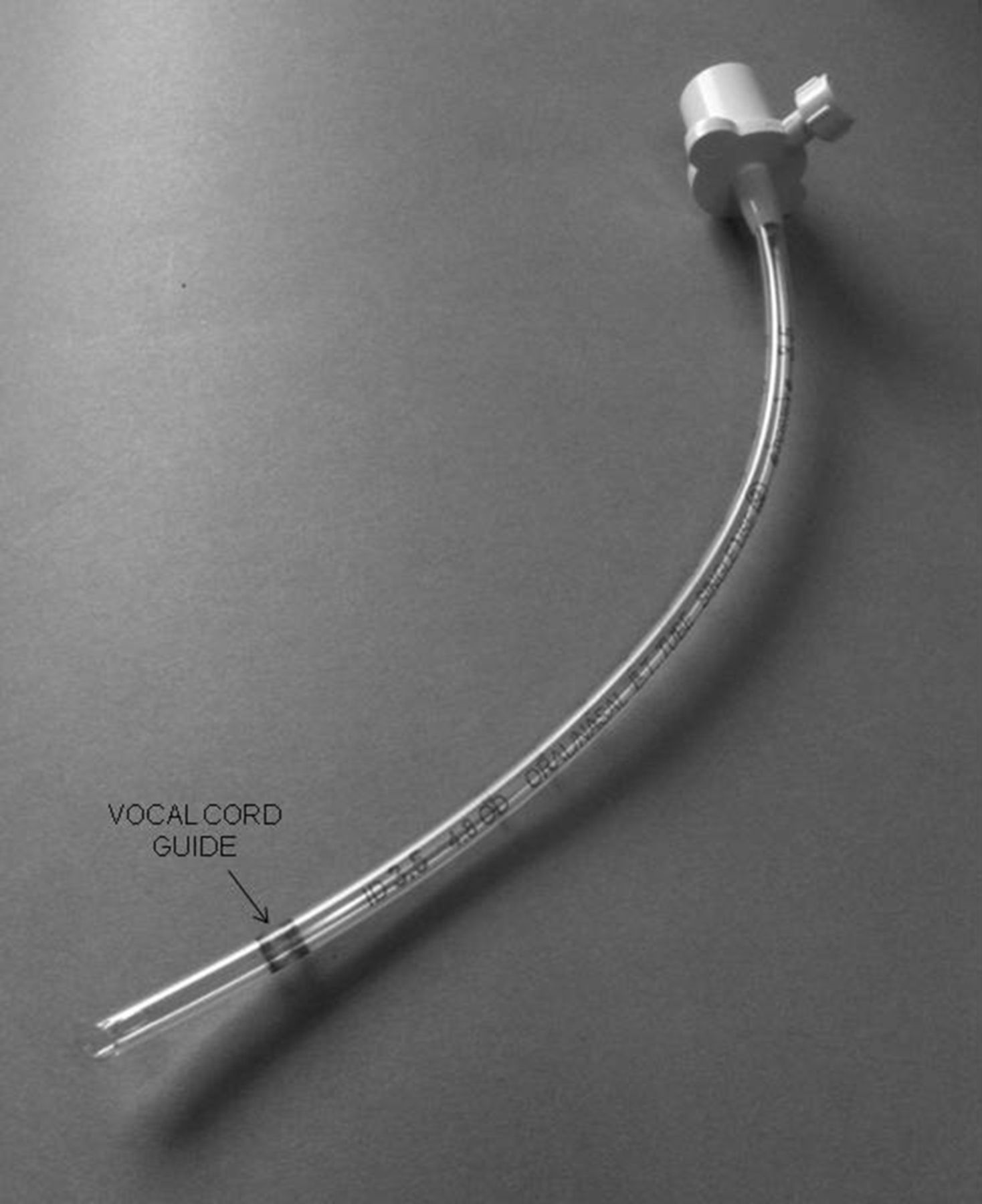
The decision to intubate was at the discretion of the treating doctor. All infants received analgesia and sedation before oral intubation was attempted; all infants received an opiate in addition to other medications, most commonly midazolam, atropine or suxamethonium. Intubation was performed using straight laryngoscope blades of size determined by their weight (<1 kg: 00; 1–2 kg: 0; and >2 kg: 1). All infants were intubated with ETTs (Portex, Smiths International Medical, Kent, UK; figure 1) of internal diameter determined by their weight (1 kg: 2.5; 1–2 kg: 3.0; and >2 kg: 3.5 mm). All ETTs were secured by the intubating doctors and nurse assistants using the lockable ETT holder supplied with the ETT.
Endotracheal tube (Portex, Smiths International Medical, Kent, UK) used in our study with vocal cord guide indicated.
When the decision to intubate was made, the intubating doctor selected the next envelope in the sequence from the appropriate box and estimated the depth of ETT insertion as directed by the group assignment.
For infants assigned to the ‘weight’ group, the intubating doctor recorded the infant’s current weight and the depth of insertion they calculated according to the formula [insertion depth (cm)=6 + wt (kg)] on the card. For infants whose weight at study entry was less than that at birth, their birth weight was used in this calculation. Doctors were instructed to secure the ETT at this depth. For infants assigned to the VCG group, doctors were instructed to advance the ETT until the VCG (figure 1) was visible at the vocal cords on direct laryngoscopy and secured at this depth. The intubating doctor recorded the depth at which they actually secured the ETT on the card indicating the group assignment for infants in both groups. They also recorded the number of unplanned extubations before a CXR was performed to determine ETT position.
An anteroposterior mobile CXR was then performed to confirm ETT tip position. The CXRs were performed by radiographers who were unaware of the infant’s group assignment. Radiographers were instructed to take the CXR with the head in a neutral position (ie, neck neither flexed nor extended) as is standard practice in our unit. If the attending doctors adjusted the ETT position based on the CXR, and they recorded how far they advanced or withdrew the ETT.
Outcome measures
The primary outcome of this study was correct position of the ETT tip on CXR performed after intubation. We determined that the ETT position was correct when the tip was between the upper border of T1 and lower border of T2. The primary outcome was determined by one consultant paediatric radiologist who was masked to group assignment.
We recorded the following secondary outcomes: number of accidental extubations prior to CXR, ETT repositioning after CXR, occurrence of pulmonary air leaks, duration of ventilation, oxygen therapy at 28 days and 36 weeks and death before hospital discharge.
Sample size estimation
In our previous study, we found that the ETT tip was correctly positioned in 25/49 infants.8 To demonstrate a reduction in the rate of incorrectly positioned ETTs from 50% to 25% (relative reduction of 50%) with the use of the VCG for the estimation of insertion depth, with 80% power with α=0.05, we estimated that we needed to recruit 116 infants.
Statistical analysis
We analysed data with SPSS V.20 using the ‘intention-to-treat’ principle. We compared the rate of the primary outcome and dichotomous secondary outcomes using Fisher’s exact test. We compared non-normally distributed continuous outcomes using an independent-samples median test. We considered p values <0.05 statistically significant.
Results
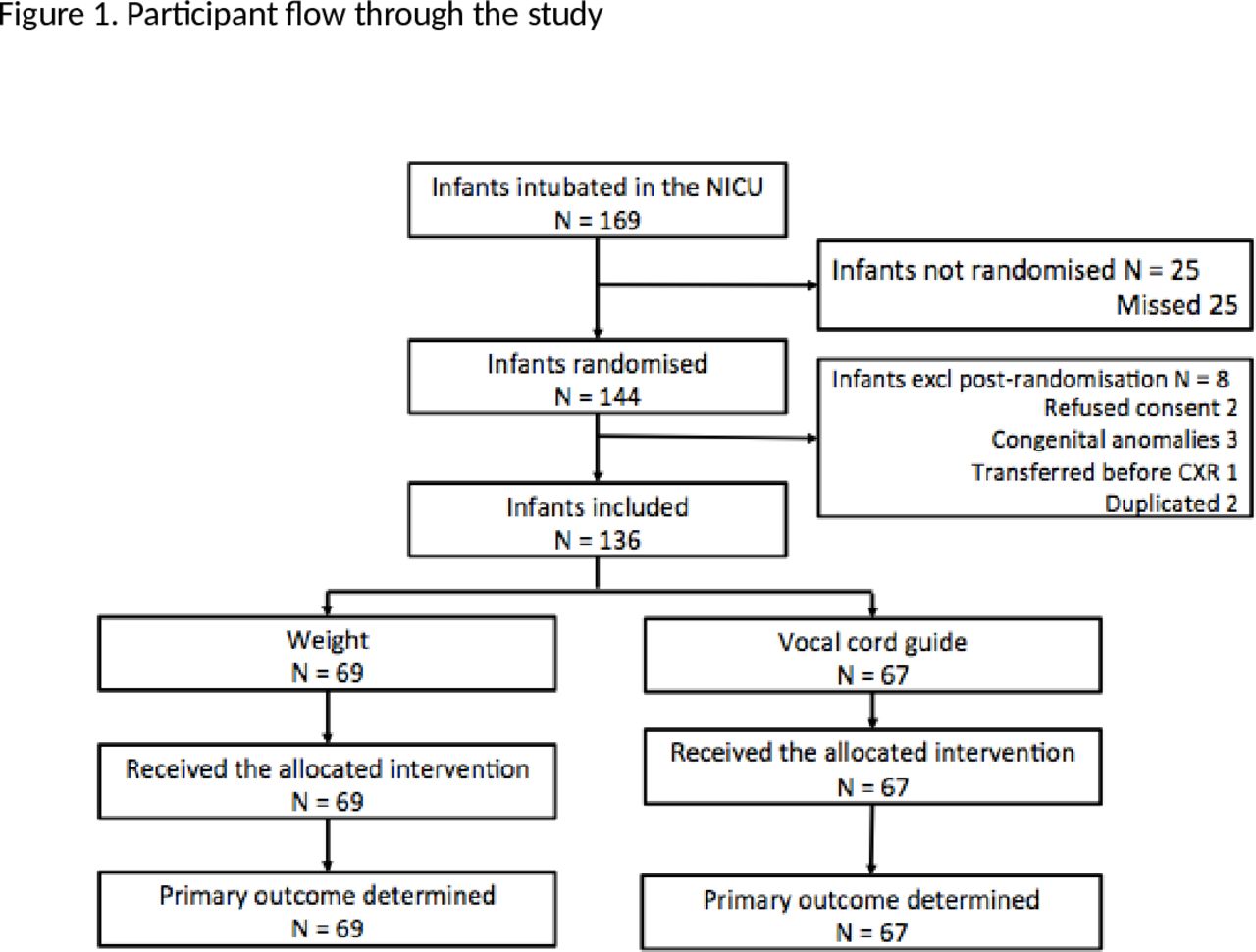
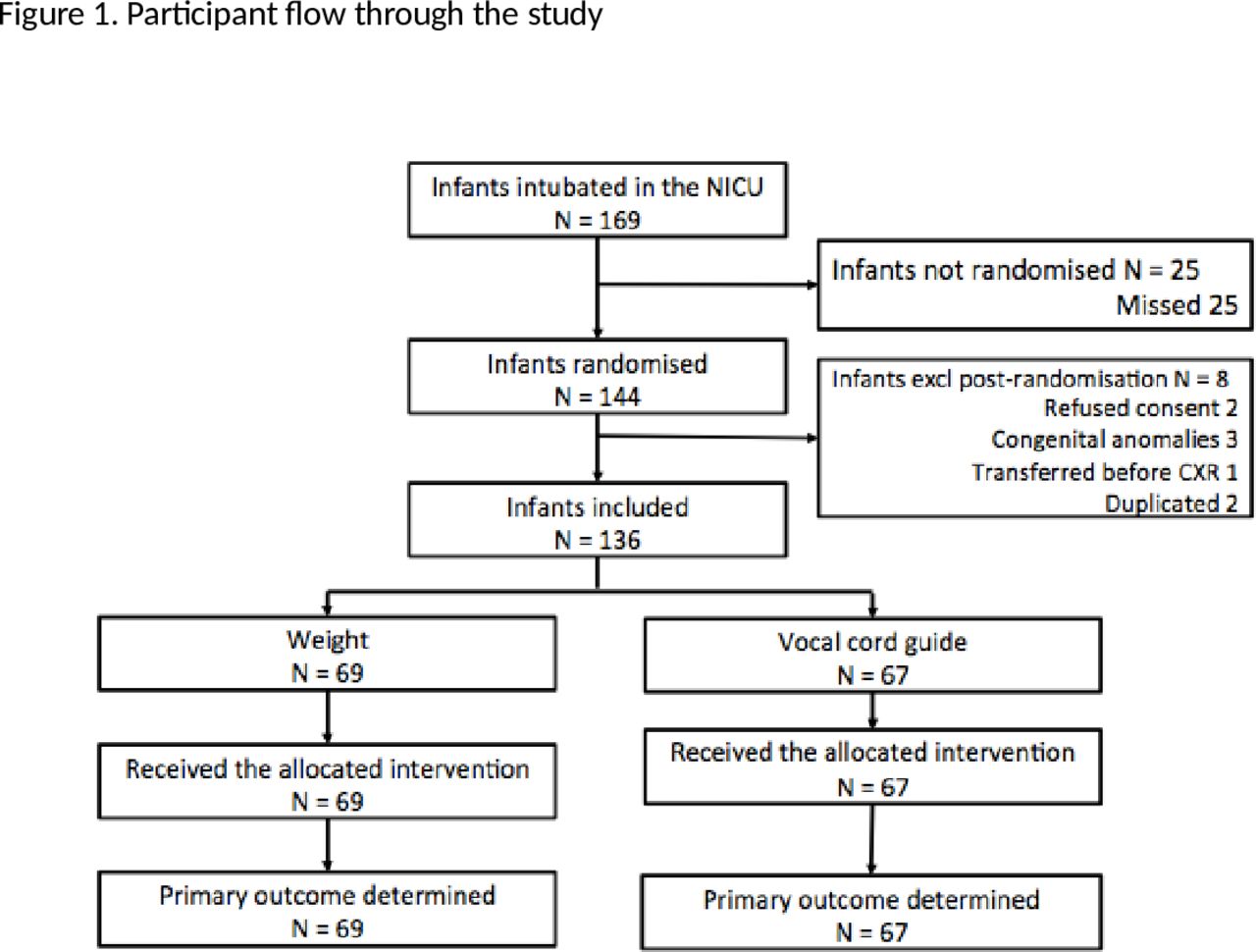
Between September 2013 and December 2015, 169 infants were intubated in NICU (figure 2). Twenty-five infants were not randomised by the intubating clinicians and so were not enrolled. Of the 144 randomised infants, eight were excluded; two families did not consent to involvement in the study, three were excluded due to the presence of congenital airway or lung anomalies, two were randomised in error having been previously enrolled in the study and one patient was transferred emergently to another hospital before CXR could be performed to determine the primary outcome.
Of the 136 infants included in the analysis, 69 were assigned to the weight group and 67 to the VCG group. All enrolled patients received the assigned intervention and had primary outcome data recorded. Patient characteristics at enrolment were similar for both groups (table 1). Though we did detect a difference in birth weight between the groups, it was not statistically significant, and the proportion of small for gestational age (birth weight <10th centile) infants did not differ between the groups (weight 16/69 (23%) vs 11/67 (16%), p=0.392, Fisher’s exact test). Of patients assigned to the weight group, 31/69 (45%) had their ETT secured at the estimated insertion depth. The median (IQR) absolute difference between the estimated insertion depth and the depth at which the ETT was secured was 0.1 (0.0, 0.2) cm for the 69 infants assigned to the ‘weight’ group overall and 0.2 (0.1, 0.4) cm for the 38 infants who did not have the ETT secured at the estimated insertion depth.
Patient characteristics at enrolment
We found no difference in the proportion of infants with correctly placed ETT tips between the groups (weight 30/69 (43%) vs VCG 27/67 (40%), p=0.731; table 2). Most of the incorrectly positioned ETTs were too low (69/79, 87%). There were three accidental extubations before CXR. All occurred in infants assigned to the VCG group. The rate of adjustment of ETT position after CXR was not different between the groups (weight 31/69 (45%) vs VCG 32/67 (48%), p=0.864).
Outcome data
Infants assigned to the weight group were more likely to receive oxygen therapy at 36 weeks (weight 31/69 (45%) vs VCG 15/67 (22%), p=0.03). We did not detect statistically significant differences in pulmonary air leaks or in death before hospital discharge between the groups.
Discussion
All infants enrolled in our study were intubated with the same model of ETT. We previously found that the position and design of the VCG may vary between models of ETT, with relatively large differences in position (up to 21 mm) between some models.14 This limits the applicability of our findings to contexts where other models of ETT are used. In common with most ETTs, the tubes we used in this study have markings at 1 cm intervals from the tip. Clinicians recorded the estimated and secured ETT insertion depth to one decimal place (eg, 6.5 cm). Such measurements are by definition an estimate. We enrolled more participants to our study than we planned as we did not appreciate that we had reached our target sample at the time. We included all participants that were randomised for whom we had consent for their inclusion in our study.
{kind=link}
{kind=link}
Participant flow through the study. CXR, chest X-ray; NICU, neonatal intensive care unit.
In keeping with the results of our previous study8 and those of other authors,5–7 9 15 we found that ETTs were frequently incorrectly positioned and that they were most often inserted too far. Most infants in our study were intubated by doctors in training who had <1 year experience of intubating newborns; however, previous studies have identified that ETTs are frequently incorrectly positioned by all doctors regardless of their level of experience.16 The ETT was recorded as being secured at more than the estimated insertion depth in almost half of the infants assigned to the weight group. Seventeen of the 31 (55%) ETTs in the weight group that were secured at the estimated depth were correctly placed on CXR. If all infants assigned to the weight group had their ETTs secured at the estimated depth and the proportion of ETTs that were correctly placed remained the same, then 38/69 (55%) ETTs would have been correctly placed on CXR. This would have resulted in a greater number of infants with correctly placed ETTs; however, the difference between the groups would not have been significantly different (weight 38/69 (55) vs VCG 27/67 (40), p=0.062, Fisher’s exact test). We speculate that clinicians may insert ETTs further than necessary in an attempt to minimise the risk of accidental extubation. Method of estimation of ETT insertion depth may have little effect on this phenomenon.
Infants assigned to the weight group were more likely to receive oxygen therapy at 36 weeks (weight 26/69 (38%) vs VCG 13/69 (19%), p=0.003). This is a secondary outcome for which our study was not designed to find differences between the groups. We believe that this is a chance finding that is not clinically relevant.
The principal weakness of our study is that neither the intubating clinicians nor the nurse assistants were masked to the infants’ group assignment. This may have led to bias in how they secured ETTs and whether the ETT position was adjusted after X-ray. However, all enrolled infants had the primary outcome measured, and it was determined by one consultant paediatric radiologist who was masked to group assignment. We believe this reduced ascertainment bias and bias in outcome assessment. Another potential weakness is the difficulty in verifying the true ETT position in the VCG group. Clinicians were instructed to position the VCG at the level of the cords and secure the ETT at that depth. However, we did not have a method of verification (eg, third party observation of video laryngoscopy) available for all infants. While we think this is a limitation of our study, we believe that it reflects real world practice with regards to neonatal endotracheal intubation.
Other methods to improve the accuracy of ETT tip placement in newborns have been proposed, including digital palpation17 18 and confirmation of ETT position with point-of-care ultrasound.19 Studies of these or other methods to improve ETT positioning in intubated newborns are warranted.
Conclusion
Estimating ETT insertion depth using the VCG rather than a weight-based formula did not result in more correctly positioned ETTs in newborns.
Acknowledgments
We would like to thank the participants and their parents, the nurses who provided their care and assisted at intubation and the clinicians who assisted in recruitment.
References
Footnotes
Contributors CPFO conceived of and designed the trial, analysed the data and edited the draft manuscript. IG wrote and revised the trial manuscript and was primarily responsible for patient enrolment, trial implementation and data collection. Trial materials and data collection tools were designed by CPFO and IG. Primary outcomes were determined by EL who also reviewed the manuscript. AS was responsible for trial implementation and data collection from January 2015 onwards and reviewed the manuscript. MCM analysed data and reviewed the manuscript. ARG and MC oversaw patient enrolment, staff engagement and monitored data collection.
Competing interests None declared.
Ethics approval Research Ethics Committee, National Maternity Hospital, Dublin.
Provenance and peer review Not commissioned; externally peer reviewed.
Author note This trial was registered at www.isrctn.com (ISRCTN39654846). The authors applied for registration on 3 September 2013, before the first participant was enrolled on 27 September 2013. No substantive changes were made to the original application before the trial registration number was assigned on 14 October 2013. Four participants were enrolled in this study between 27 September 2013 and 14 October 2013.
Presented at Presented at the European Academy of Paediatric Societies meeting in Geneva Switzerland on 24 October 2016.
Linked Articles
- Fantoms