Article Text

Abstract
Background Basic life support guidelines recommend placing spontaneously breathing children and adults on their side. Though the majority of preterm newborns breathe spontaneously, they are routinely placed on their back after birth. We hypothesised that they would breathe more effectively when placed on their side.
Objective To determine whether preterm newborns placed on their left side at birth, compared with those placed on their back, have higher preductal oxygen saturation (SpO2) at 5 min of life.
Design/methods We randomised infants <32 weeks to be placed on their back or on their left side immediately after birth. Respiratory support was given with a T-piece and face mask with initial fraction of inspired oxygen (FiO2) of 0.3. The FiO2 was increased if SpO2 was <70% at 5 min.
Results We enrolled 87 infants, 41 randomised to back and 46 to left side. The groups were well matched for demographic variables. Fourteen (6 back and 8 left side) infants did not receive respiratory support in the first 5 min. The mean (SD) SpO2 was not different between the groups (back 72 (23) % versus left side 71 (24) %, p=0.956). We observed no adverse effects of placing infants on their side and found no differences in secondary outcomes between the groups.
Conclusions Preterm infants on their left side did not have higher SpO2 at 5 min of life. Placing preterm infants on their side at birth is feasible and appears to be a reasonable alternative to placing them on their back.
Trial registration number ISRCTN74486341.
- Neonatology
- Resuscitation
- Prematurity
Statistics from Altmetric.com
What is already known on this topic
Adult and paediatric basic life support guidelines recommend placing spontaneously breathing patients on their sides.
Most newborn premature infants breathe spontaneously but are routinely placed on their backs at birth.
What this study adds
We found no difference between oxygen saturations at 5 min of life in preterm infants placed on their sides or on their backs.
Placing preterm infants on their sides at birth is a feasible and reasonable alternative to placing them on their backs.
Introduction
The International Liaison Committee on Resuscitation (ILCOR) makes recommendations for basic and advanced resuscitation in all age groups. ILCOR evaluates the evidence to support practice every 5 years and updates its recommendations accordingly. Basic life support guidelines for children1 and adults2 recommend placing spontaneously breathing patients in the recovery position (ie, on their side) as it helps to maintain a patent airway. The first recommendations for newborns made in 1999 advised placing infants either on their back or their side,3 as did the guidelines published in 2000.4 Later iterations of the guidelines did not explicitly state how infants should be positioned, but implied that they should be placed on their backs.5 ,6 Pictures in neonatal resuscitation textbooks usually show infants placed on their backs.7
Most extremely preterm infants breathe spontaneously at birth;8 however, they frequently have respiratory distress and the majority receives breathing support with continuous positive airway pressure (CPAP) and/or positive pressure ventilation (PPV) after birth. Airway obstruction is common during mask PPV in preterm infants placed on their backs9 ,10 and considerable pressure may be applied to an infant's head when delivering face mask ventilation in this position.11 Spontaneously breathing infants with mild respiratory distress who are placed on their side in the neonatal intensive care unit (NICU) have improved oxygenation and tidal volumes compared with infants placed on their back.12 ,13 Animal studies suggest that lung aeration after birth is affected by volume and pressure of inspired gas, and by body position.14
In a retrospective study of video recordings of newly born term infants in the delivery room (DR), Kostantelos found a trend to higher oxygen saturation (SpO2) and less agitation in infants placed on their side compared with their back.15 The effect of position on oxygenation of newborns in the DR has not previously been evaluated in a randomised controlled trial. We hypothesised that infants at birth would breathe more effectively if placed on their left side compared with on their back. We chose the left side so that infants could be immediately placed on their side while a pulse oximetry sensor was being applied to their right upper limb to measure preductal SpO2.
Methods
We performed this study in the DRs at three hospitals with tertiary level NICUs, the National Maternity Hospital, Dublin, Ireland (NMH); Leiden University Medical Centre, Leiden, The Netherlands (LUMC); and the Royal Women's Hospital, Melbourne, Australia (RWH). Infants were eligible for inclusion if they were born before 32 completed weeks of gestation calculated by best obstetric estimate (first trimester ultrasound or based on the mother's last menstrual period), but were excluded if they had major congenital anomalies. Infants born at any time of the day were enrolled at NMH and LUMC. Infants were enrolled at RWH only when dedicated research staff was available (09.00–17.00, Monday–Friday).
Written consent to enrol infants in the study was obtained from parents(s)/guardian(s) before birth when circumstances allowed. In emergency situations where it was not possible to obtain informed consent antenatally, infants could be enrolled with a waiver of consent. In these instances, parents(s)/guardian(s) were approached as soon as practicable after birth and their consent was sought for their infant(s) to continue in the study. If parents refused postnatally, all study data were destroyed. The study was approved by the Ethics Committees at each of the participating institutions and registered before the first patient was enrolled (ISRCTN74486341).
Infants were randomly assigned to be placed on their back or left side in a 1:1 ratio. Infants of multiple pregnancies were randomised as individuals. We stratified the randomisation by participating centre. We also stratified the randomisation according to gestational age (<28 weeks, 28–31+6 weeks) and mode of delivery (vaginal delivery, caesarean section) as both factors are known to affect oxygenation in the minutes after birth.16 ,17 We generated the group assignment schedule in blocks of four using a random number table. We wrote the group assignment on cards that we folded and placed in sequentially numbered, sealed, opaque envelopes. We placed the envelopes in four separate boxes (vaginal delivery, <28 weeks; vaginal delivery, 28–31+6 weeks; caesarean section, <28 weeks; caesarean section, 28–31+6 weeks) that were kept in the NICU. When delivery of an eligible infant was anticipated, the clinician attending the birth brought the next envelope in the sequence from the appropriate box to the DR and opened it just before birth. Neither caregivers nor outcome assessors were masked to group assignment.
Births of infants enrolled in the study were attended by at least two doctors (a consultant and/or fellow and resident) and one neonatal nurse. No specific training for treating infants on their left side was given to caregivers at the participating centres. The timer on the resuscitation table (Cosy Cot, Fisher & Paykel Healthcare, Auckland, New Zealand) was started on complete delivery of the infant. In keeping with standard practice at each participating centre at the time the study commenced, the umbilical cord was clamped immediately after birth in all infants. Infants were brought to the resuscitation table and placed in a polyethylene bag under radiant heat. Once in the polyethylene bag, infants were placed on the resuscitation table in their allocated position, either on their back or on their left side. All other aspects of DR treatment were in accordance with local hospital protocols and ILCOR recommendations. A pulse oximetry sensor was placed around their right wrist and connected to a pulse oximeter. For all infants enrolled at RWH and LUMC, and for the majority of infants enrolled at NMH, the Masimo Radical pulse oximeter (Masimo Corporation, Irvine, California, USA) was used. This pulse oximeter was set to capture data with maximal sensitivity and average it over 2 s intervals. A minority of infants enrolled at NMH were monitored with the Nellcor Oximax pulse oximeter (Covidien, Boulder, Colorado, USA).
Infants who had clinical signs of respiratory distress and/or bradycardia received respiratory support (CPAP and/or PPV). Respiratory support was given to infants in their allocated position (ie, on their back or on their side) in both groups using a T-piece device (Neopuff Infant Resuscitator, Fisher & Paykel Healthcare, Auckland, New Zealand) with a round silicone face mask (Fisher & Paykel Healthcare, Auckland, New Zealand or Laerdal, Stavanger, Norway) of appropriate size. Clinical staff were instructed to set the Neopuff to give PPV a peak inflating pressure of 25 cmH2O and a positive end-expiratory pressure of 5 cmH2O with a fraction of inspired oxygen (FiO2) of 0.30 before delivery; and not to alter the FiO2 before 5 min of age. If the infant's SpO2 was less than 70% at 5 min of age, the FiO2 was to be increased by 0.10 every minute until the SpO2 was greater than 70%, aiming for SpO2 ≥90% at 10 min of age. Infants who had persistent bradycardia or apnoea despite mask PPV were intubated for PPV. Infants in both groups were placed on their back for intubation and external cardiac massage (ECM). Once these interventions were completed (ie, endotracheal tube secured in position, ECM stopped), infants were placed in their assigned position (ie, remained on their back or returned to their left side).
Outcome assessment
The primary outcome of our study was SpO2 at 5 min of life. One person attending the birth recorded outcome data in the DR. At NMH and LUMC, this was either a member of the research team if available or a member of the clinical staff. At RWH data were recorded by a member of the research team. This individual recorded whether or not infants received respiratory support in the DR; and, if so, the starting FiO2, and the maximum FiO2 used before 5 min and at any time in the DR. They recorded the SpO2 and heart rate (HR) displayed on the pulse oximeter at 5 min and 10 min of life determined from the timer on the resuscitation table. They also recorded the time at which the infant's SpO2 first reached 90%. When DR stabilisation was complete, infants were transported to the NICU for ongoing care. On leaving the resuscitation table infants were positioned at the discretion of the treating clinicians. We determined maternal characteristics and infants’ outcomes beyond the DR from the medical records.
Sample size estimation and power calculation
The primary outcome of our study was preductal SpO2 at 5 min of life. In a previous randomised trial at NMH, we found that the mean (SD) SpO2 at 5 min of life in infants <31 weeks placed on their back who received respiratory support starting with FiO2 of 0.3 was 78 (15) %.18 To demonstrate an increase in the mean (SD) SpO2 at 5 min to 88 (15) % with 80% power and α=0.05, we estimated that we would need to enrol 74 infants (37 in each group) to our study. To allow for a failure to obtain oximetry data by 5 min in approximately 10% of enrolled infants, we aimed to enrol 82 infants to our study.
Data were analysed using the intention-to-treat principle using SPSS V.20 software (IBM Corp, Armonk, New York, USA). Continuous data were described using mean (SD) when normally distributed and median (IQR) when the distribution was skewed; and compared using parametrical tests (eg, independent-samples t test). Dichotomous data were expressed as proportions and compared using non-parametrical tests (eg, Fisher's exact test).
Results
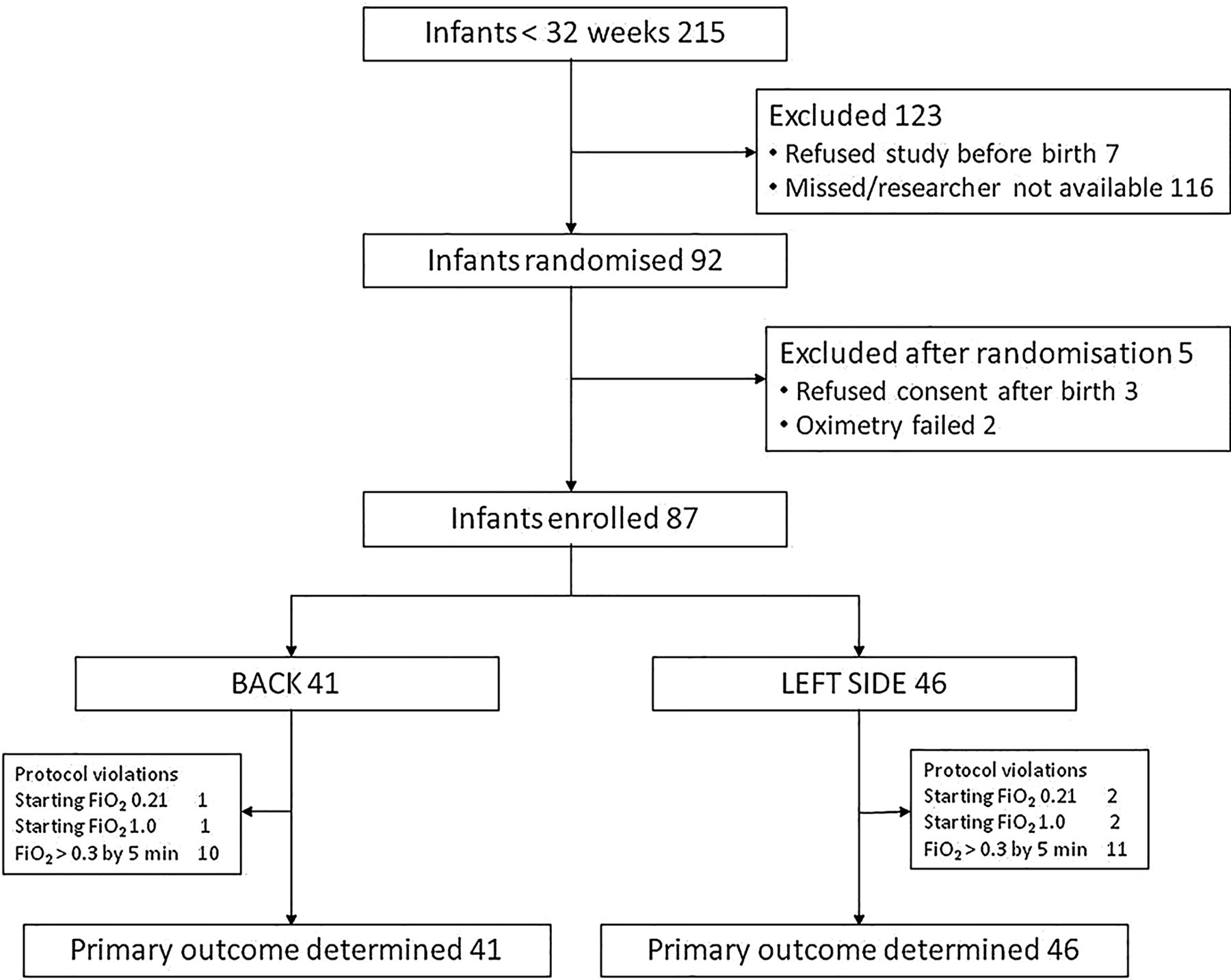
We enrolled 87 infants (57 at the NMH; 16 at RWH; and 14 at LUMC) between 5 October 2012 and 24 July 2013. Consent was obtained to enrol 54 infants antenatally. Thirty-eight infants were enrolled with a waiver of consent; consent to continue in the study was not obtained from the parent(s)/guardian(s) of three infants (see figure 1).

{kind=link}
Patient recruitment.
Forty-one infants were randomised to being placed on their back and 46 on their left side. The groups were well matched for demographic variables (table 1). Forty-eight infants were singletons (22 left side, 26 back), 36 were twins (22 left side, 16 back) and 3 were triplets (2 left side, 1 back).
Patient characteristics at enrolment
Fourteen (6 back, 8 left side) infants did not receive respiratory support in the first 5 min. No caregivers reported difficulty in providing mask CPAP or PPV to infants on their left side. Protocol violations regarding oxygen use during respiratory support in the first 5 min occurred at each participating centre. One back infant and two left side infants received a starting FiO2 0.21, and one back and two left side infants received a starting FiO2 1.0. The remaining infants (33 back, 34 left side) received a starting FiO2 0.3. The maximum FiO2 received by infants within 5 min was >0.3 in 10 back and 11 left side infants, among them were the 2 infants (1 in each group) who received chest compressions in the first 5 min. The remaining infants (25 back, 27 left side) received a maximum FiO2 of 0.3 in the first 5 min of life.
We found no difference between the groups in the primary outcome—the mean (SD) SpO2 at 5 min of life was 72 (23) % for back infants and 71 (24) % for left side infants (p=0.956).
We found no differences between the groups in the secondary outcomes mean HR at 5 min, in the mean SpO2 or HR at 10 min or in the time to reach SpO2 of 90% (table 2). Infants in the back group took longer to wean from supplemental oxygen (median (IQR) day of life—back 12 (1, 55) versus left side 1 (0, 46), p=0.018). We found no differences in the other secondary outcomes we measured (table 2). No adverse effects of placing infants on their left side were reported. There were no deaths in the DR in either group, and the proportion of infants who died before hospital discharge was not different between the groups.
Patient outcomes
Discussion
Human and animal studies suggest that several factors are likely to impact on lung aeration including gestation, mode of delivery, position and inflation pressures.12–14 ,17 SpO2 is an indirect measure of aeration and ventilation and is routinely measured in the DR. The mean SpO2 at 5 min of life in infants in this study was lower than the values in our previous study which we used to estimate our sample size.18 This may be partly explained by the greater proportion of infants in this study (14/87, 16%) who did not receive respiratory support and supplemental oxygen in the DR compared with our previous study (1/144, 1%).18 The mean SpO2 at 5 min in this study was comparable to that of earlier studies of infants who had their umbilical cord clamped immediately after birth.16 A cohort of infants born vaginally at term who had delayed cord clamping and immediate skin-to-skin contact had higher SpO2 in the 1st minutes of life compared with a cohort of infants who had immediate cord clamping that included preterm and term infants born vaginally and delivered by caesarean section.19 While we believe that the mean SpO2 at 5 min in both groups could well have been be higher if the infants in our study had had delayed cord clamping, we don't know whether SpO2 at 5 min would differ according to body position.
A minority of babies were monitored with the Nellcor Oximax pulse oximeter instead of the Masimo Radical pulse oximeter which could lead to higher SpO2 readings,20 however Masimo Radical use was not different between the two groups. We considered using a real-time data acquisition system to record the oximetry data in the DR to reduce the potential for errors inherent with observers recording the outcomes; however, this was not available at all centres. Our study was powered to detect a 10% increase in SpO2 at 5 min of life in infants placed on the left side. Though we found no difference between the groups, we cannot exclude smaller differences in SpO2 at 5 min on the basis of our study. We did detect a statistically significant difference in the number of days taken to wean from supplemental oxygen between the groups. This was a secondary outcome, in which our study was not designed or adequately powered to detect differences between the groups. We find it difficult to attribute the difference we found to the intervention and we consider it likely to be a chance finding. There were no differences in other secondary outcomes between the two groups. Neonatal mortality and morbidity outcomes are comparable to those seen in international tertiary neonatal units and support the generalisability of our results.21
From a retrospective study of video recordings of term newborns, Konstantelos reported that infants placed on their side had less agitation and a trend towards better oxygenation compared with infants placed on their back.15 The groups were of unequal size and their position was not randomly assigned. We did not record agitation, as this study was published after ours had started. As we did not study term infants, we can neither support nor refute Konstantelos’ findings.
We enrolled many infants to our study using a waiver of consent. This a well recognised approach to the difficulties encountered in the enrolment of human adults, children and infants to studies of emergency procedures and is in accordance with guidelines issued by the UK Medical Research Council22 and Article 19 of the ‘Additional protocol on the Convention of Human Rights and Biomedicine on Biomedical Research’ affirmed by the Council of Europe in 2005. The rate of refusal to participate in the study following enrolment with the waiver was low and we did not experience conflict with the families who refused to participate, either before or after their infant's birth. The antenatal refusal rate (parent(s) of 7/61 (11%) infants that were approached) was comparable to the postnatal refusal rate (parent(s) of 3/38 (8%) infants enrolled). The slightly higher rate of antenatal refusal may be a chance finding. However, we speculate that it might also reflect higher parental stress levels antenatally and a reluctance to take what they may perceive as a risk to their child, in deviating from the attending doctor's preferred position for infants during neonatal resuscitation. Parents often have more time to consider their infant’s participation in research studies postnatally. By this stage, most have formed a positive relationship with the treating clinicians, which may in turn contribute to a higher consent rate.
We believe it is reasonable to place premature newborn infants either on their left side or on their back immediately after birth as well as in the NICU; this may be done at the discretion and preference of the treating clinician.
References
Footnotes
Contributors The conception and design of the study was performed by ES and CPFO’D. LKM, EAK assisted with study design and patient recruitment in NMH. JAD, JJVV, ABTP, PGD performed patient recruitment and study data collection in LUMC and RWH. Data were analysed and the manuscript written by ES and CPFO’D.
Competing interests None declared.
Ethics approval National Maternity Hospital Ethics Committee, Dublin; Ethics Committee (CEM) at Leiden University Medical Centre; Human Research Ethics Committee, Royal Women's Hospital, Melbourne.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement Unpublished secondary data are available upon email application to CPFO'D.
Linked Articles
- Fantoms