Article Text

Abstract
Objective To test the applicability of existing retinopathy of prematurity (ROP) guidelines on Iranian patients and to develop novel ROP screening criteria in Iran.
Methods Both eyes of 1932 infants born ≤37 weeks of gestation and/or weighting ≤3000 g were included in this prospective cohort study that was conducted across nine neonatal intensive care units and a tertiary eye hospital ROP clinic. The patients were examined for ROP and the need for treatment (type 1 ROP or worse). All the patients were screened 4 weeks after birth or at 31 weeks of postmenstrual age, whichever was later. The patients were followed until retinal vascularisation was completed or the patients reached 50 weeks of gestational age (GA) without prethreshold ROP. A receiver operating characteristic curve was used to determine the best screening criteria for ROP. Screening criteria from other countries were applied to our patient data to determine their ability to appropriately detect ROP.
Main outcome measure Patients with ROP requiring treatment.
Results The mean GA±SD and birth weight (BW)±SD of the screened patients were 32±2.7 weeks and 1713±516 g, respectively. Using criteria of GA≤32 weeks or BW ≤2000 yielded sensitivity and specificity of 100% and 26.7%, respectively, for treatment requiring ROP regardless of clinical comorbidities. Using screening recommendations of American Academy of Pediatrics would miss 25.4% of ROP and 8.4%ROP requiring treatment in our cohort.
Conclusions Other countries screening recommendations would result in a significant amount of missed cases of treatment requiring ROP when applied to Iran. As a result, we have proposed new guidelines for premature babies in Iran.
- Ophthalmology
- Screening
- Retinopathy of Prematurity
- Infant, Iran, neonatal, prematurity, pediatrics.
Statistics from Altmetric.com
What is already known on this topic
Retinopathy of prematurity (ROP) appears in more mature babies in low/middle-income countries. It is highly recommended that every country develop its own ROP screening criteria.
What this study adds
By following the American Academy of Pediatrics guidelines (gestational age (GA) ≤30 weeks or birth weight (BW) ≤1500 g), 8.4% of Iranian ROP babies who required treatment would have been missed. Our revised screening guidelines, GA ≤32 weeks or BW ≤2000 g, result in 100% sensitivity for ROP requiring treatment in Iran.
Introduction
Retinopathy of prematurity (ROP) is the leading cause of avoidable blindness in premature infants.1 Blindness from ROP is an increasing problem in the low/middle-income countries resulting in the ‘third epidemic’.2 The proportion of blindness due to ROP varies greatly among countries and is influenced by the nenonatal care as well as the availability of effective screening and treatment programmes.3 Timely screening and treatment is critical to reducing unfavourable outcomes including blindness.4
Severe ROP is increasingly seen in more mature infants in low/middle-income countries, especially when compared with their counterparts in developed countries. It is recommended that each country develops and employs its own specific screening criteria appropriate for its local population.4 The latest American Academy of Pediatrics (AAP) screening guidelines for ROP recommends mandatory screening for infants with birth weights (BWs) ≤1500 g or gestational ages (GAs) ≤30 weeks.5 These guidelines have been shown to be inadequate for screening in low/middle-income countries.6–8
To date no screening criteria has been published for Iran. The aim of the present study was to evaluate the applicability of current different international ROP screening guidelines, including those of the AAP, and to develop ROP screening criteria that can provide a safe and efficient model for identifying babies who require ROP treatment.
Methods
Institutional review board/ethics committee approval was obtained from the Farabi Eye Hospital. The study protocol adhered to the tenets of the Declaration of Helsinki. Informed consent was obtained from the parents or guardians of the babies enrolled in the study. Patients were screened at nine neonatal intensive care units (NICU) in Tehran or in the Farabi Eye Hospital ROP Clinic (the largest ROP centre in Iran) after being referred from outside hospitals/NICUs in Iran between November 2012 and November 2013. Infants born at ≤37th week of gestation and/or weighting ≤3000 were initially screened at the 31st week of GA or 4 weeks after birth, whichever was later. The location and severity of ROP was recorded for each infant according to the International Classification of ROP.9 The patients were examined by experts in ROP screening (AF, RR, MRE, RK and AK).
Nearly half of the patients were screened in NICUs and the remainder were referred on an outpatient basis for evaluation. Depending on the results of the initial fundal examination, the next examination was performed every 2–21 days until one of the following criteria for cessation was met:(1) zone III retinal vascularisation attained without previous zone I or II ROP if the patient was more than 35 weeks of GA or (2) full retinal vascularisation was observed or (3) the patient reached 50 weeks postmenstrual age and no prethreshold disease (defined as stage 3 ROP in zone II or any ROP in zone I) or worse ROP was present.5
The need for treatment was based on the early treatment of ROP (ETROP) study and was confirmed by at least two of the experienced ophthalmologists mentioned above. The ETROP trial recommended considering treatment for an eye with any of the following criteria of type 1 ROP:10
Zone I, any stage ROP with plus disease
Zone I, stage 3 ROP with or without plus disease
Zone II, stage 2 or 3 ROP with plus disease
A receiver operating characteristic (ROC) curve was used to identify the best screening criteria for identifying patients with ROP requiring treatment. The ROC curve plots true positive rate (or sensitivity) against false positive rate (or 1-specificity) at different threshold settings. BW and GA thresholds were combined to form many sets of criteria for the ROC curve. Sensitivity and specificity were determined for each threshold separately. The scenario with the lowest BW and GA that achieved 100% sensitivity was considered the best. To compare the applicability of different national screening criteria in the world with our population, criteria from Turkey, the USA, the UK, Latin America and China were applied to our data. We highlighted these regions because they represent criteria used in both the developed and low/middle-income countries, the latter of which mirrors the situation in Iran. The sensitivity and specificity using these criteria were assessed in our population, and the frequency of missed cases of ROP when these criteria were applied to our cohort is reported.
Mean GA and BW were compared between the no-ROP and ROP group as well as between patients with ROP who did and did not require treatment using a t-test for statistical significance.
Results
One thousand nine hundred and thirty-two infants with either a BW ≤3000 g and/or GA of ≤37 weeks were screened. The mean age±SD of examined patients was 32±2.7 weeks (range: 24–37 weeks).The mean BW±SD of screened patients was 1713±516 g (range 600–3000 g). Table 1 provides a comparison between babies who had and did not have ROP and who did and did not require treatment based on GA and BW.
Comparison of mean gestational age (GA) and birth weight (BW) of patients with and without retinopathy of prematurity (ROP) and those who did and did not require treatment
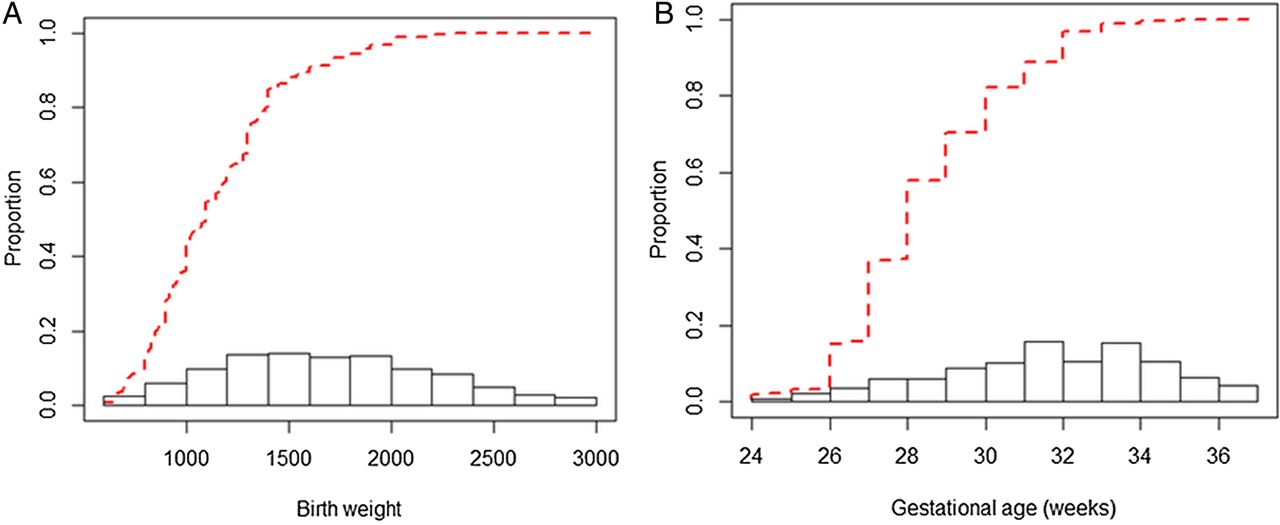
Figure 1 provides the cumulative proportion of affected babies with ROP who required treatment when considering their BW (figure 1A) and GA (figure 1B) separately.
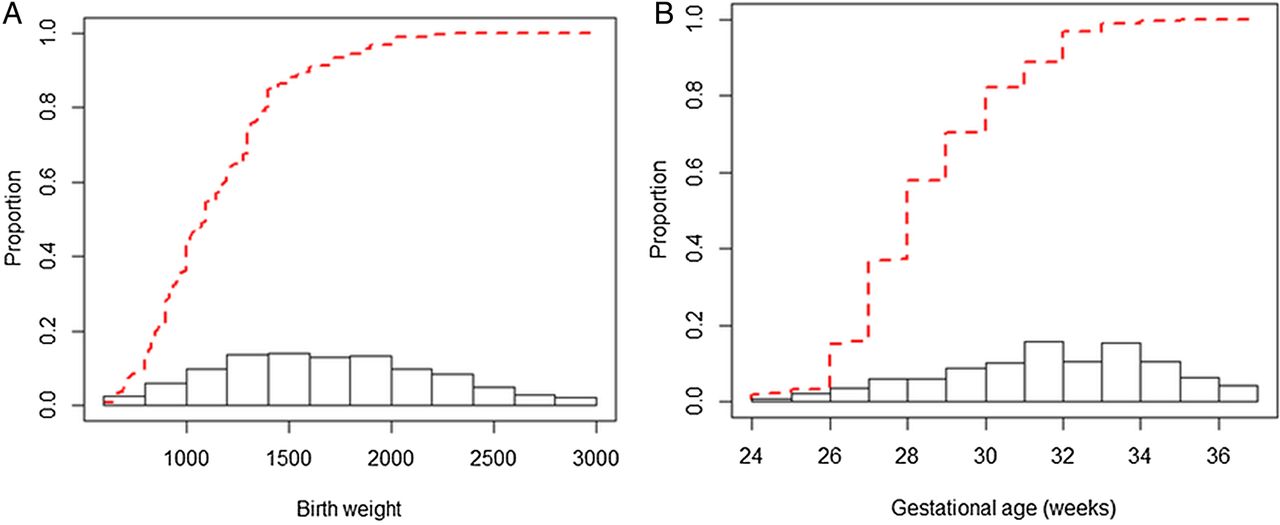
Histogram of distribution of retinopathy of prematurity at different birth weight (A) and gestational age (B) with cumulative proportion infants requiring treatment represented by the dashed red line.
Systemic factors available for review were compared between patients with and without ROP. The presence of intubation, twin birth, transfusion, acute respiratory distress syndrome, intraventricular haemorrhage, sepsis, phototherapy, small GA and/or oxygen therapy were compared between patients with and without ROP (table 2).
Comparison of systemic risk factors in ROP positive and no-ROP groups
ROP was diagnosed in both eyes of 570 (30.0%, 95% CI 28.0% to 32.2%) patients. and among these 161(8.3% of all patients) required bilateral treatment. Stage 4 or 5 ROP was seen in 1.4% of patients with ROP while lower stages (1, 2 or 3) were seen in 98.6% of patients with ROP.
Using ROC curve, the area under the curve (AUC) for ROP detection was 0.815 (95% CI 0.794 to 0.836) and 0.778 (95% CI 0.775 to 0.801) for GA and BW, respectively. Also, the AUC for ROP requiring treatment was 0.877 (95% CI 0.853 to 0.902) for GA and 0.851 (95% CI 0.822 to 0.888) for BW.
Considering only one factor, a screening threshold of BW ≤2300 g or GA≤35 weeks would result in 100% sensitivity; however, using only one of these factors would result in screening of more patients than the health system could bear and would not be cost-effective. To find an appropriate screening threshold, we considered both GA and BW and defined several potential screening criteria for which sensitivity and specificity were calculated (figure 2). Among these possibilities, a threshold of GA≤32 weeks and/or BW ≤2000 g yielded a sensitivity of 93.9% and specificity of 32.3% for identifying any ROP and a sensitivity of 100% and specificity of 26.7% for identifying patients with ROP who required treatment. This criterion was considered the best option because it possessed a 100% sensitivity for identifying patients with ROP requiring treatment (figure 2).

{kind=link}
{kind=link}
Sensitivity and specificity for retinopathy of prematurity (ROP) diagnosis and treatment requiring ROP at different gestational age (GA) and birth weight (BW) thresholds using receiver operating characteristic curves.
Following screening recommendations of AAP, 25.4% of ROP would be missed as would 8.4% of ROP requiring treatment. Conversely, using Turkish criteria 1.9% of ROP would be missed without any cases of ROP requiring treatment being missed. Table 3 provides the performance of different national guidelines when applied to Iranian patients.
Comparison of different national ROP screening guidelines when applied to our Iranian cohort using receiver operating characteristic curves
Discussion
ROP is a significant cause of blindness that requires constantly evolving approaches to reduce ocular morbidity. In this study, ROP was diagnosed in both eyes of 30% of patients (n=570) and 8.3% of patients (n=161) requiring treatment. These results are consistent with findings from studies in several low/middle-income countries (defined as countries with human development index rankings between 31 and 100).3 ROP incidences have been reported to be 34.4% in Egypt (152 patients),11 34% in Oman (73 patients),12 47% in India (165 patients) 13 and 56% in Saudi Arabia (174 patients).14 An earlier study from 2003–2007 in Iran identified an incidence of 34.5%.15
In our incidence of ROP treatment was similar to the 9.8% of Egyptian patients requiring treatment.11 In comparison, 5% of infants examined in the USA, UK and Canada require treatment.16–18
The mean GA for the babies in the Egyptian study11 was 31.02±2.13 weeks (152 patients), which was similar to our cohort but higher than other studies including Goble et al's19 examination of 1611 infants from six centres in Birmingham, UK (29.1 weeks). We found that babies who had ROP had significantly lower BW and lower GA compared with those without ROP. In addition, patients with ROP who did not require treatment had greater GA and higher BW when compared with their counterparts who required treatment. We did not find any of the systemic factors examined to be significantly associated with ROP development.
Suggested screening guidelines in Saudi Arabia identify at-risk patients as having a GA at birth of ≤32 weeks and a BW of ≤1500 g.4 Widening the screening criteria in India to include 34-week GA infants and14 screening all babies weighing ≤1700 g has also been recommended.13 In Canada20 and the UK, screening all infants younger than 30 weeks GA or with lower than 1200 g BW and <32 weeks GA or <1501 g BW has been suggested.18 ,21 ROP screening thresholds were set higher in other low/middle-income countries such as Turkey and Saudi Arabia8 ,14 with studies in Saudi Arabia, India and China recommending considering screening more mature infants in their protocols to avoid missing treatable ROP.7 ,14 ,22 ,23
In Ecuador, where the criterion for screening was a BW of 1500 g, several initially unexamined infants presented with inoperable stage 5 ROP, so the criteria were changed in the following year to 1901 g BW and/or 37 weeks GA.3
There are several significant geographic differences in ROP incidence and proportion of ROP-related blindness. More mature infants develop ROP in low/middle-income countries. There are innate differences in at-risk populations across countries. The use of different screening guidelines may be partly responsible for differences in the reported rates of ROP between countries. Additionally, genetics, ethnicity and differences in NICU care may be responsible for some of the differences in ROP incidences and outcomes.24–26 Socioeconomic status and differences in resources may also influence care protocols and the ability to screen patients that ultimately influences outcomes and reported incidences. The proportion of ROP-related blindness also varies greatly and depends on several factors including degree of national development that may influence the availability of neonatal care, general neonatal outcomes, availability of ophthalmic expertise and the existence of effective screening and treatment protocols.
We sought to develop novel screening guidelines for ROP in Iran, which currently does not have nation-specific ROP screening criteria. The ideal ROP guidelines will not miss any patients with ROP that require treatment while limiting the costs, healthcare burden and stress to fragile neonates by minimising examinations of patients with mild or no retinopathy.27The importance of efficient healthcare resources use is particularly heightened in the low/middle-income countries where resource limitations, such as physicians trained in ROP care, exist. Applying AAP guidelines to our patients who have resulted in 8.4% of ROP requiring treatment being missed and although the use of Turkish guidelines would yield 100% sensitivity in our population, it would result in unnecessary examinations and create an extra strain on the healthcare system. We found that screening of premature infants with GA ≤32 weeks and/or BW ≤2000 g, which falls between the Turkish and AAP criteria, has a 100% sensitivity of identifying patients with ROP who require treatment while limiting unnecessary examinations.
Accurate delineation of the population of premature infants who are at risk for this potentially blinding condition is necessary, as it provides the evidence on which to base screening guidelines. The UK, the USA and Canada20 along with China and other countries28 ,29 have developed evidence-based screening criteria that continue to be reviewed as the population of infants who are at risk changes over time.5 ,18 ,30
Though preliminary results of growth-based ROP prediction modelling are promising, and models such as WINROP have the potential to reduce the number of unnecessary and stressful examinations, they are not yet adequately sensitive to be proposed for changing screening practices.31
There are several limitations of this study. Referral criteria used in the nine referring NICUs were standardised. Outpatients, however, were referred by neonatologists who were not necessarily using the same criteria. In addition, infants from outside the nine NICUs may have been referred on an outpatient basis to other providers and were therefore not captured in our study. The incidence data reported here may therefore not reflect the true incidence in the entirety of Iran. Different methods of assessing GA may have been used across the NICUs which would have influenced GA data. We did not consider risk factors beyond GA and BW because of heterogeneity in reporting risk factors among different NICU centres and limitations in the availability of this information from patients who were referred to us from outside as outpatients. Thus, it would be prudent to recommend screening more mature high-risk patients at the discretion of the neonatologist.
In summary, screening guidelines used in highly developed countries are not generalisable to all environments and will miss a high number of patients with ROP with a subsequent risk for blindness. ROP screening guidelines need to be tailored to local populations and continue to evolve. We recommend screening premature patients with GA of ≤32 weeks and or BW of ≤2000 g in Iran.
Acknowledgments
The authors would like to acknowledge the support provided by nine NICUs in Tehran for their help facilitating ROP screening. These NICUs are as follows: Arash, Akbarabadi, Bahrami, Valiasr, Shariati, Firuzgar, Aliasghar, Jameye Zanane and Markaz Tebbi e Kudakan.
References
Footnotes
Competing interests None declared.
Patient consent Obtained.
Ethics approval Eye Research Center, Tehran University of Medical Sciences.
Provenance and peer review Not commissioned; externally peer reviewed.