Article Text

Abstract
Background/aims To investigate the risk of developing retinal vein occlusion (RVO) in patients with systemic lupus erythematosus (SLE).
Methods In this retrospective population-based cohort study, 6756 patients with SLE and 40 536 controls without SLE (1:6) were selected from the Taiwan National Health Insurance Research Database claims from 2001 to 2006.
Results The incidence of RVO was 3.46-times higher in the SLE group than in controls (5.61 vs 1.62 per 10 000 person-years) (adjusted HR=3.883, 95% CI 2.299 to 6.558) calculated using Cox proportional hazard regression. Age was an independent risk factor for RVO, with adjusted HRs of 4.842 for individuals aged ≥50 years compared with those 0–49 years. For each age subgroup, the risk of RVO was significantly higher only in the 0–49-year-old SLE group than in controls. In the 0–49-year-old SLE group the incidence of developing RVO was 7.92 times higher (95% CI 3.60 to 17.45) in the SLE group than in the 0–49-year-old controls. In women with SLE, the incidence of developing RVO was 3.33-times higher (95% CI 1.88 to 5.90) than in female controls.
Conclusions SLE was significantly associated with an increased risk of developing RVO.
- Epidemiology
- Retina
Statistics from Altmetric.com
Introduction
Systemic lupus erythematosus (SLE) is one of the most well known autoimmune diseases. Ocular manifestations, such as retinal vein occlusion (RVO), in SLE are fairly common, potentially sight threatening and may be the presenting feature of their disease.1 The proportion of patients with SLE who manifest retinal involvement varies depending on the population studied; it ranges from 3% in well-controlled patients to 29% in patients with more active systemic disease.2–9
The retinal microangiopathy associated with SLE is thought to result from immune complex mediated vascular injury and microvascular thrombosis.10–12 Therefore, RVO may be a manifestation of systemic vascular involvement in SLE and may have an important impact on the health of these patients. However, the risk of developing RVO in patients with SLE has not been systemically examined.
We investigated both the incidence of RVO in patients with SLE and the effects of five comorbidities—coronary artery disease (CAD), diabetes mellitus (DM), hyperlipidaemia, hypertension (HTN), and stroke—on the risk of developing RVO.
Methods
Data sources
The Taiwan National Health Insurance (NHI) Program is a universal health care system that covers 99% of the country's population of 23.3 million.13 The data used in this analysis were obtained from the National Health Insurance Research Database (NHIRD), which contains all claims data from 1996 through 2010. There were no significant differences in age, gender, or healthcare costs between the sample group and all enrolled residents. The database contains encrypted patient identification numbers, ICD-9-CM (International Classification of Diseases, Ninth Revision, Clinical Modification) codes for applied clinical diagnoses and procedures, details of prescribed drugs, dates of admission and discharge, and basic sociodemographic information, including gender and date of birth.
Design
This was a retrospective cohort study with two study groups: patients with SLE (SLE group); and age, gender, and index date matched controls without SLE (non-SLE group). The SLE group included patients with an initial diagnosis of SLE (ICD-9 code 710.0) who had an SLE catastrophic illness identification card, which exempts them from copayments for outpatient and inpatient care (except for hospital room and board charges). Patients with SLE were identified from records in the Catastrophic Illness Patient Database, a subset of the NHIRD for certain major diseases. Controls without medical claims for SLE were randomly selected. The index date for the patients with SLE was the date between 1996 through 2009 on which they were first registered as having SLE. Other comorbidities that may have presented before the index date were defined as follows: HTN (ICD-9 code 401), hyperlipidaemia (ICD-9 code 272.0-272.4), stroke (ICD-9 code 430-438), CAD (ICD-9 code 410-414, A270, A279), and DM (ICD-9 code 250). The comorbidities were identified only through a diagnosis made during admission or by a specialist upon the patient's third hospital visit. Newly developed RVO (ICD-9 code 362.35, 362.36) was identified by referred teaching hospitals and tertiary referred medical centres. The Taiwan Health Insurance Bureau conducts routine peer reviews to maintain diagnostic consistency, especially in referred teaching hospitals and tertiary referred medical centres. To investigate the association between the occurrence of RVO and the disease progress of SLE, only patients with newly diagnosed SLE from 2001 to 2006 were included. The claims data from 1996 to 2000 were used to confirm none of the enrolled patients had ever been diagnosed with SLE or RVO before 2001. Follow-ups were done for a minimum of 4 years (2006–2009) to determine the incidence of RVO until the end of 2009, or until they were censored due to death. The identification numbers of all of the individuals in the NHIRD were encrypted to protect their privacy. Institutional review boards of Chi Mei Medical Centre and Taipei Medical University approved this study.
Statistical analysis
Descriptive statistical analyses using Pearson’s χ2 test were done to compare the differences in sociodemographic characteristics and comorbidities between the SLE group and the controls. The incidence rate was calculated as the number of RVO cases identified during follow-up divided by the total person-years for each group by gender, age, and number of follow-up years. The risk of developing RVO was compared by estimating the incidence ratio using a Poisson regression. The risk of developing RVO associated with the five above mentioned comorbidities was estimated using Cox proportional hazard models. A Cox proportional hazard regression analysis with propensity score matching was used to estimate the hazard ratio between the SLE group and the controls. Propensity score matching was used to reduce any selection bias in our hypothesis, which can bundle many confounding covariates that may be present in an observational study with this number of variables.14 Score matching identified the predicted probability of obtaining one SLE patient versus one control from the logistic regression model according to the baseline covariates of age, gender, geographic region, and income.
Lupus retina changes may be part of the clinical picture of hypertensive retinopathy, because HTN is often present secondary to lupus nephritis. Lupus retinopathy can occur as an independent manifestation of the underlying disease process in the absence of HTN.15 ,16 To treat HTN as a confounder, the comorbidity of HTN was also matched. A Cox proportional hazards regression analysis and a Kaplan–Meier survival analysis were used to calculate the cumulative incidence rates of RVO in the two cohorts, and the log rank test was used to analyse the differences between the survival curves. SAS for Windows V.9.2 (SAS Institute, Cary, North Carolina, USA) was used for all statistical analyses. Significance was set at p<0.05 (two tailed).
Results
Incidence of RVO based on patient characteristics
Based on the 2001 to 2006 claims data, 6756 patients with SLE met the eligibility criteria and an additional 40 536 participants were randomly selected for inclusion in the control group. Of the 6756 patients with SLE, 6021 (89.12%) were female and 735 (10.88%) were male. The annual incidence of SLE in Taiwan averaged 5.19 per 100 000 from 2001 to 2006. The sociodemographic characteristics and comorbid medical disorders in patients with SLE and the control group were similar in gender and age distribution (table 1). The ratio of patients with central retinal vein occlusion (CRVO) to those with branch retinal vein occlusion (BRVO) was not significantly different between the two groups. There were significant differences in annual income (p=0.0014) and geographical distribution (p<0.0001) between the two groups, however.
Demographic characteristics and comorbid medical disorders for patients with systemic lupus erythematosus (SLE) and without SLE (controls) in Taiwan after matched by propensity scores
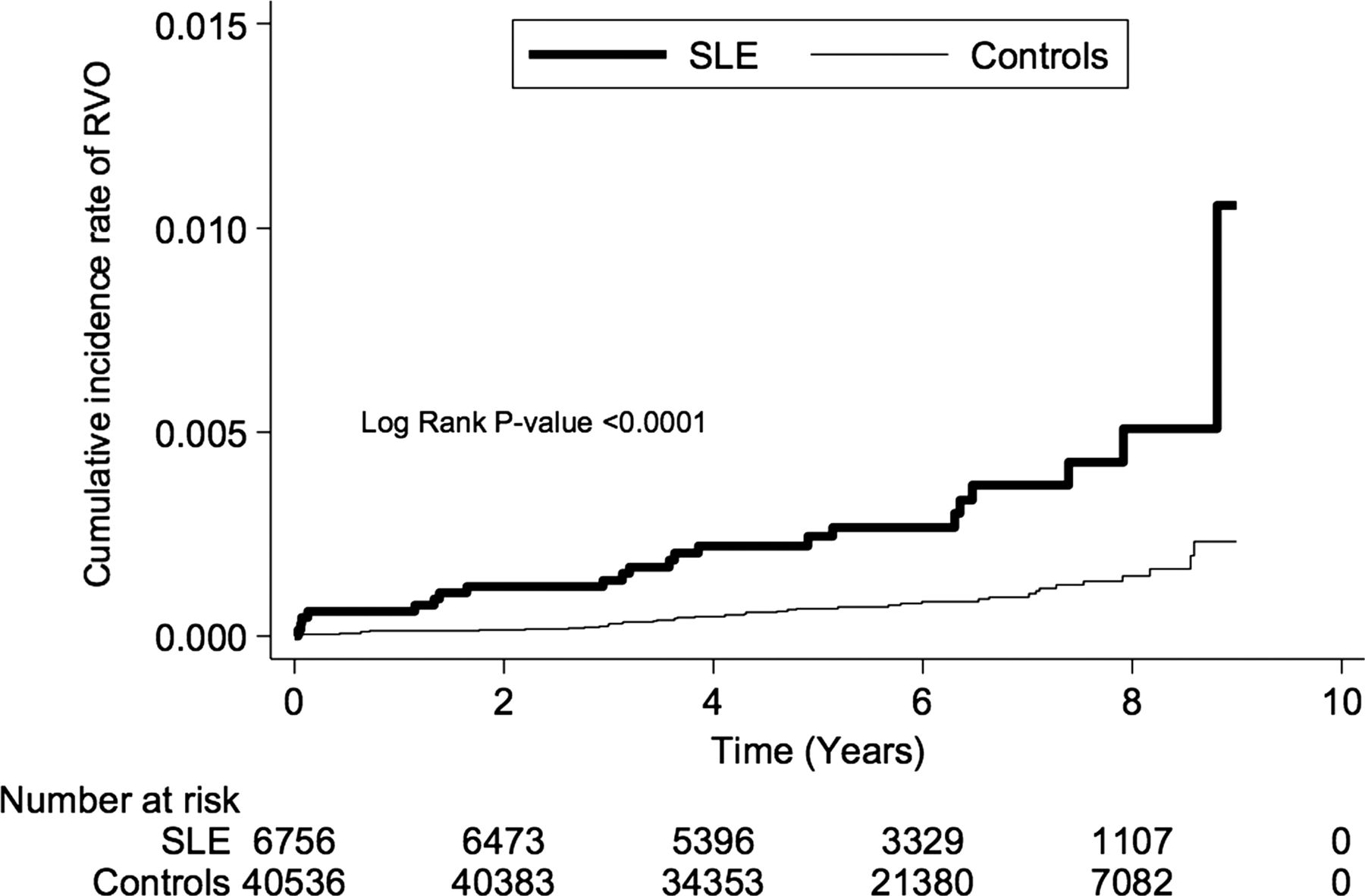
The estimated risk of developing RVO based on gender, age, and the number of years of follow-up in the SLE group and the control group was compared. By the end of the follow-up period, the cumulative incidence rate of RVO was higher in the SLE group than in the control group (p<0.0001) (figure 1). The incidence rates of RVO classified by gender, age, and number of years of follow-up were compared between the SLE group and the control group. For each age subgroup, there was a significantly increased risk of RVO in the SLE group compared with the control group, but only in patients who were 0–49 years old (p<0.0001). In the 0–49 age range, the incidence of developing RVO was 7.92 times higher (95% CI 3.60 to 17.45) in the SLE group than in the control group (table 2).
Risk of retinal vein occlusion (RVO) for patients with systemic lupus erythematosus (SLE) and without SLE (controls)

{kind=link}
The cumulative incidence rate of retinal vein occlusion (RVO) in the systemic lupus erythematosus (SLE) group and the non-SLE control group in Taiwan (2000–2009).
In both groups, patients ≥50 years of age had a higher incidence of RVO than did patients 0–49 years (adjusted HR (AHR) 4.842, 95% CI 2.624 to 8.936) (table 3). A stratified analysis of the duration of follow-up showed a significantly higher incidence of developing RVO in the SLE group than in the control group when stratified by <2 (p<0.0001), 2–4 (p=0.0306), and >4 (p=0.0314) follow-up years (table 2).
Crude and adjusted hazard ratios of Cox proportional hazards regressions and 95% CI for the development of retinal vein occlusion during the follow-up period for the study cohort
Gender specific incidence rate ratio of RVO
The incidence rate of RVO was significantly higher for women (incidence rate ratio (IRR) 3.33, 95% CI 1.88 to 5.90) and for men (IRR 4.22, 95% CI 1.19 to 14.95) in the SLE group than in the control group (p=0.0257) (table 2).
RVO is associated with comorbid DM
The risk of developing RVO was higher in the SLE group than in the control group (AHR 3.883, 95% CI 2.229 to 6.558). There were significant differences in the prevalence of comorbid stroke, CAD, and hyperlipidaemia (p<0.0001 for all) between the two groups. A multivariate Cox proportional hazards regression analysis, which included gender, age, geographic region, income, and comorbidities in the model, revealed no significant differences in the risk of developing RVO with the comorbidities of stroke, CAD, DM, and hyperlipidaemia (table 3). However, there was a significant difference in the risk of developing RVO with the comorbidity of HTN (AHR 2.91, 95% CI 1.12 to 7.58; p=0.0284) (table 2).
Discussion
The major finding in this study was that patients diagnosed with SLE between the years 2001 and 2006 had a substantially higher incidence of RVO than controls without SLE from the general population (IRR 3.46, 95% CI 2.01 to 5.83) (table 2), which is consistent with the literature.1–3
Patients diagnosed with SLE typically (63.6%) develop RVO in the first 4 years of follow-up. Our findings agree with previous reports. For example, one retrospective cohort study of 426 patients with SLE17 found that the incidence of thrombovascular events was highest during the first year post-diagnosis. Another cohort study of 482 patients with autoimmune disease18 reported that, in the SLE group, 78% of thrombosis observed occurred during the first 5 years of follow-up.
We found that patients in the 0–49 year age group had a significantly higher incidence of RVO than did controls. However, patients in the ≥50 year age group did not show a significantly increased incidence of RVO. This discrepancy between different age groups may reflect age related differences in the clinical manifestations of SLE. Vasculopathy may be more common in women with an earlier onset of SLE.19 Our findings agree with a report that women aged 18–44 years with SLE had a significantly higher risk of acute myocardial infarction, congestive heart failure, and cerebrovascular accident than did controls without SLE.20
The risk of patients with SLE developing CRVO (p=0.0015) and BRVO (p=0.0006) was significantly higher than for controls. HTN is believed to be one of the major causes of BRVO,21 ,22 and both HTN and vascular disease are believed to be important risk factors for CRVO.23 In addition, we found that the risk of developing RVO did not increase with the comorbidities of hyperlipidaemia, CAD, or stroke (table 2). Our results are in line with the consensus that SLE retinopathy is generally considered to be an immune complex mediated vasculopathy.24
We found a significant IRR (3.33, 95% CI 1.88 to 5.90) between the SLE group and controls for the development of RVO in women, and a more pronounced IRR (4.22, 95% CI 1.19 to 14.95) between the SLE group and controls for the development of RVO in men. However, a multivariate Cox proportional hazard regression analysis showed no significant difference in the risk of developing RVO based on gender (adjusted HR 1.531, 95% CI 0.774 to 3.020). Other studies may not have been able to examine the significance of gender due to a limited number of patients with RVO.1–3
The underlying mechanism of developing RVO in patients with SLE remains unclear. SLE retinopathy is generally considered to be an immune complex mediated vasculopathy, based on previous reports of immune complex deposition in retinal vessels in SLE.24 Rather than a true inflammatory vasculitis, the lupus retinopathy is thought to stem from fibrinoid degeneration with necrosis of the vessel walls.24 It is felt that atherosclerosis as a result of HTN, steroid use, and dyslipidaemia in SLE may be involved in the development of SLE retinopathy.25 A systematic review22 of all studies published between January 1985 and July 2007 that compared cases with any form of RVO, including BRVO and CRVO, with controls, found that both HTN (OR 3.5, 95% CI 2.5 to 5.1) and hyperlipidaemia (OR 2.5, 95% CI 1.7 to 3.7) were significantly associated with RVO, but that the association was less pronounced for DM (OR 1.5, 95% CI 1.1 to 2.0). In the present study, Cox proportional hazards regression was used to access the possibility of linkage between the development of RVO and comorbid DM, HTN, hyperlipidaemia, and the HTN related diseases of stroke and CAD. Our analyses of subgroups with comorbid HTN, hyperlipidaemia, stroke, CAD, and DM showed that the risk of developing RVO did not increase with the comorbidities of hyperlipidaemia, CAD, or stroke, but that it did with the comorbidity of HTN (AHR 2.84, 95% CI 1.456 to 5.567). This implies that comorbid HTN contributes to the development of RVO, but the association in the subgroup was less pronounced than it was in the overall group in the present study. In the subgroup of patients with comorbid DM, the risk of developing RVO was higher in the SLE group than in the non-SLE group (IRR 6.33, 95% CI 1.71 to 23.59; p=0.0059). Because the baseline comorbidity of DM was not significantly different between the SLE and controls, we may conclude that there was a synergic effect between DM and SLE for the development of RVO in the present study.
Strengths and limitations
This study, with its large sample size, indicates that there is an elevated risk for patients with SLE to develop RVO. The data extracted using diagnostic codes from catastrophic illness identification cards issued to patients with SLE makes the possibility of misdiagnosis or misclassification highly improbable. Medical access to a referred teaching hospital and tertiary referred medical centre is convenient in Taiwan, and their exemption from co-payments for SLE care makes patients highly adherent to physician prescribed therapeutic regimens. This nationwide population based dataset, which includes a large sample of SLE cases and longitudinal follow-ups, allows researchers to analyse, with a minimal tendency for selection bias, the risk factors for developing RVO. The large sample size also increased the statistical power and precision of risk appraisal.13
This study has some limitations. Several suspected risk factors for RVO were not available in the insurance database, such as current blood pressure and laboratory data of serum cholesterol and triglyceride values. The insurance claims data did not include information on the severity of RVO or other laboratory test results. Clinical examinations, such as skin lupus flare, systemic manifestations, and imaging results, were not available to evaluate the extent of SLE treatment in the selected sample. The inability to assess these factors may have introduced some bias.
Awareness of the elevated risk of developing RVO in patients with SLE might prompt the early detection and treatment of RVO. Medications that control autoimmune activity may benefit patients with SLE who are at risk of developing RVO. With appropriate and timely medical interventions, the prognosis of RVO in patients diagnosed with SLE is good.
Conclusion
SLE was significantly associated with an increased risk of developing RVO. A significantly higher risk was observed in patients aged 0–49 years, particularly in females.
Acknowledgments
This study is based in part on data from the Taiwan National Health Insurance Research Database provided by the Taiwan Bureau of National Health Insurance. The interpretation and conclusions contained herein do not represent those of the Taiwan Bureau of National Health Insurance.
References
Footnotes
-
Contributors YCY: made substantial contributions to study design, and was involved in the acquisition of data. YSL, HAC, and SFW: made substantial contributions to study conception and design, and data analysis. All authors reviewed and approved the manuscript's content before submission, and jointly agreed to submit the final version.
-
Funding This work was supported by Taipei Medical University-Chi Mei Medical Centre Research Fund, grant number 09909-066.
-
Competing interests None.
-
Ethics approval Institutional Review Board of Chi Mei Medical Center, No. 09909-066.
-
Provenance and peer review Not commissioned; externally peer reviewed.
-
Data sharing statement This study is based in part on data from the National Health Insurance Research Database provided by the Bureau of National Health Insurance, Department of Health and managed by National Health Research Institutes. The identification numbers of all of the individuals in the NHIRD were encrypted to protect privacy. All the data could be accessed only for research and academic discussion with the editor and readers through our corresponding author.