Article Text

Abstract
Aim To evaluate intravitreal VEGF Trap-Eye (VTE) in patients with macular oedema secondary to central retinal vein occlusion (CRVO).
Methods In this double-masked study, 177 patients were randomised (3:2 ratio) to intravitreal injections of VTE 2 mg or sham procedure every 4 weeks for 24 weeks. Best-corrected visual acuity was evaluated using the Early Treatment Diabetic Retinopathy Study chart. Central retinal thickness (CRT) was measured with optical coherence tomography.
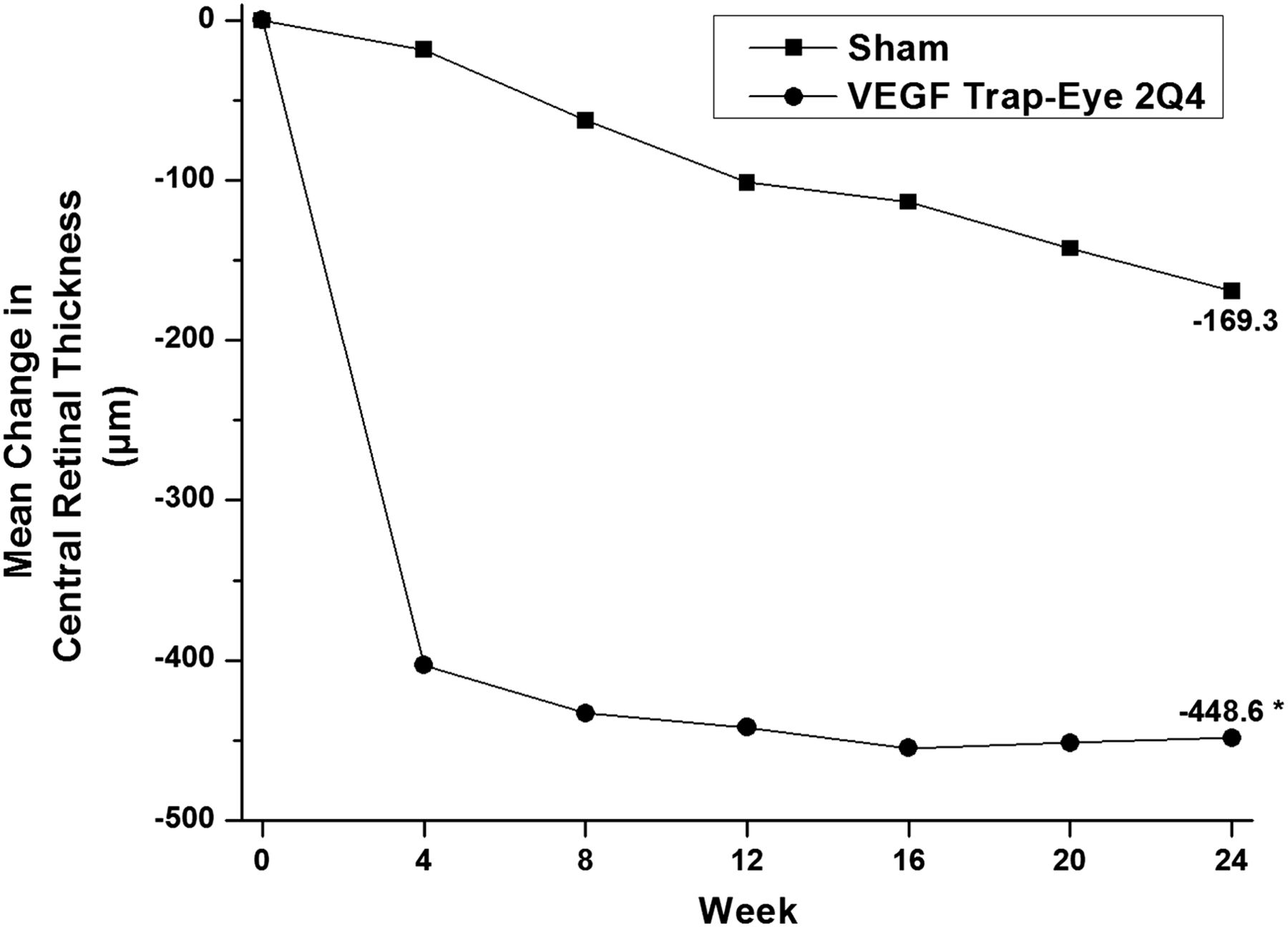
Results From baseline until week 24, more patients receiving VTE (60.2%) gained ≥15 letters compared with those receiving sham injections (22.1%) (p<0.0001). VTE patients gained a mean of 18.0 letters compared with 3.3 letters with sham injections (p<0.0001). Mean CRT decreased by 448.6 and 169.3 µm in the VTE and sham groups (p<0.0001). The most frequent ocular adverse events in the VTE arm were typically associated with the injection procedure or the underlying disease, and included eye pain (11.5%), increased intraocular pressure (9.6%) and conjunctival haemorrhage (8.7%).
Conclusions VTE 2 mg every 4 weeks was efficacious in CRVO with an acceptable safety profile. Vision gains with VTE were significantly higher than with observation/panretinal photocoagulation if needed. Based on these data, VTE may provide a new treatment option for CRVO.
- Macula
- Neovascularisation
- Retina
Statistics from Altmetric.com
Introduction
Macular oedema is the most common cause of vision loss for patients with central retinal vein occlusion (CRVO).1 Patients suffering from CRVO, particularly from non-perfused CRVO,2 have the worst prognosis of all RVO patients.3
A wide variety of strategies have been used for the treatment of macular oedema secondary to CRVO including surgical procedures,4–6 laser photocoagulation,7 steroid implants,8 intravitreal steroid injections9 and, more recently, antivascular endothelial growth factor (anti-VEGF) agents.10–14 Although effective in reducing macular oedema secondary to CRVO, macular grid laser photocoagulation did not appear to improve vision compared with observation.2 Treatment with steroids resulted in vision gains, but was associated with higher rates of intraocular pressure (IOP) elevation, cataract formation and steroid-induced secondary glaucoma.8 ,9 ,15 In contrast, intravitreal injections of anti-VEGF agents reduced macular oedema and improved vision with a better safety profile compared with intravitreal steroids.10–14 Based on a survey from the American Society of Retinal Specialists, over 70% of the retinal specialists (n=619) use intravitreal anti-VEGF agents to treat macular oedema secondary to CRVO.16
VEGF Trap-Eye (VTE, aflibercept injection; Regeneron Pharmaceuticals, Inc. Tarrytown, New York, USA, and Bayer HealthCare Pharmaceuticals, Berlin, Germany) is a fusion protein comprising key domains from human VEGF receptors 1 and 2 with human IgG Fc that blocks all VEGF-A isoforms and placental growth factor.17 ,18 Previous studies with VTE have demonstrated improvements in visual function for patients with neovascular age-related macular degeneration19 ,20 and diabetic macular oedema.21 GALILEO is one of two similar trials (with the COPERNICUS study)22 designed to evaluate the efficacy and safety of intravitreal VTE in patients with macular oedema secondary to CRVO.
Methods
GALILEO is a phase III, randomised, double-masked, multi-centre clinical study conducted across 63 centres in Europe (Austria 3; France 5; Germany 21; Hungary 5; Italy 7; Latvia 2) and the Asian/Pacific region (Australia 6; Japan 6; Singapore 2; South Korea 6). The total study duration is 76 weeks, with 68 weeks of treatment (figure 1). Herein the results from primary analyses at week 24 are reported, while the study continues in a masked fashion up to week 76 with an additional analysis planned at week 52 (registered as NCT01012973 on clinicaltrials.gov). The appropriate institutional review boards/ethic committees approved the protocol and all participants provided written informed consent.
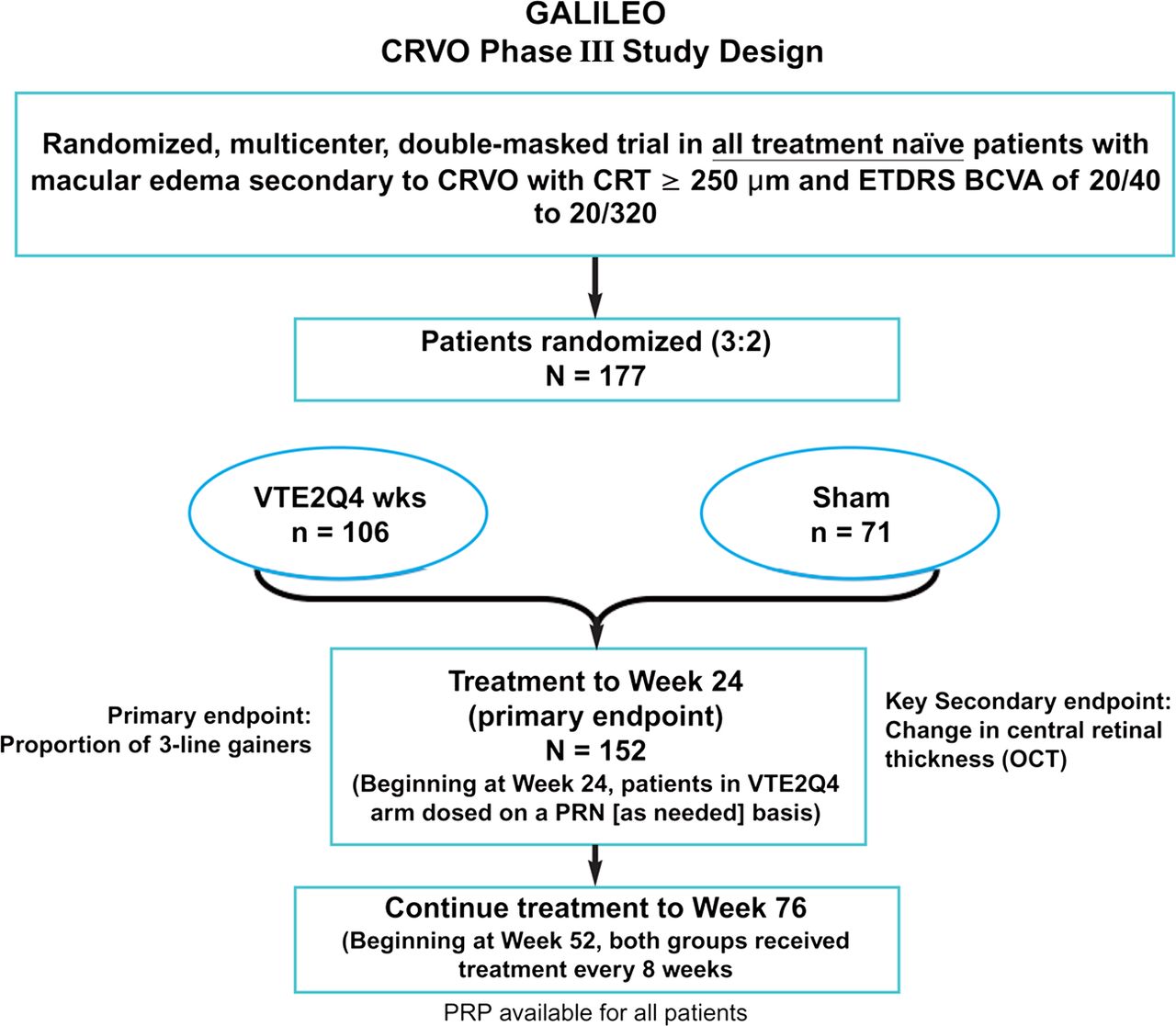
GALILEO study design. The two study arms consisted of VEGF Trap-Eye 2 mg every 4 weeks or sham intravitreal injections every 4 weeks. BCVA, best-corrected visual acuity; CRT, central retinal thickness; CRVO, central retinal vein occlusion; ETDRS, Early Treatment Diabetic Retinopathy Study; OCT, optical coherence tomography; PRP, panretinal photocoagulation; VTE2Q4, VEGF Trap-Eye 2q4. This figure is only reproduced in colour in the online version.
Since at the time when the GALILEO and COPERNICUS studies were started there was no approved treatment for CRVO, health authorities requested that the duration of the sham treatment in GALILEO be extended to a full year (the sister study, COPERNICUS, conducted outside the EU maintained a sham arm for only the first 6 months). Considering this rather long duration of sham treatment, the visual acuity and other ocular findings were observed carefully by a team of masked medical reviewers. If, at any time, this review team had the impression that a patient might not benefit from further study participation or might be more adequately treated outside the study, the investigator was queried and asked to provide a reassessment of the patient.
Participants
Treatment-naive patients, age ≥18 years, were included if they had centre-involved macular oedema secondary to CRVO for a maximum of 9 months, with a central retinal thickness (CRT) ≥250 μm on optical coherence tomography (OCT) and an Early Treatment Diabetic Retinopathy Study (ETDRS) best-corrected visual acuity (BCVA) of 73 to 24 letters (20/40 to 20/320) in the study eye. Patients were excluded if they were pregnant or had uncontrolled glaucoma (IOP≥25 mm Hg), filtration surgery, bilateral manifestation of RVO, iris neovascularisation, or previous treatment with anti-VEGF agents, pan-retinal or macular laser photocoagulation, or intraocular corticosteroids.
Treatments
Patients were randomised in a 3:2 ratio to receive either intravitreal injections of VTE 2 mg (VTE2Q4) or sham procedure every 4 weeks for 24 weeks. Sham procedure was performed by pressing an empty syringe with no needle to the conjunctival surface. Randomisation was stratified by region (Europe vs Asia/Pacific) and baseline BCVA (≤20/200 vs >20/200). Pan-retinal photocoagulation was allowed at any time for all patients if they progressed to neovascularisation of the anterior segment, optic disc or fundus.
Endpoints
The primary endpoint was the proportion of patients who gained ≥15 letters in BCVA at week 24 compared with baseline. The secondary endpoints were: (a) the change from baseline to week 24 in BCVA and CRT, (b) the proportion of patients progressing to neovascularisation of anterior segment, optic disc or elsewhere in the fundus by week 24 and (c) the changes in vision-related and overall health-related quality of life (QoL) as assessed by the National Eye Institute Visual Functioning Questionnaire-25 (NEI VFQ-25) and European Quality of Life-5 Dimensions (EQ-5D) Health Questionnaire, respectively. Selected subscales of NEI VFQ-25 were assessed as tertiary efficacy variables.
Methodology
Visual function was assessed using the ETDRS charts.23 Retinal characteristics were evaluated using OCT (Stratus OCT, Carl Zeiss Meditec, Jena, Germany). Baseline retinal perfusion status was determined by fluorescein angiography using the central vein occlusion study (CVOS) classification.2 Patients were considered non-perfused if they had ≥10 disc areas of capillary non-perfusion. Vision-related and overall health-related QoL was assessed using the NEI-VFQ-25 and EQ-5D Health Questionnaires, respectively.
Statistics
A total of 150 patients (90 VTE/60 Sham) were considered necessary to detect a between-group difference of 25% in proportion of patients gaining ≥15 letters with a power of 90% using a two-sided Fisher's exact test. For the efficacy analyses, the full analysis set included all randomised patients who received any study treatment and had baseline and at least one postbaseline BCVA assessment. The safety analysis set included all patients who received any study treatment. For the primary endpoint analysis, the between-group difference was evaluated by a two-sided Cochran-Mantel-Haenszel (CMH) test at a 5% level stratified for regions and baseline visual acuity. In this analysis, patients who discontinued prior to week 24 were considered as non-responders. Several sensitivity analyses for the primary endpoint were performed by imputing the missing values with the last observation carried forward (LOCF) approach, using observed cases, or excluding patients who discontinued study prior to week 24 and received fewer than five injections.
Secondary endpoint analyses were performed sequentially according to the order in which the variables were defined to preserve an α of 0.05. Proportions were analysed with the CMH test. BCVA as a continuous variable was analysed by analysis of variance main effects model with treatment group, region and baseline BCVA as fixed factors. A descriptive, post hoc analysis using a double-sided Fisher test was conducted to evaluate the between-group differences in the proportion of patients losing ≥1 and ≥10 letters.
Results
Patient disposition, demographics and disease characteristics
A total of 240 patients were screened, 177 patients were randomised and 172 patients were included in the safety analysis set (table 1). One patient did not have any postbaseline BCVA assessment. Therefore, the full analysis set comprised 171 patients (table 1). Overall, 86.4% of VTE2Q4 patients and 79.4% of sham patients had a perfused retinal occlusion (table 2).
Patient disposition (all randomised patients) and overview of analysis sets
Baseline demographics and disease characteristics (study eye)
Visual outcomes
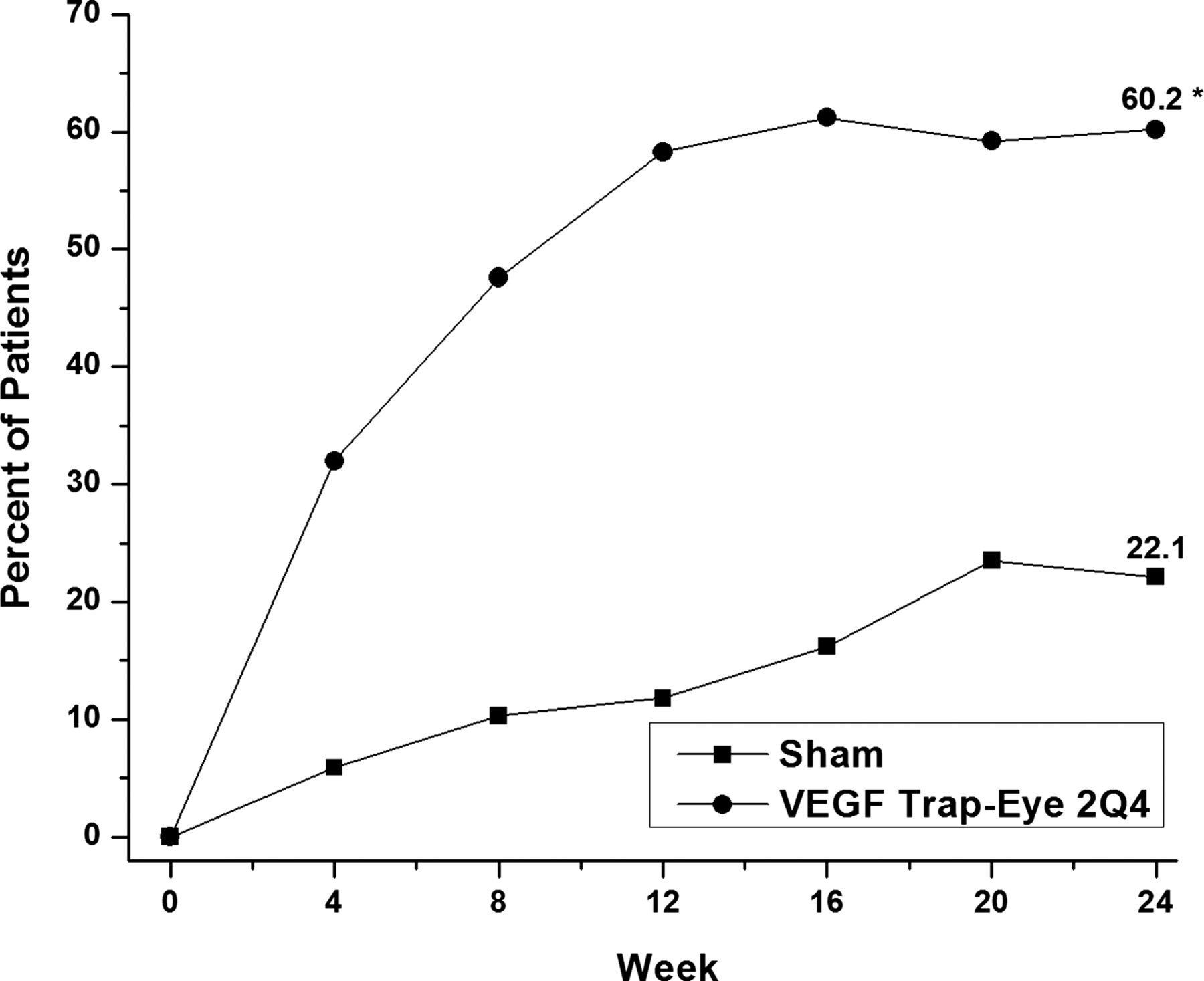
Significantly more VTE2Q4-treated patients gained ≥15 letters by week 24 than those receiving sham injections (60.2% vs 22.1%, p<0.0001) with a CMH-adjusted difference of 38.3% (table 3, figure 2). Similar results for the CMH-adjusted difference (95% CI) was obtained after imputing the missing values with the LOCF approach (41.1% (27.4% to 54.9%)), using the observed cases (38.7% (23.5% to 53.8%)), or excluding patients who discontinued study prior to week 24 and received fewer than five injections (39.2% (25.4% to 53.0%)).
Primary and secondary endpoints

Percentage of patients who gained ≥15 letters over the course of 24 weeks. Full analysis set; patients who discontinued prior to respective visit evaluated as non-responders. VEGF Trap-Eye 2Q4, n=103; sham, n=68. Difference between groups at week 24=38.1%. *p<0.0001 VEGF Trap-Eye versus sham was calculated using two-sided Cochran-Mantel-Haenszel test adjusted by region and baseline best-corrected visual acuity category.
Patients receiving VTE2Q4 had a significantly greater mean change in BCVA than the sham-treated patients at week 24 (18.0 vs 3.3 letters, respectively; p<0.0001; figure 3) resulting in an adjusted between-group difference of 14.7 letters (table 3). The VTE2Q4 arm also showed higher proportions of patients with vision gains of ≥0, ≥10 and ≥30 letters at week 24 (figure 4). In all, 11 (10.7%) patients in the VTE2Q4 group experienced a loss of one or more letters during the course of the 24 weeks compared with 27 (39.7%) patients in the sham arm (p<0.0001). A total of 8 patients (7.8%) in the VTE2Q4 group lost 10 or more ETDRS letters during the 24 weeks compared with 17 (25.0%) for the sham group (p=0.0033).
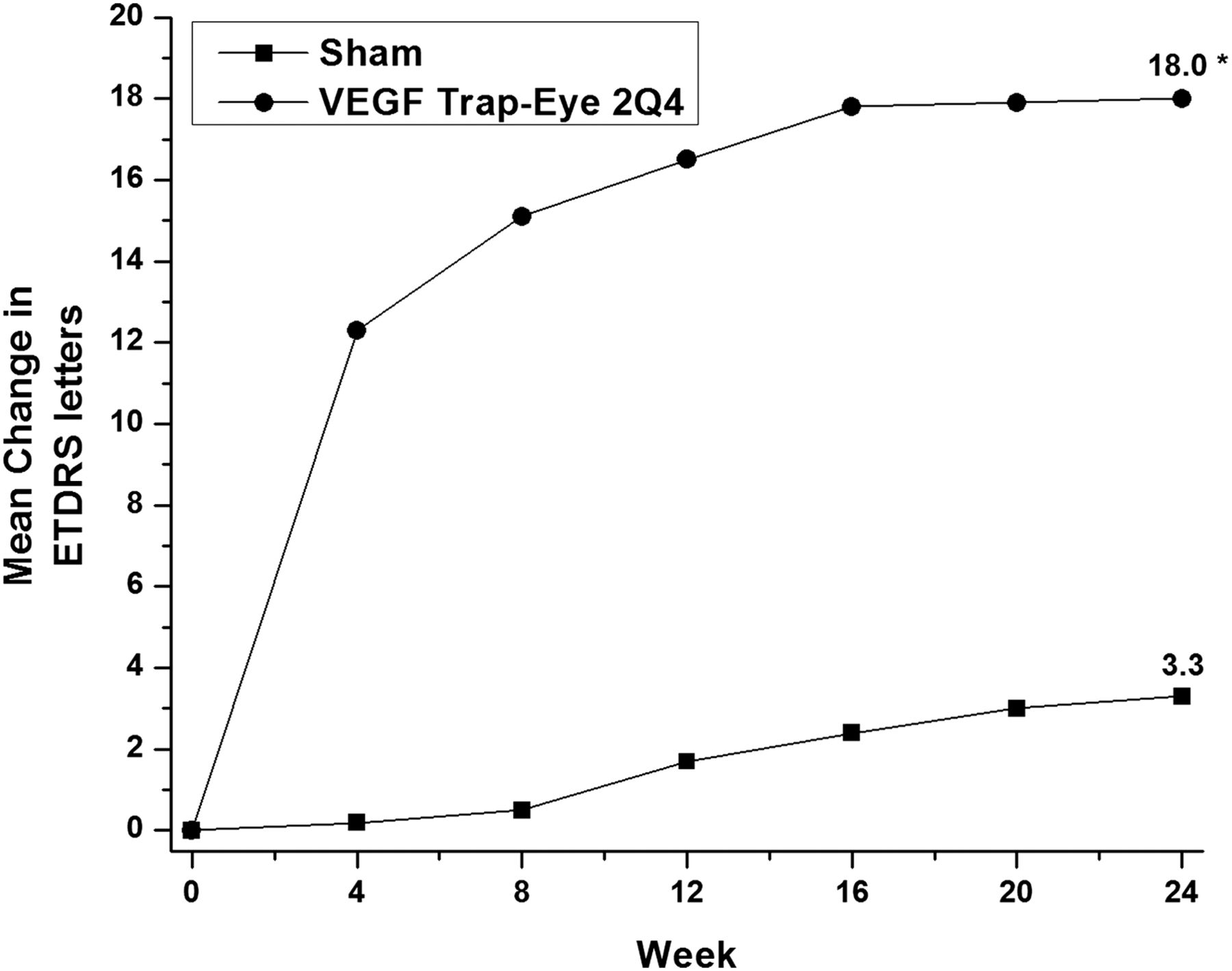
Mean change in visual acuity (Early Treatment Diabetic Retinopathy Study (ETDRS) letters). Full analysis set; LOCF. VEGF Trap-Eye 2Q4, n=103; sham, n=68. Difference between groups at week 24=14.7 letters. *p<0.0001 VEGF Trap-Eye versus sham based on treatment difference of the least squares mean changes derived from analysis of variance.
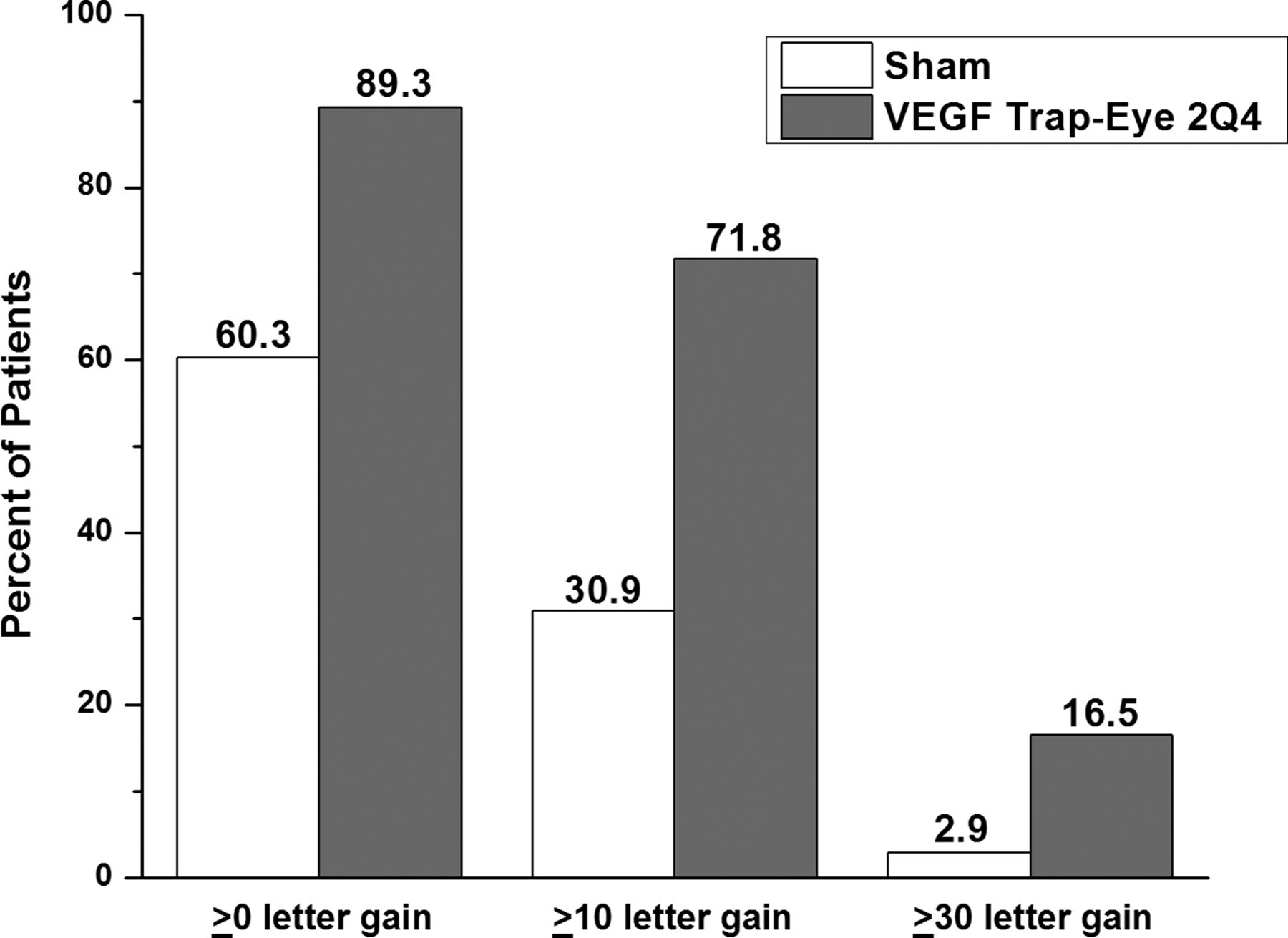
Proportion of patients who gained vision at week 24 compared with baseline. Full analysis set; patients who discontinued prior to week 24 evaluated as non-responders. VEGF Trap-Eye 2Q4, n=103; sham, n=68.
Larger numerical differences between VTE2Q4 and sham were seen in the subgroup of patients with disease duration <2 months compared with the difference noted in the study population as a whole (disease duration <2 months: unadjusted difference of 50.9% ((20.0% sham; 70.9% VTE2Q4)). Within the VTE2Q4 group, the proportion of patients who gained at least 15 letters at week 24 was higher (70.9%) for patients beginning treatment within 2 months of diagnosis compared with 50.0% of VTE2Q4 patients starting treatment ≥2 months after diagnosis.
Anatomical outcomes
The difference between the treatment groups in mean changes in CRT at week 24 was 279.3 µm (figure 5) (difference between least squares mean changes 239.4; p<0.0001, table 3). Neovascularisation was developed in three VTE2Q4 patients (2.9%) (two anterior segment neovascularisation and one neovascularization elsewhere (NVE)) and three sham patients (4.4%) (one anterior segment neovascularisation and two NVE) (p=0.5947, table 3). Only one case of iris neovascularisation in the VTE2Q4 group required treatment with pan-retinal laser photocoagulation. The other cases reported to be neovascularisation in the VTE2Q4 group did not require therapy. All of the three sham patients with neovascularisation received pan-retinal laser photocoagulation. No further rescue laser treatment was applied until week 24.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Mean change in central retinal thickness. Full analysis set; LOCF. VEGF Trap-Eye 2Q4, n=103; sham, n=67. Difference between groups at week 24=279.3 µm. *p<0.0001 VEGF Trap-Eye versus sham is based on treatment difference of the least-squares mean changes derived from analysis of covariance (ANCOVA).
QoL outcomes
The mean change from baseline to week 24 in total NEI-VFQ scores was 7.5 for the VTE2Q4 group and 3.5 for the sham group. The between-group difference in both the total NEI-VFQ score and the near-activities subscore was significant at week 24 (p=0.0013 and p=0.0003, respectively, table 3). A trend was observed between groups in favour of VTE2Q4 for the distance-activities subscore, dependency subscore and overall mean EQ-5D score at week 24 (p=0.0689, p=0.2552, p=0.0627, respectively).
Safety
The most common treatment-emergent adverse events (AEs) for the VTE2Q4 patients were eye pain, increased IOP and conjunctival haemorrhage (table 4). A slight imbalance was seen in IOP-increased AEs between VTE2Q4 (10 (9.6%)) and sham (4 (5.9%)). Of note, 5 (4.8%) of these IOP-related AEs were procedure-related in the VTE2Q4 group, while only 1 (1.5%) in the sham group was related to procedure. Three incidents (2.9%) of increased IOP in the VTE2Q4 group were judged to be drug-related compared with 1 (1.5%) for the sham group. The IOP-increased events for reasons other than the injection procedure were well balanced across the arms (table 5). The proportions of patients experiencing predefined elevations in IOP (ie, ≥10 mm Hg change from baseline, >21 mm Hg or ≥35 mm Hg) were low and similar between treatment groups at all time points.
Treatment-emergent adverse events. Those events with an incidence ≥3% in either study group are shown
Mean IOP prior to injection and the proportion of patients experiencing predefined elevation in IOP during the study
There were no incidences of endophthalmitis or cases of rhegmatogenous detachment in either treatment group. There was one incidence of uveitis in the VTE2Q4 arm that was considered to be mild and resolved without change of therapy. There were none in the sham group. Two patients in the VTE2Q4 group and four patients in the sham group had ocular SAEs (table 6). There were no arterial thromboembolic events or deaths reported in either treatment group during the 24-week study period.
Percentage of patients with treatment-emergent ocular SAEs (Study eye)
Discussion
VTE 2 mg every 4 weeks resulted in significantly better visual acuity outcomes than sham. Clinically relevant improvements in visual acuity in the VTE2Q4 group could be seen as early as the first post-treatment assessment (week 4) and reached a stable level, on average, around week 16. The better visual acuity outcome was accompanied by more favourable vision-related QoL measures in the VTE2Q4 group than in the sham group.
Several studies have investigated the efficacy of other anti-VEGF agents for the treatment of macular oedema secondary to CRVO. The CRUISE study reported that patients receiving monthly injections of 0.5 mg ranibizumab (n=130) experienced a mean change from baseline BCVA of 14.9 letters at 6 months.10 Furthermore, 47.7% of patients gained ≥15 letters at 6 months. A relatively smaller, randomised, double-masked study of bevacizumab (n=30) found a mean increase of 14.1 letters from baseline to week 24 in BCVA of patients receiving bevacizumab every 6 weeks.24 The proportion of patients gaining ≥15 letters in the bevacizumab study was 60% at 24 weeks.24 These findings compare favourably with the results of the current study as the mean increase in BCVA was 18.0 letters and 60.2% of patients gained ≥15 letters in the VTE2Q4 group (n=103) at week 24. Improvements in visual acuity were observed in the CRUISE study as early as at the 7-day time point.10 The efficacy with VTE was not measured until the fourth week; however, both studies suggest that the effect of anti-VEGF agents on macular oedema secondary to CRVO occurs very soon after the initiation of treatment.
In parallel with the increases in BCVA, patients in the VTE2Q4 arm experienced a substantial reduction in CRT. Like visual acuity, the onset of the effect on CRT occurred immediately after the first treatment resulting in a rapid restoration of macular morphology. The CRUISE and bevacizumab studies found reductions in central foveal thickness consistent with the current study.10 ,24
Since VEGF is a known stimulator of angiogenesis,25 VEGF blockade is expected to reduce neovascularisation secondary to CRVO. Numerically, a lower percentage of patients in the VTE2Q4 than the sham group progressed to any neovascularisation. However, this effect was not significant due to the generally low incidence of neovascularisation in both study arms. Of note, investigators treated all three patients with neovascularisation in the sham arm, but only one of the three patients in the VTE2Q4 arm. None of the neovascularisation events were serious. No unexpected safety findings were reported. The key AEs were either due to the injection procedure or to the underlying disease. The slight imbalance in the rate of increased IOP in VTE-treated eyes might reflect transient IOP increases after the injection procedure, as an indepth analysis of preinjection IOP did not reveal a relationship between increased IOP and the drug therapy.
The sham group had a higher percentage of patients discontinuing study primarily due to AEs and lack of efficacy; this had no major impact on the analysis of the primary endpoint (with discontinued patients before week 24 judged as non-responders), as similar results were obtained after imputing the missing values with the LOCF approach, using observed cases, or excluding patients who discontinued prior to week 24 and received fewer than five injections.
The week 24 results using VTE2Q4 from the GALILEO study are consistent with those seen in the sister study, COPERNICUS,22 which also compared CRVO patients receiving VTE2Q4 with patients receiving monthly sham injections. The visual outcomes in the sham group were more slightly favourable in GALILEO than in COPERNICUS.22
In conclusion, the GALILEO study demonstrated efficacy of VTE in the treatment of macular oedema due to CRVO with a generally favourable safety and tolerability profile. Therefore, VTE may have the future potential to contribute to the management of patients with this sight-threatening condition.
Acknowledgments
The authors thank the members of the Independent Data Monitoring Committee, Marc de Smet, Yit Yang, Finn Waagstein and Walter Lehmacher, for their review of safety data and their recommendations during the conduct of the trial. Editorial assistance for the preparation of this manuscript was provided by Julie Crider, PhD.
References
Footnotes
-
Contributors All authors, FGH, JR, YO, J-FK, CS, GG, RV, AB, FH, KB, OZ and RS, were involved in the conception and design, acquisition of data, or analysis and interpretation of data in the GALILEO study. Additionally, all authors were involved in the drafting and revision of the article for intellectual content and the approval of the final version to be published.
-
Funding The GALILEO study was supported by Bayer HealthCare, Berlin, Germany and Regeneron Pharmaceuticals, Inc. Tarrytown, New York, USA.
-
Competing interests Dr Holz is a consultant to Acucela, Bayer HealthCare, Boehringer-Ingelheim, Heidelberg Engineering, Genentech, GlaxoSmithKline, Neuron, Novartis and Pfizer and has received research funding from Bayer HealthCare, Genentech, Novartis and Pfizer. He has also received travel support from Bayer HealthCare and lecture fee from Novartis and Pfizer. Dr Roider is a consultant to Bayer HealthCare. Dr Ogura is a consultant to and has received travel support and lecture fee from Bayer HealthCare. Dr Korobelnik is a consultant to Alcon, Bayer HealthCare, Carl Zeiss Meditec and Thea. He is also an advisory board member in Allergan and Novartis. Dr Simader is a consultant to Bayer HealthCare. Dr Groetzbach is an employee of Bayer HealthCare. Dr Vitti is an employee of Regeneron Pharmaceuticals, Inc. Dr Berliner is an employee of Regeneron Pharmaceuticals, Inc. Hiemeyer is an employee of Bayer HealthCare. Beckmann is an employee of Bayer HealthCare. Dr Zeitz is an employee of Bayer HealthCare. Dr Sandbrink is an employee of Bayer HealthCare.
-
Patient consent Obtained.
-
Ethics approval Institutional Review Boards and Ethics Committee.
-
Provenance and peer review Not commissioned; externally peer reviewed.
Linked Articles
- PostScript