Article Text

Abstract
Aims: To derive an evidence base for the efficacy of two novel optometric primary eye care services in Wales, the Primary Eyecare Acute Referral Scheme (PEARS) and the Welsh Eye Health Examination (WEHE).
Methods: A Donabedian model using structure, process and outcome was applied to evaluate prospectively 6432 individuals attending 274 optometrists within an 8-month period. Telephone interviews and review of optometric and hospital notes were used to determine management appropriateness for patients either managed in optometric practice or referred to the Hospital Eye Service (HES). A Geographic Information Systems analysis determined distances travelled to the optometrist. A cost analysis was used to determine the net cost of the schemes.
Results: 4243 (66%) of the 6432 individuals were managed in optometric practice; inappropriate management was apparent in 1% of individuals. 392 hospital notes were reviewed; 75% exhibited appropriate optometric referrals to the HES. 87% of individuals travelled less than 5 miles to attend an optometrist. The net cost of a PEARS/WEHE consultation was a minimum of £12.
Conclusions: Optometric management within the schemes is acceptable. Good equity of access was achieved at a relatively low net cost per consultation. Agreement on protocols for referral to the HES would enhance the schemes.
Statistics from Altmetric.com
The commissioning of primary eye care services in the community should be based upon equity of patient access and value for money.1–4 In Wales, the Primary Eyecare Acute Referral Scheme (PEARS) and the Welsh Eye Health Examination (WEHE) scheme were introduced in 2003 to provide, respectively, an optometric primary care intervention service to facilitate the early assessment of acute ocular conditions and a case-finding service for ocular disease in patients considered at risk.
Patients requiring a PEARS examination expect to be seen within 24 h of requesting an appointment and undergo investigations considered necessary and appropriate by the optometrist. Patients attending for a WEHE undergo predefined and specific ocular investigations. Both types of examination are free of charge to the patient and, at the time of this evaluation, optometrists received a fee of £38 from the Welsh Assembly Government. Optometrists are the sole providers of the service with patients generally either self-referring or being referred from their general practitioner (GP). In order to participate in the schemes, optometrists are required to pass theoretical modules and practical assessments designed to improve skills in ocular disease recognition and management.
The PEARS and WEHE are consistent with a model that could provide good primary eye care.5 First, community optometrists appear to be able to provide a quality primary eye care service to patients with ocular problems who otherwise would visit their GP. Second, both schemes appear to provide a first point-of-contact in the community for all eligible patients. To evaluate these claims, the following prospective evidence was analysed: care pathway; presenting symptoms; appropriateness of those managed in optometric practice; patient satisfaction with the schemes; outcome of optometric referrals to the Hospital Eye Service (HES); equity of access to an optometrist; and cost of the schemes.
METHODS
The evaluation was undertaken over a period of 8 months (April to December 2006). The cohort comprised 6432 consecutive individuals presenting to 274 optometrists (64% of those in Wales; mean professional registration 19.1 years; SD 10.4; range 1 to 46 years). All individuals had given informed consent for access to their optometric and medical records under the auspices of the Multi Centre Research Ethics Committee for Wales.
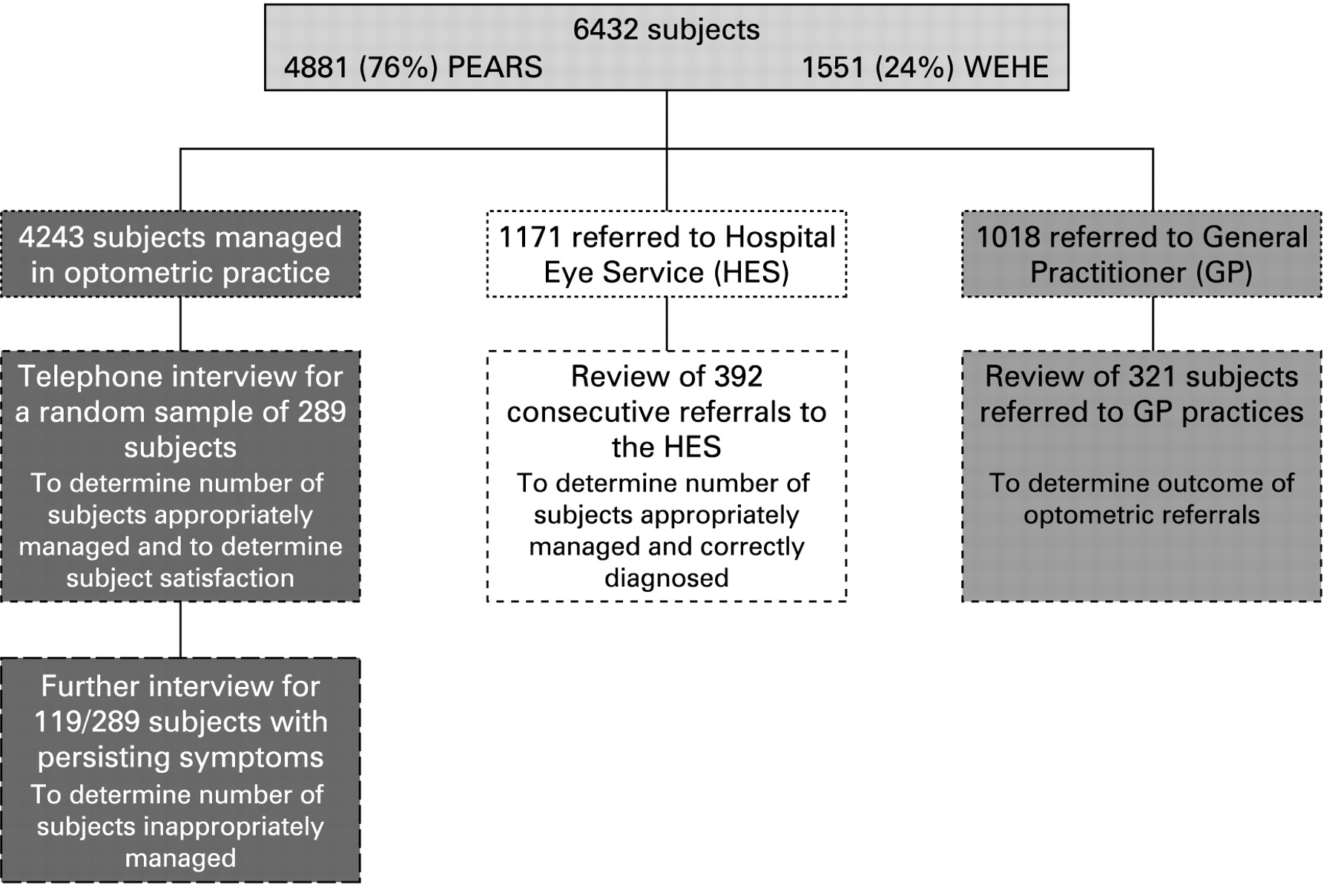
The study (fig 1) was conducted using a Donabedian model of evaluation based upon structure, process and outcome.6

{kind=link}
Flow diagram of evaluation methodology. PEARS, Primary Eyecare Acute Referral Scheme; WEHE, Welsh Eye Health Examination.
The details of the ophthalmic examination from each of the 6432 individuals had been recorded on a standardised record card designed for the evaluation and available in both paper and electronic format. Information from the record cards was entered onto a password-protected and encrypted Access database.
Telephone interview
A total of 289 individuals (yielding 90% power with a 95% CI of 5%) randomly selected from those attending between September and December 2006 underwent a telephone interview by one of two optometrists within a week of attending for a PEARS (73%) or WEHE (27%) consultation. The interviewees (mean age 63.1 years; SD 14.6; range 18 to 94 years) comprised 172 (59.5%) females and 117 (40.5%) males. The telephone interview determined: the management appropriateness of individuals examined in optometric practice; level of satisfaction with the service received from their optometrist; and health-related quality of life.
Individuals reporting persisting symptoms at the first interview and who had been managed in optometric practice received a further telephone interview approximately 1 month later to determine the clinical course of the ocular problem. A 1-month interval was used, arbitrarily, to identify self-limiting conditions. The optometric record cards of those with a persisting ocular problem at the second interview were evaluated to determine appropriateness of patient management in optometric practice.
The level of satisfaction with the service was derived using subscales adapted from those measuring satisfaction with GP consultations7 and was scored on a five-point response scale ranging from “very satisfied” to “very dissatisfied.”
The health-related quality of life was determined using the EuroQol EQ-5D Health-Related Quality of Life (HRQOL) scale.8
Review of HES notes
The outcome of optometric referrals to 11 HES departments was determined for 392 consecutive referrals between August and December 2006.
Referral outcome was evaluated in terms of appropriateness of optometric management and of accuracy of diagnosis and was determined by a consultant ophthalmologist (JMS) and an optometrist with a doctorate (JSP), both of whom resided and practised outside Wales.9 The decision for each case was based upon the optometric and HES notes. The ophthalmologist was the final arbiter. The location of eye disorder recorded in the HES notes was classified according to the WHO ICD 10 coding.10
The ophthalmology management outcome (ie, if an individual was discharged, treated or followed up in the HES) was also used as an outcome measure, since it provides a feasible, acceptable and reliable measure of referral quality.11
Review of GP notes
A three-item tick-box postal questionnaire was used to determine the outcome of optometric referrals to 321 consecutive GP practices between August and December 2006, that is whether individuals had been managed or discharged from GP practice.
Equity of access
The travel time and distance to an optometrist were determined for each individual using Geographic Information Systems (GIS) analysis based upon postcode data.12
Cost of the schemes
The costing model was based on: (a) the fees paid to optometrists for 6432 PEARS/WEHE consultations; (b) the assumption that the 3692 self-referrals to PEARS did not have to consult a GP prior to self-referral (GP consultation costed at £22.00);13 (c) the initial assumption that all 1576 referred by GPs to PEARS/WEHE avoided an HES outpatient consultation (costed at £69.80 per consultation);14 (d) the costs of inappropriate optometric management arising from unnecessary referrals to the HES; and (e) the cost of consultations arising from optometric re-referral to the GP.
RESULTS
The mean age of the 6432 individuals (3751 females, 58%; 2681 males, 42%) attending for a PEARS or WEHE examination was 57.2 years (SD 18.6). The care pathway for the consultation is given in table 1.
Care pathway after optometric examination
Of the 6432 individuals, 4243 (66%) were managed in optometric practice (ie, not referred to healthcare professionals); 1171 (18%) were referred to the HES; and 1018 (16%) were referred to the GP, either for co-management (415; 41%) or for systemic investigation (603; 59%).
Of the 1576 who had been referred to PEARS/WEHE by the GP (table 1), 940 (60%) were managed within optometric practice, 365 (23%) were re-referred to the GP, and 271 (17%) were referred to the HES.
Number and type of presenting symptoms and subsequent management
The most common primary presenting symptom was “unilateral red eye” (1416 of 6432, 22%), followed by “ocular discomfort” (986, 15%) and “flashes and floaters” (601, 9%). The majority of unilateral red eyes (1276 of 1416, 90%) were managed in optometric practice or in conjunction with the GP.
Appropriateness of individuals managed in optometric practice
Three of the 119 individuals with persisting symptoms had been inappropriately managed.
Satisfaction with the optometric service
Of the 289 interviewees, 274 (94.8%) were “very satisfied” and 15 (5.2%) “fairly satisfied” with the optometric service.
Health-related quality of life
The mean self-reported dimension of health was 72% (SD 17.8; range 5 to 100) for responses measured by an analogue scale, and 0.76 (SD 0.25; range −0.35 to 1.0) for those determined by description. The mean was approximately three-quarters of the “best imaginable” health state.
Outcome of optometric referrals to the HES
The mean age of the 392 individuals referred (168 males, 43%; 224 females, 57%) was 59.8 years (SD 19.1). Seventy-five per cent were deemed to have been appropriately managed by the optometrist and 284 (72%) correctly diagnosed.
Forty-nine of the 97 inappropriate referrals (51%) were for uncomplicated posterior vitreous detachment (PVD), with 45 cases correctly diagnosed by the optometrist. Of these 45, 27 had been referred solely on the basis of local protocols implemented by ophthalmologists. Of the remaining 48 inappropriate referrals, two were missed retinal tear/detachment referred solely for flashes and floaters, 34 had non-sight-threatening problems and 14 were normal.
The most frequent referral to the HES (25%), disorders of the “choroid and/or retina,” was appropriately managed in 91% of individuals and correctly diagnosed in 72% of cases. Disorders of the “sclera, cornea, iris and ciliary body” accounted for 81 referrals and were appropriately managed and correctly diagnosed in 84% and 73% of cases, respectively. Forty-one (10%) of referrals were for “asymptomatic eye disease,” including open angle glaucoma (OAG): of these, 35 (85%) were appropriately managed and 71% appropriately diagnosed.
Of the 392 individuals, 286 (73%) attended for at least two follow-up HES visits. Of the remaining 106, 85 (22%) were discharged at the first visit without treatment; of these, 37 (44%) had initially presented with symptoms of photopsia. Twenty-one cases received treatment prior to discharge at the first visit; of these, 16 (4%) received chloramphenicol eye-drops only.
Outcome of optometric referrals to the GP
Insufficient replies were received (five out 321) to enable referral outcomes to be evaluated.
Equity of access
Of the 6432 individuals, 87.4% travelled less than 5 miles to an optometrist (Mid and West Wales, 78.6%; North Wales, 80.2; South Wales, 97.6%).
Cost of the schemes
The gross cost incurred for PEARS/WEHE was approximately £244 000, and the resource utilisation avoided (ie, the savings on unnecessary HES and GP consultations) was approximately £191 000. The net cost of the 6423 examinations over the 8-month period of the evaluation was approximately £77 000, or a cost of approximately £12 per PEARS or WEHE consultation.
It can be postulated that, prior to PEARS/WEHE, not all 1576 GP referrals to the schemes would have been referred to the HES. It was considered that a minimum of 44% would have been referred by the GP to the HES (eg, corneal disorders, iritis, posterior segment disorders, and symptoms of flashes and floaters). A cost model based upon a 50% referral to the HES with the remainder consulting the GP on two further occasions yields a cost of approximately £15 per PEARS or WEHE consultation.
DISCUSSION
The PEARS and WEHE provide a unique primary eye care triaging and ocular case finding service. The evidence indicates that these schemes are clinically effective, provide a satisfactory service to the patient and combine ease of access at relatively low cost. Optometrists managed 66% of all individuals in practice without referral to other healthcare professionals. They made satisfactory clinical judgements for individuals remaining in their care and for those they referred. These findings provide a basis for the development of future policy on primary eye care in the community.
The optometric management of individuals referred to the HES was appropriate in 75% of cases: however, this figure is confounded by cases of posterior vitreous detachment (PVD). It was felt that uncomplicated PVD did not warrant referral, and so these cases were classified as inappropriate referrals. However, a number of HES departments in Wales utilise local protocols in which optometrists are required to refer uncomplicated PVD. The percentage of appropriate optometric referrals to the HES increased from 75% to 82% when correctly diagnosed uncomplicated PVD cases, referred according to local protocol, are considered. Implementation of an all-Wales protocol for the management of uncomplicated PVD should prevent unnecessary referrals to the HES.
The appropriateness of optometrist referrals to the GP could not be analysed due to insufficient numbers of returned questionnaires. Therefore, the ability of optometrists to case-find systemic disease remains unknown.
Optometrists participating in the study were aware that their notes would be reviewed. This could have introduced some positive bias in that participating optometrists may have demonstrated increased clinical vigilance.
The PEARS and WEHE exist alongside the less costly NHS-funded and private sight tests in which optometrists have a statutory duty to detect, rather than manage, ocular injury or disease. The PEARS and WEHE models differ from the sight test in that a structure for the management of ocular conditions is implemented and formalised. Previous studies investigating the referral patterns to the HES resulting from a sight test indicate that optometrists tend to refer posterior segment conditions, whereas GPs refer anterior segment conditions.15–17 In this study, a substantial proportion of optometric referrals to the HES were for anterior segment conditions. This change in referral pattern highlights the difference between the PEARS and WEHE and the standard NHS-funded and private sight tests. The sight test and the PEARS and WEHE are so different that a comparison of the outcome of the two was considered to be unnecessary.
Almost all new cases of OAG are identified from opportunistic case finding by optometrists, and the process is associated with a significant proportion of false-positive outcomes, estimated to be as high as 50%.18–20 In this study, only four of 23 individuals (17.4%) referred for OAG were discharged. Although these numbers are small, the training provided for optometrists in the detection of OAG as part of the accreditation process for PEARS and WEHE could explain the lower false-positive outcome. Targeted training for optometrists on the characteristics of the glaucomatous optic nerve head reduces the number of false-positive referrals to the HES.21 The improved discrimination for OAG, if representative, would reduce waiting times for outpatient appointments at glaucoma clinics as well as yielding further cost savings.
Telephone interviews and a review of clinical notes were used to establish whether individuals discharged from optometric practice were managed appropriately. Telephone interviews are a useful method to ascertain such outcomes and are commonly utilised in medicine.22 In all inappropriately managed cases, the letter from the optometrist to the GP contained insufficient information for the GP to act upon. Discussion of specific relevant case histories has already been undertaken with those optometrists responsible for cases of inappropriate management.
Approximately 1–3% of a GP’s workload is concerned with ocular problems.23 24 In this study, most patients referred by the GP were managed within optometric practice. This implies that optometrists have the expertise to manage such patients. The majority of GPs receive inadequate ophthalmology training,25 26 and the shift from GP to optometrist as a service provider should release valuable GP resources for allocation elsewhere. However, the ensuing lack of ophthalmic experience may adversely effect GPs’ ability to recognise primary ophthalmic disease and that associated with systemic disease.
The PEARS and WEHE model of primary eye care has been shown to be clinically effective, acceptable and accessible, and to be provided at relatively low cost. A randomised controlled trial of community ophthalmic care against the PEARS and WEHE model would provide further evidence, but the impact of potential regulatory and technological developments should also be considered. Optometric practices are not required to meet the same standards, in terms of infection control, provision of immediate life support, audit, appraisal and indemnification of professional staff as both the HES and the private ophthalmological sector. Costs would be incurred if these standards were also applied to providers of the WEHE. Digital imaging of the posterior segment is becoming routine for the diagnosis and management of glaucoma, and this may also have consequences for optometric practice. The future commissioning of NHS primary eye care services depends on informed decision-making. The study provides a preliminary evidence base to develop and implement strategies for services in the primary eye care sector.
REFERENCES
Footnotes
Funding: Funded by the Welsh Assembly Government. The funder had no involvement with the research.
Competing interests: None.
Ethics approval: Ethics approval was provided by the Multi Centre Research Ethics Committee for Wales.
Patient consent: Obtained.