Article Text

Abstract
Background: There has been considerable recent interest in the impact of unilateral visual impairment on functional status and wellbeing, particularly in relation to second eye cataract surgery.
Aim: To determine if unilateral visual impairment has a measurable impact on health related quality of life (HRQOL) in an older community, as assessed by the generic, multidimensional 36 item short form health survey (SF-36).
Methods: All participants of the second cross sectional Blue Mountains Eye Study (n = 3508) were invited to attend comprehensive eye examinations and complete an SF-36 questionnaire. Unilateral visual impairment was defined as visual acuity (VA) <6/12 in the worse eye and ≥6/12 in the better eye. Mild visual impairment was defined as VA <6/12 but ≥6/24, moderate as VA <6/24 but ≥6/60, and severe (blindness) as VA <6/60 in the worse eye. Cases with amblyopia (n = 48) were excluded.
Results: Complete data were available for 3108 participants; 227 (7.3%) had unilateral visual impairment (148 mild, 29 moderate, 50 severe). Moderate to severe non-correctable unilateral impairment was associated with poorer SF-36 profiles. After adjusting for age and sex, this group had significantly poorer scores than the unimpaired group in three of eight domains (p<0.05); limitations as a result of physical problems, social function, limitations because of emotional problems, and in the mental component score. Mental domains were more affected than physical domains. Unilateral impairment from undercorrected refraction did not measurably affect HRQOL.
Conclusions: Moderate to severe non-correctable unilateral visual impairment caused by eye diseases such as cataract had a measurable impact on HRQOL.
- unilateral visual impairment
- quality of life
- SF-36
- epidemiology
- visual function
- cataract surgery
- Blue Mountains Eye Study
Statistics from Altmetric.com
- unilateral visual impairment
- quality of life
- SF-36
- epidemiology
- visual function
- cataract surgery
- Blue Mountains Eye Study
The impact of bilateral visual impairment on health related quality of life (HRQOL) and independent living has been well documented1 including an increased mortality risk,2–4 earlier nursing home placement,5 falls,6 and increased use of community support services.7 The impact of unilateral visual impairment on functional status and wellbeing is more subtle and less well understood. Its impact, however, has been generating increasing interest in recent years, particularly in the context of second eye cataract surgery.8
The estimated cost of cataract surgery in the United States in 1991 was US$3.4 billion.9 In the United Kingdom, it has been estimated that approximately one third of cataract surgery is performed on second eyes.10 Owing to constraints on healthcare budgets, there have been suggestions that public funding for second eye cataract surgery could be rationed. Many recent studies have indicated that this would be a detrimental move which could adversely affect functional status, independence, and HRQOL.11–20
The Blue Mountains Eye Study (BMES) is a well described cohort study of vision and common eye diseases. We aimed in this population sample to determine whether unilateral visual impairment had a measurable impact on HRQOL, as assessed by the generic, multidimensional 36 item short form health survey (SF-36).21 This instrument is a validated health outcome measure that has been widely used to assess the impacts on quality of life in many different medical conditions.22–26
PATIENTS AND METHODS
The BMES is a well described population based survey in an urban population aged 49 years or older resident in two postcode areas of the Blue Mountains region, west of Sydney, Australia. Methods used in this survey have already been described.27 The present report uses findings from the second cross section of this population.
BMES I identified 4433 eligible non-institutionalised permanent residents in a door to door census conducted during 1991, of whom 3654 (82.4%) participated in the examinations during 1992–4. After 5 years, BMES I participants were invited to attend repeat examinations during 1997–9 (BMES IIA). By the time these commenced, 543 people had died (14.9%) and 2335 (75.1%) were re-examined. A repeat door to door census conducted in 1999 of the same area identified 1378 additional eligible permanent residents who had moved into the area or were now aged 50 or older. We examined 1174 (85.2%) of this group during 1999–2000 (BMES IIB). Cross section 2 thus comprised 3509 participants from BMES IIA and IIB.
Participants were invited to attend a comprehensive eye examination that included measurement of distance logMAR visual acuity, before and after subjective refraction using the ETDRS method,27 automated perimetry, and lens and stereo retinal photography.
Before attending, we asked participants to complete a detailed questionnaire, which was mailed after appointments were made. Included were questions about visual function and diet, and the SF-36 quality of life, self administered questionnaire.21 This instrument contains 36 items, measuring eight dimensions of health and wellbeing: “physical functioning,” “role limitation due to physical problems,” “bodily pain,” “general health perceptions,” “vitality,” “social functioning,” “role limitation due to emotional problems,” and “mental health.” Each dimension was scored from 0 (worst possible health state) to 100 (best possible health state) by coding, summating, and transforming relevant item scores. Missing values were substituted by averaging other items if the number of missing items was less than half the total number of items in that dimension. No substitution was used for dimensions with only two items. The eight dimensions comprise two domains “physical” and “mental,” scored as physical component scores (PCS) and mental component scores (MCS). These are summary measures calculated using factor analysis and Australian normalised scores.28
Unilateral visual impairment was defined as visual acuity (VA) <6/12 in the worse eye and ≥6/12 in the better eye. Mild visual impairment was defined as VA <6/12 but ≥6/24, moderate impairment as VA <6/24 but ≥6/60, and severe impairment (blindness) as VA <6/60. People with unilateral impairment attributed to amblyopia were excluded, as their inclusion would have diluted assessment of the impact of changes in unilateral visual acuity. The impact from unilateral visual impairment which was correctable by refraction was also assessed.
Statistical Analysis System (sas, version 6.12 for Windows; SAS Institute, Cary, NY, USA) was used for statistical analyses. Age and sex adjusted values are presented.
RESULTS
Participants had a mean age of 66.7 years (range 49–98 years) and 57% were female. Of the 3508 participants in the second BMES cross section, complete data sets that included SF-36 questionnaires were available for 3153 participants (89.9%). Bilateral visual impairment, based on presenting VA, was present in 237 participants (7.5%), unilateral impairment was present in 543 subjects (17.2%), and 2373 (75.3%) had no visual impairment, as shown in Figure 1. After refraction, 67 participants (2.1%) were still visually impaired in both eyes, while 264 (8.4%) remained impaired in one eye only. After further exclusion of subjects with amblyopia, there were 497 people (16.0%) with unilateral visual impairment at presentation and 227 (7.3%), after refraction. Of these 227 subjects, 148 participants had mild and 29 had moderate unilateral visual impairment while 50 were unilaterally blind. Owing to the relatively small numbers, cases with moderate and severe unilateral visual impairment were pooled for the analysis of SF-36 profiles.

Flow chart showing number of people with bilateral and unilateral visual impairment (VI), based on presenting and best corrected visual acuity: the Blue Mountains Eye Study second cross section.
Increasing age was strongly associated with poorer SF-36 profiles. This worsening age related trend was demonstrated for all SF-36 dimensions (Fig 2) and for the two component scores (data not shown; p<0.001). After adjusting for age, women had slightly poorer SF-36 profiles than men (data not shown). This sex difference, however, was statistically significant for all dimensions (p<0.05), apart from “general health” (p = 0.41) and “role limitation due to emotional problems” (p = 0.14).

Sex adjusted mean SF-36 scores in the Blue Mountains Eye Study (second cross section) by age group.
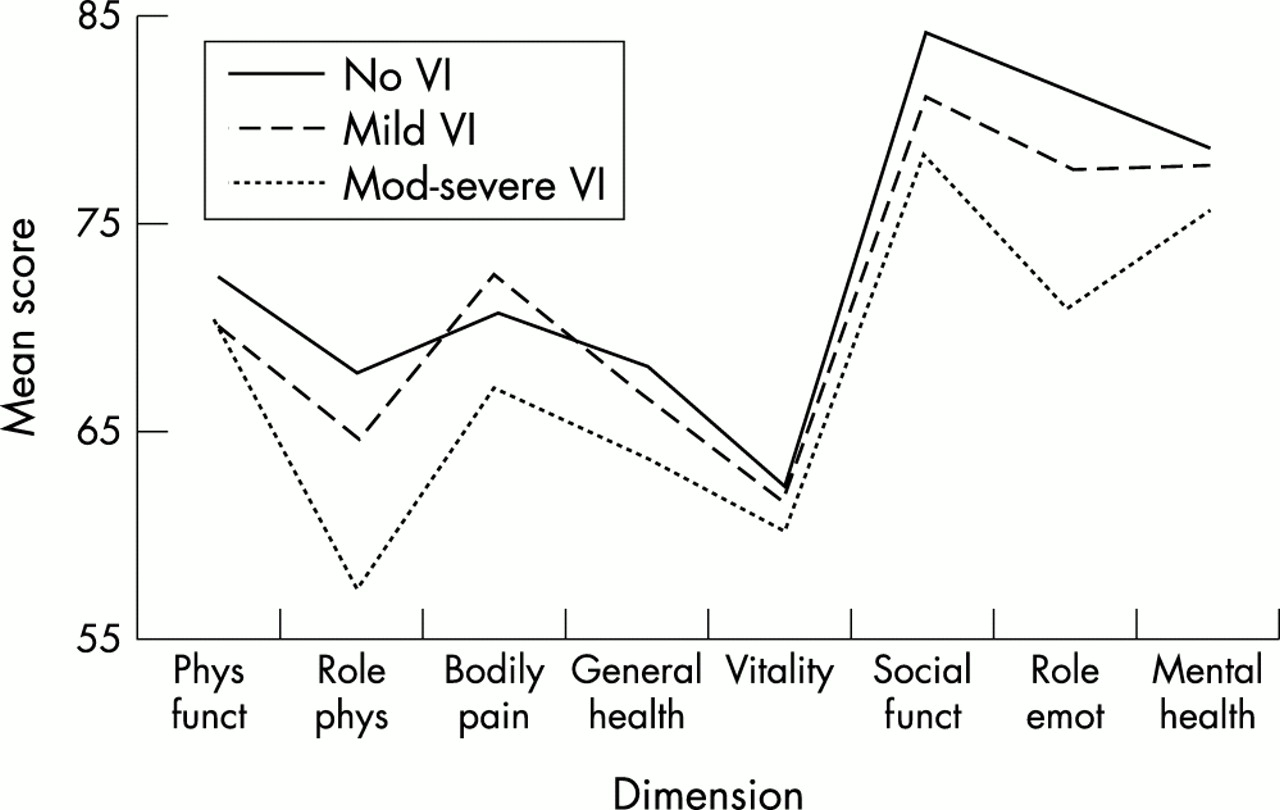
Table 1 shows that there were no overall differences in mean age and sex adjusted SF-36 scores between people with and without unilateral visual impairment. Unilateral visual impairment correctable by refraction had no measurable impact on the mean scores. Unilateral non-correctable impairment modestly affected one dimension; “role limitation due to physical problems” (p = 0.04), but there was no impact on overall physical or mental summary scores. Stratification of the non-correctable group, however, demonstrated a gradient with poorer SF-36 profiles seen for increasing severity of unilateral visual impairment, as shown in Figure 3. Table 2 shows that, while relatively modest, the impact was statistically significant only for people with moderate to severe impairment. After adjusting for age and sex, this group had significantly poorer mean scores than people with no visual impairment in three of eight dimensions (p<0.05); “role limitation due to physical problems” (15% lower), “social functioning” (7% lower), “role limitation due to emotional problems” (13% lower), and in the mental component score. There was a greater effect on the mental domain than the physical domain.
Mean age and sex adjusted SF-36 scores of Blue Mountains Eye Study participants with non-correctable, correctable, and no unilateral visual impairment (VI)
Mean age and sex adjusted SF-36 scores of Blue Mountains Eye Study participants with moderate to severe, mild, and no non-correctable unilateral visual impairment (VI)

{kind=link}
{kind=link}
{kind=link}
Age and sex adjusted mean SF-36 scores in the Blue Mountains Eye Study (second cross section) with moderate to severe (n = 79), mild (n = 148), and no (n = 2822) non-correctable unilateral visual impairment (VI).
DISCUSSION
In the past decade, there has been considerable interest in examining the effects of unilateral visual impairment, particularly in relation to second eye cataract surgery in the context of constrained healthcare expenditure.8 Our study demonstrates a modest, but statistically significant impact on a general health measure of quality of life and independent functioning in the presence of moderate to severe non-correctable unilateral visual impairment. This was present in only three of the eight SF-36 domains, after age-sex adjustment and only for moderate to severe impairment. There was no measurable impact from correctable unilateral impairment.
Our data confirm findings from many recent reports that have demonstrated a range of benefits from second eye cataract surgery.8,13,14,16,20 These have included improvements in subjective visual function,20 binocular and stereo acuity,13,14 and better performance on questionnaire instruments that target general functioning (for example, the Sickness Impact Profile16), eye specific functioning (for example, the Visual Function 14 item questionnaire8,16), or quality of life.13
In a randomised trial of the effectiveness of second eye cataract surgery, Laidlaw et al13 reported an 11%–30% difference in visual symptoms and quality of life measures between routine and expedited surgery. Javitt et al20 showed that patients with bilateral cataract induced visual impairment who underwent cataract surgery in both eyes had significantly improved subjective visual function than those with unilateral cataract surgery alone. Talbot and Perkins14 showed that second eye cataract surgery increased the proportion of older people who satisfied driving licence requirements from 52% to 86%. Guthauser and Flammer29 reported a subgroup of patients with central visual field impairment who had the greatest threshold for recovery after cataract surgery.
The functional improvement in vision from second eye cataract surgery could be explained by better monocular and binocular contrast sensitivity.14,19 Talbot and Perkins14 also showed that 66% of their participants had improved binocular visual acuity and stereoacuity from 32% to 90%, previous ocular dominance was restored in 44%, and there were improvements to binocular horizontal and vertical field of vision. Laidlaw and Harrad19 have also stated that glare reduction may also play a part, with a reduction from 86% to 41%, in the proportion of patients with symptomatic glare after second eye cataract surgery, despite previous reports of increased glare associated with posterior chamber lens implants.30
There are well described objective improvements to visual acuity following second eye cataract surgery in terms of stereopsis and visual acuity that can be explained by binocular summation. Objective tests, however, have not demonstrated significant binocular inhibition from second eye cataract.19 Thus, the disability resulting from visual impairment does not stem from the loss of visual acuity or subjective aspects of visual function such as glare alone. Both visual8,31 and functional8,13,19 effects need to be addressed independently. Our study has attempted to examine the impacts of unilateral visual impairment on HRQOL, as measured by the SF-36, an instrument that includes both physical and mental domains. We excluded cases where unilateral visual impairment was due to amblyopia, as their inclusion could dilute our findings and this disorder has uncertain public health importance.
Data from the United Kingdom indicate that cataract surgery will improve objective vision with minimal complications when well established guidelines are used.32 Most past studies have looked at objective changes in vision such as binocular acuity, contrast sensitivity, and stereopsis. The trial reported by Laidlaw et al13 showed benefits from second eye cataract surgery in reducing self reported difficulties, despite only marginal improvements in binocular visual acuity. A large observational UK study of cataract surgery showed significant gains in health and vision related quality of life outcome measures from first eye surgery with additional significant gains at 1 year, if second eye surgery was also performed.16
The SF-36 questionnaire has been shown to discriminate well between Australians with and without various health conditions, in a validity study conducted on 555 subjects in a National Heart Foundation survey.33 Our age and sex specific SF-36 findings (in part, shown in Fig 2) are also very close to the SF-36 norms for a much larger population sample, provided by the 1995 Australian Bureau of Statistics National Health Survey.28 The number of domains with significant age-sex adjusted differences between people with and without moderate to severe unilateral non-correctable visual impairment (three of eight domains, plus the mental component score) is similar to findings from a number of recent reports using this instrument.34 In our study, moderate to severe bilateral non-correctable visual impairment was associated with a substantially greater impact than unilateral impairment, and was of a magnitude similar to that from major systemic diseases, such as heart disease, stroke, diabetes, and cancer (data not shown). Changes in SF-36 scores that differ between groups by two or more points on the scale of 0 to 100 have been shown to be clinically or socially meaningful.35 In our study, at least this magnitude of difference was demonstrated for all eight domains (in Table 2). Importantly, the completion rate (89.9%) of the SF-36 questionnaire by participants in our study is substantially higher than in most other reports using the self administered version, mailed to respondents (for example, 79.2%36).
Our study has a number of limitations, including: (1) insufficient power to examine the impacts on HRQOL from the different causes of visual impairment (for example, cataract versus macular degeneration) and (2) lack of concurrent comparison with questionnaires designed to measure visual functioning. The strengths are its population base and relatively high completion rate (89.9%) by study participants.
In summary, this study has demonstrated modest, but statistically significant detrimental effects on a general measure of HRQOL associated with unilateral non-correctable visual impairment in an older population sample. Importantly, this was only found for moderate to severe levels of visual impairment and for three of the eight SF-36 dimensions, plus the mental component score. Nevertheless, our study highlights the potential for significant morbidity from unilateral eye diseases, such as unoperated cataract, particularly in the psychosocial domain, and the potential for improvement with treatment. These data provide support for the notion that cataract surgery on the second eye of patients with bilateral cataract is likely to provide significant and measurable functional benefits.
Acknowledgments
This study was supported by the Australian National Health and Medical Research Council (grant Nos 974159 and 991407) and the Westmead Millennium and Save Sight Institutes, University of Sydney.