Article Text

Abstract
AIMS To study the refractive development in children with Down's syndrome longitudinally.
METHODS An unselected population of 60 children with Down's syndrome was followed with repeated retinoscopies in cycloplegia for 2 years or more (follow up 55 (SD 23) months). Accommodation was assessed with dynamic retinoscopy.
RESULTS From longitudinal spherical equivalent values of the right eye, three main categories of refraction were defined: stable hypermetropia (<1.5 D difference between the first and last visit) (n=34), increasing hypermetropia (“hypermetropic shift”; ⩾1.5 D difference) (n=11), and decreasing hypermetropia/development of myopia (“myopic shift”; ⩾1.5 D difference) (n=9). Patients with anisometropia (n=6) were evaluated separately. In the stable hypermetropia group three sublevels were chosen: low (⩽+2.0 D at the last visit), moderate (+2.25 to + 4.0 D), and high (>+4.0 D). An accommodation weakness was found in 55% of the children. Accommodation weakness was significantly less frequent in the stable, low grade hypermetropia group (22%) than in all the other groups (p=0.008). The frequency of astigmatism ⩾1.0 D at the last visit was 57%, the direction of axis being predominantly “with the rule.” All the eyes with oblique astigmatism had a side specific direction of axis; the right eyes belonging to the 135° axis group and the left eyes to the 45° axis group.
CONCLUSION A stable, low grade hypermetropia was significantly correlated with a normal accommodation. Accommodation weakness may be of aetiological importance to the high frequency of refractive errors encountered in patients with Down's syndrome. A striking right-left specificity in the oblique astigmatic eyes suggests that mechanical factors on the cornea from the upward slanting palpebral fissures may be a major aetiological factor in the astigmatism.
- accommodation
- astigmatism
- children
- Down's syndrome
- refractive errors
Statistics from Altmetric.com
The increased frequency of refractive errors in individuals with Down's syndrome has been documented by many authors.1-9 However, most studies have been based on selected populations.1-6 In addition, all reports so far have been cross sectional studies.
Hoping to elucidate new aspects of this issue, we have studied the refractive development in an unselected Down's syndrome childhood population by repeated examinations during the past 10 years. To our knowledge, this is the first longitudinal study on refractive errors in children with Down's syndrome.
Subjects and methods
STUDY POPULATION
Seventy seven children with Down's syndrome born during the years 1988–99 in Hordaland County, Norway (population 416 000, annual births 6000), were referred from Vestlund Habilitation Resource Center to our department for an ophthalmological examination. This centre coordinates the habilitation of all Down's syndrome children in the county. To ensure a population based study design, the files of the regional laboratory for cytogenetics were examined. In this way we found 16 dropouts. Thus, the total number of patients with Down's syndrome born in our county during these years was 93, giving a mean annual incidence of 1.25 per 1000 live births (range 0.63–2.12).
Among the 16 dropouts, four had died and three had moved to other parts of the country. The other nine children were invited for an eye examination, which six of them attended. Valid data on previous refraction by other ophthalmologists could be obtained, and they were included in the study. Another six children moved to our region during the study period and were included in the study with successive examinations. Thus, 89 children with Down's syndrome born in the years 1988–99 were examined. Among these, 40 had their first examination during the first year of life (mean age at examination 7.1 (SD 3.0) months, range 3–12). Cross sectional data from these 40 infants will be presented separately.
Patients with follow up time <2 years (n=29) were excluded from the longitudinal study. The group of children with Down's syndrome thus followed for ⩾2 years with repeated eye examinations consisted of 60 children (30 girls and 30 boys). Mean follow up time was 55 (SD 23) months (range 24–115). With very few exceptions, all the examinations were done by one of the authors (OHH). In the whole longitudinal study group the mean age at the first examination was 21 (SD 14) months (range 3–61).
Informed consent was obtained from the parents, and the study was approved by the regional committee for medical research ethics.
REFRACTIVE MEASUREMENTS
Retinoscopy in cycloplegia was performed using cyclopentolate 1% eye drops twice 30 minutes before the examination. Astigmatism was recorded as minus cylinders. The axis of astigmatism was classified as follows: 180 (SD 15)° (“180° meridian” or “with the rule”), 90 (SD 15)° (“90° meridian” or “against the rule”), 16–74° (“45° meridian”), and 106–164° (“135° meridian”).
To evaluate the axis of oblique astigmatism in a mentally normal population, we used the preoperative refractive data from the excimer laser clinic in our department. Only patients referred for primary, uncomplicated refractive errors were included. Eyes with cylindrical power of <1.0 D were excluded. Thus, our control group included 365 eyes (172 right eyes, 193 left eyes) with astigmatism ⩾1.0 D.
ACCOMMODATION
During the past 2–3 years of the study, each examination included an evaluation of the accommodative function with dynamic retinoscopy. Several authors have found dynamic retinoscopy valuable in assessing the accommodative function, especially in children and in the mentally retarded.10-13 In most of these studies, the fixation target is mounted on the retinoscope, and the observer looks for the “breakdown” of the neutral retinoscopic reflex while constantly moving closer to the child. Because many of our Down's children became scared as the examiner moved close to them, the technique was modified as follows. In case of myopia, or hypermetropia > +2.0 D, the child should wear his/her distant glass correction. Sitting about 50 cm in front of the child, the examiner observes the retinoscopic streak light movement while the child is looking straight ahead with both eyes open. A small picture that attracts interest (Lang's cube) is then introduced 20–30 cm in front of the child. The child is constantly encouraged to fixate the near target. If normal accommodation is present, the examiner observes a very distinct shift from “with” movements to “against” movements. Such a response was classified as “normal.” If, when presenting the accommodative target, this clear shift did not take place in spite of a cooperative child, the accommodation response was classified as “accommodation weakness.” The test was repeated three or more times.
VISUAL ACUITY
In infants and small children the visual acuity was tested with the Teller acuity card test. In older children we used an optotype test, mostly the Østerberg chart or the LH chart. In the most cooperative children, ordinary Snellen optotypes were used. Amblyopia was defined as a difference in visual acuity between the two eyes of more than one line on the acuity chart.
STATISTICS
The data were analysed statistically in the spss 9.0 program, using the χ2 test and the Fisher's exact test. p = 0.05 was chosen as the level of significance.
Results
CROSS SECTIONAL DATA IN INFANTS
Twenty one (53%) of the infants were emmetropic or hypermetropic <+2.0 D, while 16 (40%) were hypermetropic between +2.0 and +5.25 D. There were three myopic children, all within –1.5 D. Clinically significant astigmatism (⩾1.0 D) was present in 21 of 40 infants (53%). In all but one case the astigmatism was bilateral. In one patient, the axis was “against the rule” bilaterally, in all the other cases (95%) there was a “with the rule” astigmatism.
LONGITUDINAL STUDY
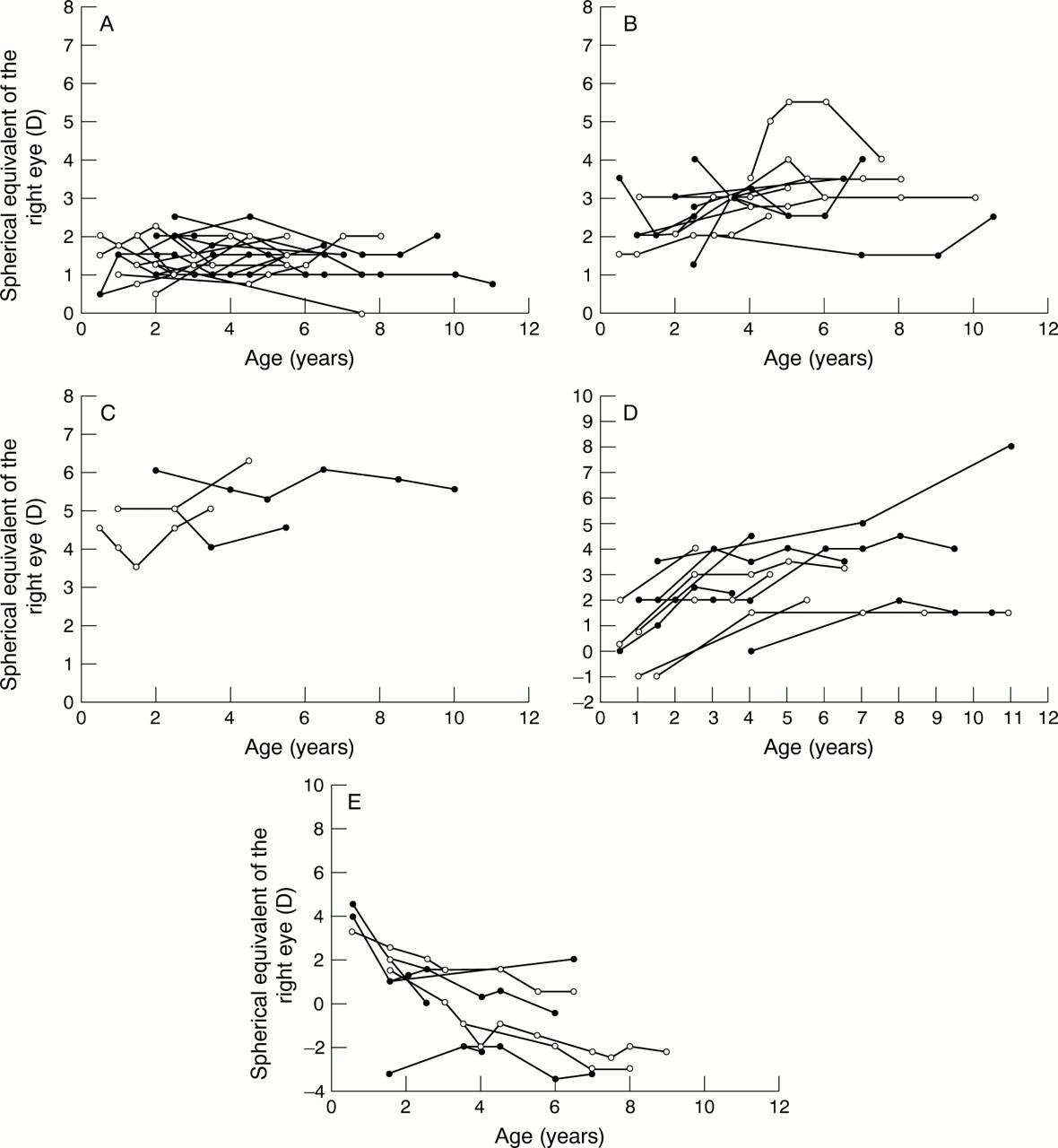
Six patients with clinically significant anisometropia at the last examination were regarded as one group. According to the development of the spherical equivalent of the right eye, the other 54 patients were classified into three main groups, presented in Table 1: group 1 stable hypermetropia (at different levels) (n=34); group 2 increasing hypermetropia (n=11), and group 3 decreasing hypermetropia or development of myopia (n=9) (see Table 1 for the detailed definitions). The individual longitudinal curves for each subgroup are shown in Figure 1A–E.
Longitudinal refractive development in 60 children with Down's syndrome

Individual curves of spherical equivalent values from children with Down's syndrome and stable, low grade hypermetropia (A), stable, moderate hypermetropia (B), stable, high grade hypermetropia (C), increasing hypermetropia (D), and decreasing hypermetropia or development of myopia (E).
In group 2 (“hypermetropic shift”) a level of stability (defined as three consecutive measurements differing ⩽0.5 D) was reached in five patients (45%), mean age at stability was 5.4 years (range 4–8 years). In group 3 (“myopic shift”) only one patient demonstrated stability (11%). This difference was not statistically significant.
ASTIGMATISM
Nineteen children (group A) had no clinically significant astigmatism during the study period. Seven children (group B) had a significant astigmatism at an early age, but it disappeared during the follow up period. The mean age at which the astigmatism disappeared in this group was 40 (SD 16) months (range 19–71). None of these patients had cylindrical values above 1.5 D.
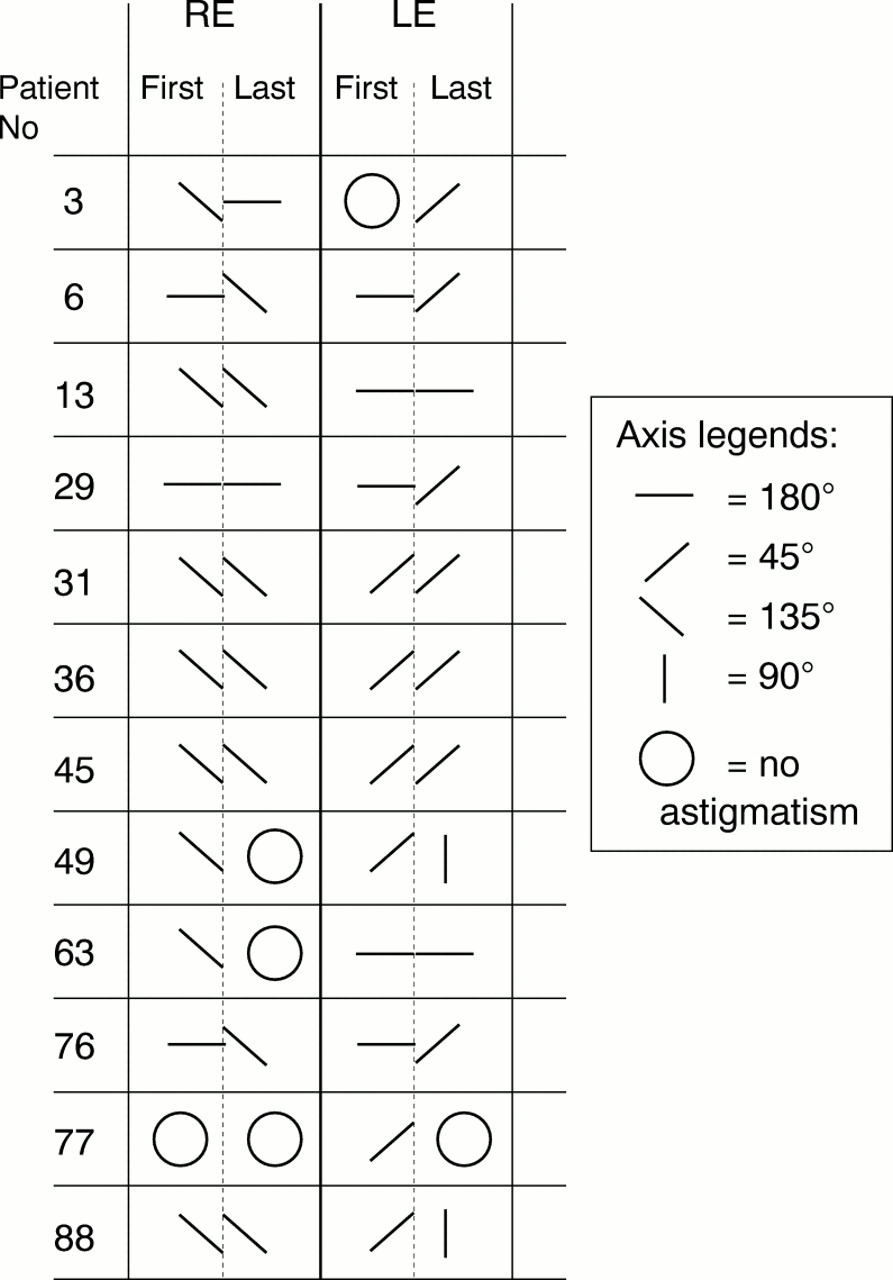
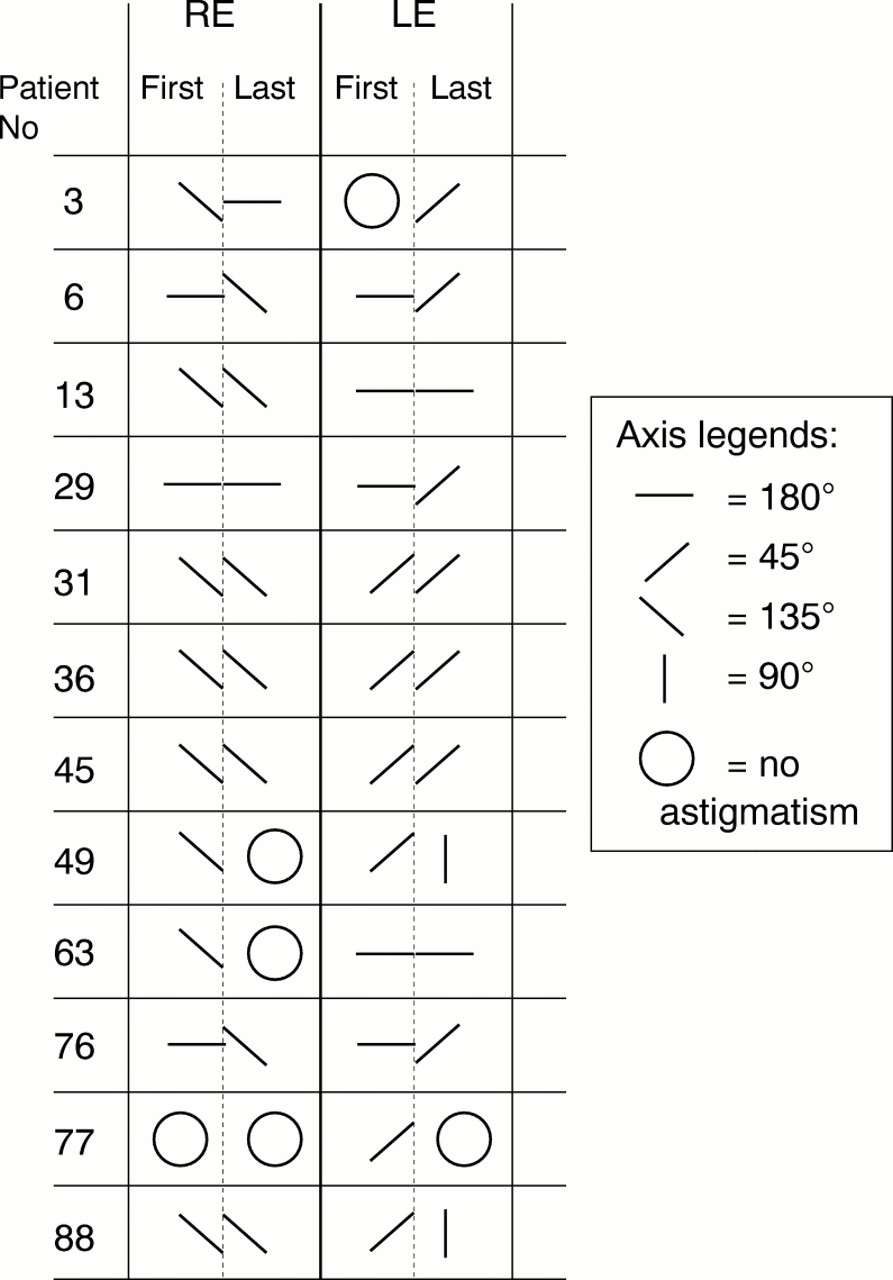
Thirty four patients (57%) had an astigmatism ⩾1.0 D in one or both eyes at the last visit (group C). In 19 patients the axis remained unchanged in the 180° meridian throughout the study period (upper part of Table 2). Three patients with “against the rule” astigmatism also had stable axes (middle part of Table 2). The lower part of Table 2 shows data from the 11 patients in group C with an oblique astigmatism at some point of the study period. All eyes that changed axis during the follow up period (n=8) belonged to this subgroup (in bold). At the last examination, nine patients had an oblique astigmatism in one or both eyes. All the right eyes with oblique astigmatism had their axes in the 135° meridian, while all the left eyes had their axes in the 45° meridian. Figure 2 shows the axes of all the 12 patients with oblique astigmatism at any point of the study.
Individual longitudinal data on 34 children with Down's syndrome with clinically significant astigmatism at the last examination (group C)
{kind=link}
{kind=link}
Direction of axis in the left and the right eyes in 12 children with Down's syndrome with oblique astigmatism. The signs in the columns “first” and “last” show the direction of the astigmatism when the astigmatism was first noticed and at the last examination, respectively (patient numbers correspond with Table 2).
In the control group of patients referred to our excimer laser clinic, the right and left eyes with oblique astigmatism were equally distributed to the 45° axis and the 135° axis.
ACCOMMODATION
Accommodation weakness was found in 33 patients (55%) (Table 3). However, the frequency was lower in the stable, low grade hypermetropic group than in the other groups (χ2 = 14.7; df=5; p = 0.008). Among those tested at two or more visits (n=40), six changed from “normal” to “weak,” while one child changed from “weak” to “normal.”
Accommodative ability in different refractive groups among 60 children with Down's syndrome
VISUAL ACUITY
Visual acuity could be evaluated in 53 children (88%) in the longitudinal study group (Table 4). In 27 children visual acuity could be recorded in each eye separately, while in 26 cases only binocular testing was possible. Only one of the children tested monocularly had a difference between the two eyes of more than one line on the acuity chart.
Visual acuity in the better eye in 60 children with Down's syndrome
Discussion
DEVELOPMENT OF SPHERICAL EQUIVALENT
This study shows that about one third of the children with Down's syndrome (group 1a) had stable refractive values around emmetropia or low hypermetropia throughout preschool and early school age. Stable, but higher, values of hypermetropia were demonstrated in about one fourth of the children. Of special interest are the “hypermetropic shift” and “myopic shift” groups, leading to a persistent wide distribution of refractive values. In a normal refractive development, a low to medium grade hypermetropia with a wide distribution is present in infancy.14 ,15 This corresponds well with our findings in the Down's syndrome infant group. During the second year of life, the mean refraction normally changes towards emmetropia or slight hypermetropia. At the same time the distribution of refractive values narrows (emmetropisation).16-20 Previous cross sectional studies9 ,21 indicate that this normal process does not occur in patients with Down's syndrome. Our longitudinal data support and further characterise this refractive distribution in children with Down's syndrome.
Inside the “hypermetropic shift” group, there were five patients (45%) reaching a level of stability, while in the “myopic shift” group only one patient stabilised (11%). Although this difference is not statistically significant, it may indicate that a refractive development in a myopic direction in individuals with Down's syndrome is more likely to continue into high and disabling values. This is also supported by clinical experience and reported by others.21
The present study confirms the high frequency (55%) of accommodation weakness among children with Down's syndrome reported by others.13 ,22 ,23 Interestingly, our data demonstrate that the stable, low grade hypermetropia group (corresponding to a normal refractive development) had a significantly lower frequency of accommodation weakness than the other refractive groups. This association between an accommodation weakness and a failing emmetropisation does not prove a causative relation. However, several animal studies have shown that optical defocus on the retina induces compensating eye growth.24-26 ,27 This supports the view that reduced accommodation in early age, causing a blurred retinal image for objects at near, may be of aetiological importance for the abnormal refractive development in children with Down's syndrome. Obviously, there must be additional factors, as a reduced accommodation would always shift the optical focus behind the retina and thus induce a myopic shift. This mechanism, therefore, does not explain the cases with increasing hypermetropia.
In addition to a high proportion of accommodation weakness in our material, six of the 40 patients who were repeatedly examined for accommodation showed a change from normal to defect accommodative function. This could indicate that an accommodative ability initially present might later be weakened or lost.
The underlying mechanisms accounting for the reduced accommodation remain unclear. Such factors may be central28 or peripheral in origin.
DEVELOPMENT OF ASTIGMATISM
The prevalence of astigmatism in our Down's syndrome infant group (53%) was comparable with that of normal infants (Table5).20 ,29-34 However, it was considerably higher than that reported in Down's syndrome infants by Woodhouseet al. 9 The present study strongly indicates that “with the rule” astigmatism is the predominant type of astigmatism in infants with Down's syndrome. This contrasts with the findings in normal infants, where “against the rule” astigmatism seems to be the most common type (Table 5).
Astigmatism in infants: comparison between the present and previous studies
At the last examination, 57% of the whole longitudinal study group had a clinically significant astigmatism. This equals the high frequency of astigmatism in infancy and contrasts with the normal development, in which a decline in astigmatism is seen during the second year of life.30 ,35 Thus, the normal disappearance of astigmatism does not seem to take place in children with Down's syndrome.
Two thirds of the patients with clinically significant astigmatism at the last examination had stable axes during the whole follow up period. The 12 patients in whom an oblique astigmatism was recorded at least once in one or both eyes deserve particular attention. All the eight eyes changing axis belonged to this group. The axis of the oblique astigmatism in the right eyes was in all cases in the 135° meridian, while all the oblique astigmatism in the left eyes was in the 45° meridian. To our knowledge, this right-left specificity of oblique astigmatism in Down's syndrome has not previously been pointed out or commented on. The astigmatic axes are usually only reported as “with the rule,” “against the rule,” or oblique. We have only found one publication reporting the axes separately for the right and the left eyes in patients with Down's syndrome.1 In this report, 14 out of 15 eyes with oblique astigmatism showed the same right-left specific pattern as in our study.
We have had the opportunity to review the refractive data on 50 teenagers (100 eyes) with Down's syndrome reported by Doyleet al.36 Fifty two eyes had cylindrical power ⩾1.0 D. Among these, 21 had an oblique axis according to our definition. The direction of the axes showed the same right-left specificity as described above in 18 of these 21 eyes (86%). These data on the right-left specific axes were not reported in the published article.
In normal adults, McKendrick and Brennan37 found that the right and the left eyes with oblique astigmatism were equally distributed to the 135° and the 45° meridian. This finding corresponds to the results of our preoperative measurements on the excimer laser patients.
We suggest that this right left specific direction of oblique astigmatism may be caused by the upward slanting of the palpebral fissure, first described in the original publication by Down.38 Not specifically for Down's syndrome, but as a general hypothesis, pressure from the eyelids has already been pointed out as a major aetiological factor of corneal astigmatism.32 ,39 Shapiro and France5 found that the angle of the palpebral fissure in Down's syndrome patients exceeded 10° in 45% of the patients. In addition, Lowe1reported a widening of the angle between the two anteroposterior orbital axes from the normal 45º to 75° in four skulls from Down's syndrome patients. Both these factors might contribute to the right-left specificity in oblique astigmatism in Down's syndrome.
In conclusion, our longitudinal study confirms an abnormal refractive development in children with Down's syndrome. A possible causative association to a poor accommodation needs to be further explored. A high frequency of accommodation weakness in children with Down's syndrome suggests a more liberal use of bifocal or progressive glasses than practised today. At present, however, it must be emphasised that although improving visual performances at near, it is uncertain whether the use of progressive or bifocal glasses will prevent an unfavourable refractive development in children with Down's syndrome.
Acknowledgments
We are grateful to Dr Stephen J Doyle and co-workers at Manchester Royal Eye Hospital, who put their data on teenagers with Down's syndrome at our disposal. The Medical Birth Registry of Norway (MBR) and the Laboratory for Cytogenetics, Center for Medical Genetics and Molecular Medicine, Haukeland University Hospital, Bergen, are gratefully acknowledged for their efforts to provide necessary information. We thank Birgitte Espehaug for valuable help with the statistical analyses.