Article Text

Abstract
Kawasaki disease (KD) is a childhood vasculitis and the most frequent cause of paediatric acquired heart disease in North America, Europe and Japan. It is increasingly recognised in rapidly industrialising countries such as China and India where it may replace rheumatic heart disease as the most common cause of acquired heart disease in children. We review the current global epidemiology of KD and discuss some public health implications.
- Kawasaki disease
- Epidemiology
Statistics from Altmetric.com
Introduction
Kawasaki disease (KD) is an idiopathic systemic vasculitis particularly affecting infants and young children. The aetiology remains unknown and there is no diagnostic test. KD is characterised by the sequential appearance of clinical features, many of which are seen in other paediatric disorders, and none of which are specific or sensitive for KD. The diagnosis is usually made on a constellation of characteristic clinical findings, which may appear sequentially.1 KD is a serious and potentially life-threatening condition.2 It results in coronary artery aneurysms in up to a quarter of untreated patients. The risk of coronary artery aneurysm is reduced to ∼5% with prompt and appropriate treatment.1 KD is the most common cause of paediatric acquired heart disease in North America, Europe and Japan.1 The long-term cardiovascular risks associated with KD remain unclear, especially in those with no abnormalities on echocardiography.
KD has been reported from over 60 countries in all continents and is increasingly recognised in many resource-limited countries (figures 1 and 2).3 The fascinating epidemiology of KD has provided important clues to the aetiology. Here we describe the current global epidemiology of KD and discuss potential public health implications.
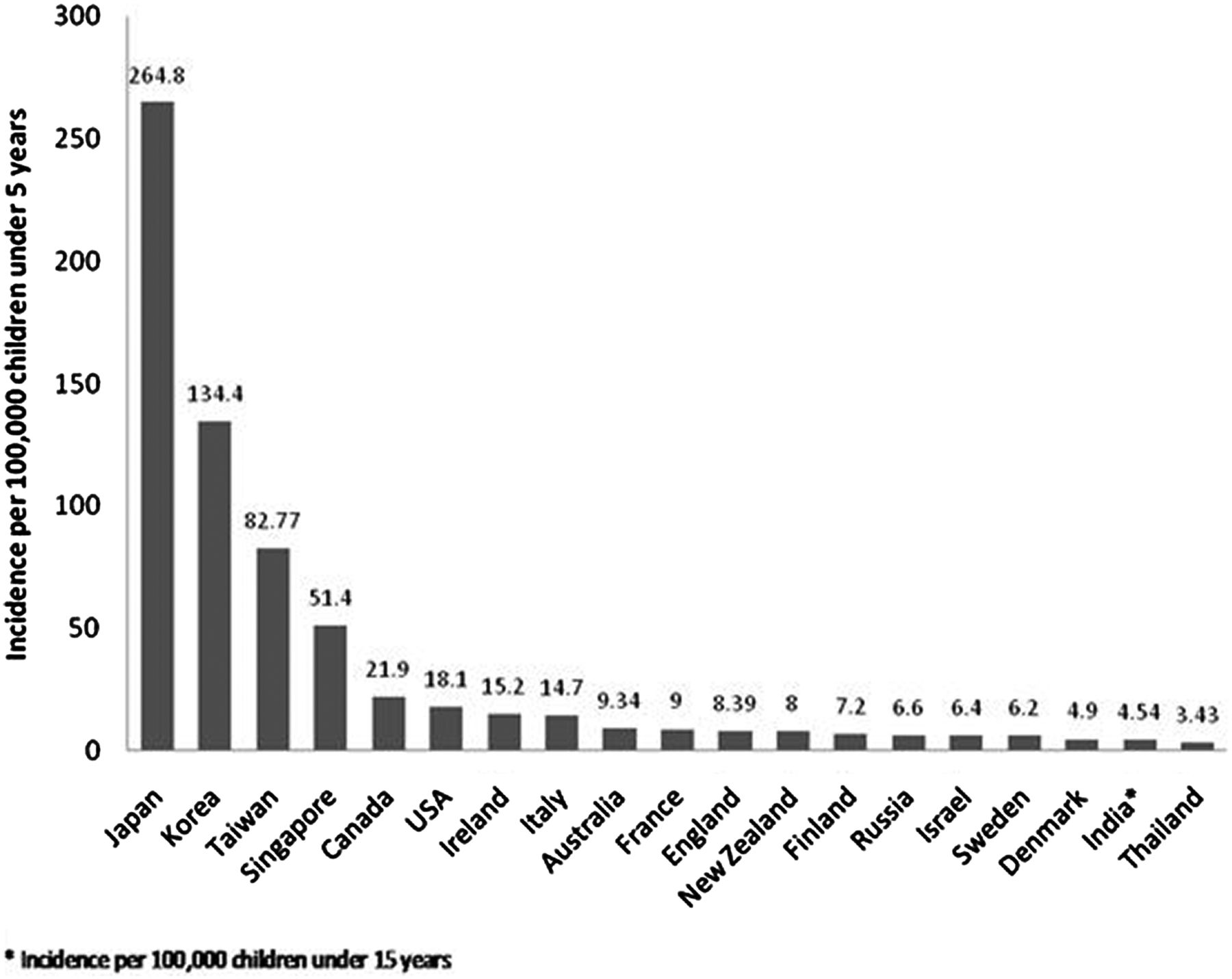
Histogram showing the incidence of Kawasaki disease per 100 000 children aged <5 years across the globe.

{kind=link}
{kind=link}
Incidence of Kawasaki disease from 2000 to 2012 per 100 000 children aged <5 years.
It is important to note that there are inherent limitations to the epidemiological data. The clinically based diagnosis and the proportion of incomplete cases mean that the true incidence remains unknown, with under-reporting and over-reporting likely. Epidemiological studies have used various methodologies, including passive surveillance from regional or national hospitalisation records, active surveillance of case-reporting clinicians, retrieval of intravenous immunoglobulin (Ig) prescriptions, and centre-based case registries, all of which may lead to variations in epidemiological data. Systematic medical chart review to identify missed cases or confirm administrative diagnoses is rarely performed.4
The criteria for the epidemiological diagnosis of KD are well described, although the more widely used American Heart Association (AHA) guidelines1 differ from those from the Japanese Ministry of Health.5 In contrast to the AHA guidelines, the Japanese criteria include fever as one of six diagnostic features, of which four must be present for the diagnosis to be made with certainty. In addition, fever of 4 days or less is considered diagnostic if early intravenous Ig is given, as almost a third of Japanese patients receive intravenous Ig on or before day 4 of fever.5 In clinical practice it is not unusual for treatment to be given even when the diagnostic criteria are incomplete and the KD diagnosis is not secure. Therefore hospital-based records based on KD diagnosis and/or treatment may yield different incidence estimates from active epidemiological surveys.6 Conversely, it is unfortunately not unusual for cases of KD to be missed and this may be more prevalent in countries where the condition is less familiar, leading to regional variation in under-reporting. Finally, almost all studies report the incidence of KD per 100 000 children less than 5 years of age. We have followed this convention in this review and the incidence data presented here relate to this age group unless otherwise stated. However a significant proportion of KD occurs in school-age children7 and the total disease burden is therefore greater than that implicit in using preschool children as the denominator for incidence rates.
Epidemiological patterns of KD
Distinct epidemiological patterns of KD have been described (figure 2). In North America, Australia and Europe, the current incidence of KD is 4–25/100 000 children under 5 years, with well described variations in different ethnic groups.7–9 In these regions the incidence increased—partly due to increased ascertainment—until the last decade, when it appears to have largely plateaued. In contrast, North-East Asian countries (notably Japan and Korea)10 ,11 and Taiwan12 report an incidence 10–20 times higher than the USA and Europe, and the incidence is continuing to increase. For example the current incidence in Japan is 265/100 000 <5 years, with approximately 14 000 KD diagnoses reported in 2012.10 In China and India—the two most populous countries—from where only more recent and less complete epidemiological data are available, the incidence also appears to be increasing, mirroring rapid industrialisation and economic growth.13 ,14 Even a modest increase in incidence of KD in these countries would have profound implications on the likely burden on health services caring for children acutely, and for adults with coronary artery sequelae.
Epidemiology in Europe, America, Australia and New Zealand
North America, Europe, Australia and New Zealand currently have a stable incidence, varying between a relatively low incidence in Scandinavia, moderate incidence in the UK and continental European countries (such as The Netherlands) and the highest incidence in regions of Canada and the USA. These latter observations may partly reflect referral patterns to specialist centres.7–9 ,15–17 There is some evidence that KD may have been present in the UK for over a century as pathological specimens indicate similar coronary artery pathologies.18
KD in the USA and Europe
Passive surveillance data from the USA are available from the mid-1970s. These data suggest a current incidence of between 17.5/100 000 and 20.8/100 000.9 There appears to have been no significant increase in the KD incidence in the USA in the last decade.8 The North American data show significant ethnic variation in KD incidence, with a significantly higher rate in Pacific Islanders and African Americans.8 ,9 In Japanese Americans living in Hawaii, the incidence is similar to that in Japan (>200/100 000),19 suggesting a significant genetic contribution to KD susceptibility. In Ontario, Canada, the incidence increased until the last published report in 2011 (27.5/100 000).17 There is increasing awareness of the burden of KD in Latin America, and regional epidemiological studies are underway.20
Most European countries report an incidence <16/100 000 and in some countries with longitudinal data, the incidence may have plateaued. Hospital episode statistics from 1998–2003 in England show seasonal peak for KD in winter months. The annual incidence was estimated to be 8.4/100 000. The report also noted a higher incidence of KD in children of Chinese ethnicity.21 In Australia and New Zealand, in which much of the recent population immigration in the last ∼150 years has been from northern Europe, the incidence rate (approximately 8–10/100 000) has increased in the last four decades and is now similar to the UK.7 ,16 It is unclear whether the incidence in Australia is continuing to increase or has levelled off.
KD in Japan, Korea and Taiwan
Japan, Korea and Taiwan are the only Asian countries with robust nationwide incidence data.6 ,10–12 ,22 In these countries the incidence is >50/100 000 (figures 1 and 2) and has continued to increase over the last few decades (figure 2). It has been suggested that KD may not have existed in these countries prior to the 1950s and may therefore be a ‘new’ disease.18
KD in Japan
Japanese data are principally based on nationwide epidemiological surveys conducted regularly since the early 1970s. Twenty-two surveys have been completed to date.10 Data are from questionnaires returned by specialist paediatric hospitals or general hospitals with >100 beds, so may represent an underestimate if smaller centres manage uncomplicated cases. The response rate was 43% in the first survey and 71.6% in the most recent.10 ,23 KD incidence has more than doubled since 1990 and continues to increase. The current incidence is the highest worldwide (265 per 100 000 <5 years) and an estimated 1 in 100 Japanese children will be diagnosed with KD by the age of 10 years.10 Japan has documented three large nationwide epidemics, in 1979, 1982 and 1986, the only country to do so.9 Large epidemics have not been reported recently, but Japan and many other countries report less dramatic spatial and temporal clustering.24
KD in Korea
Korea has conducted questionnaire-based nationwide surveys on KD from all hospitals with a paediatric residency programme every 3 years since 1991. The incidence has been increasing since 2000. Korea reports the second highest incidence of KD in the world (134.4/100 000).11
KD in Taiwan
Incidence data on KD in Taiwan are based on hospitalisation records maintained by the National Health Insurance System. The current incidence (82.8/100 000) is the third highest in the world.6
Patterns in other Asian countries
In China and India there is a paucity of accurate nationwide data on trends in KD incidence. Some data are available from cities or regions but nationwide studies are difficult to conduct in such populous countries.13 ,14 Moreover healthcare delivery is complex, with the private and public health systems managing patients with KD, and there is no centralised data linkage. Consequently epidemiological data are difficult to access and it is unclear whether the reported recent increases in KD incidence25 reflect nationwide epidemiology, or whether reported increases are sustained. These data will be important for modelling the likely impact of KD on health service utilisation, especially given the enormous populations potentially at risk.
KD in China
Data on the incidence of KD in China are based on studies conducted in different provinces using varying methodologies, making comparisons difficult.13 ,26 In Beijing, questionnaire data give an incidence between 40.9/100 000 and 55.1/100 000 between 2000 and 2004, with a significant increase observed from 1995 to 2004.13 ,27 In Shanghai the reported incidence increased from 27.3/100 000 between 1998 and 2002, to 46.3/100 000 in 2007.28 In Sichuan province, the mean incidence during 1997–2001 was 7.1/100 000 children, which may reflect relative social disadvantage and access to medical services.26 In Hong Kong the incidence of KD increased from 26/100 000 in 1994, to 39/100 000 in 2000, and to 74/100 000 in 2011.29 Despite different methodologies in China and Hong Kong, the overall trend is similar to that in East Asia overall, with an increasing incidence of KD during the last 10–20 years and no evidence of a levelling off.
KD in India
KD has been increasingly reported from several parts in India over the last 20 years. Prior to 1990, there were only three published reports of KD.30 This was followed by two case series in 1997 from two geographically non-contiguous areas in the country—Trivandrum (South India) and Chandigarh (North India).30 Subsequently KD has been identified in virtually all parts of the country. Based on a hospital based analysis from 1994 to 2007 in Chandigarh, the incidence has increased from 0.51 in 1994 to 4.54 cases per 100 000 children below 15 years of age in 2007, although annual incidence varied.14 This figure is likely to be an underestimate.
Seasonality of KD
Asian countries
Several countries have reported distinct seasonality in KD. Japan reports two seasonal peaks of KD incidence in January and July, with a nadir in October.9 ,10 ,24 Korea, at approximately similar latitude, has similar peaks in June/July and December/January.31 Taiwan has peaks in May/June and the lowest incidence is reported from November to January.12 Seasonality data from China are more variable.9 In Chandigarh (India), a consistent peak in October with a nadir in February is observed.14
USA and Europe
KD has been reported to occur more commonly in the winter months in mainland USA, Canada and Europe, and in the more temperate regions of Australia.7 ,9 Winter peaks in incidence are not discernible in Hawaii, where the seasonal weather patterns are different from mainland USA.9 ,19 A recent global study of the seasonality of KD described a winter peak and summer/autumn nadir in non-tropical regions of the northern hemisphere, but less clear seasonality (partly related to less data) in the southern hemisphere.32
A putative hypothesis to explain the seasonality of KD
Fascinating recent observations show that seasonal changes in tropospheric wind patterns from the northern Pacific closely correlate with KD cases in Hawaii, southern California and Japan.33 Similar associations with wind patterns have not been observed in Canada34 and analogous data are not available from several other parts of the world including Europe, although an association with northern desert winds has been reported from Chile.35 It has been hypothesised that KD may be triggered by an airborne agent originating in central Asia. It is suggested that this putative trigger is blown to various geographical regions of the world in the troposphere and by entering the upper respiratory tract results in KD. Air-sampling of the troposphere has shown a high density of spores from Candida albicans,36 although whether this is necessary or sufficient to cause KD is unclear. Interestingly a C. albicans cell wall extract is used as a stimulus in some animal models of KD. Further studies, including data relating incidence to wind patterns from other regions of the world, are needed to confirm the relevance of these interesting observations to the aetiology of KD.
KD epidemiology—a true increase in incidence or increased ascertainment?
KD is currently diagnosed and reported frequently in several populations, including those in rapidly industrialising countries such as India and China. It is difficult to determine whether this is the result of increased ascertainment due to increased awareness and/or access to specialist medical services, or whether it reflects a true increase in incidence. It seems likely that both factors play a role in many countries, at least those where KD has been described more recently.
In countries where the diagnosis has been familiar for many years, the incidence continued to increase initially and then plateaued (eg, USA, Canada, UK).9 ,17 ,19 In contrast in Japan and other North-East Asian countries, where the disease is common and well recognised, the incidence continues to increase, presumably indicative of a true rise in diagnosed cases.10
A correlation has been noted between economic development and the emergence of KD in several countries in Asia. Industrialisation has been accompanied by the adoption of a more ‘Western’ diet and lifestyle. This may have resulted in a new niche for the trigger(s) that previously did not result in overt disease. For instance, the emergence of KD in Japan parallels the rapid economic development from the mid-1950s to the early 1970s. Similar associations have been noted in Korea, Taiwan and China.18 In a national UK epidemiological study, urbanisation was significantly associated with KD incidence, although it was unclear whether this partly reflected a greater proportion of Asians living in larger towns and cities.21 Analysis of the Taiwanese National Health Insurance database showed no association between urbanisation and KD incidence.22
There are limited regional data from single countries. In China, the KD incidence is much lower in the Jilin province than in Shanghai and Beijing,12 ,13 ,28 ,37 and there is also marked economic disparity between these provinces. In India, economic liberalisation and high growth have been evident since the early 1990s, although in the absence of national epidemiological data, it remains largely speculative whether there is a relationship between KD incidence and economic growth in India.
Anecdotal reports, confirmed by a single-centre prospective study,38 suggest a predominance of KD cases from more affluent Indian families. In Kerala, South India, which has one of the highest rates of literacy and economic development in India, KD incidence appears to be increasing rapidly.25 It is unclear whether these regional variations reflect differences in economic growth, industrialisation and/or access to services.
Why is the epidemiology of KD important?
Public health implications
For the first half of the 20th century, rheumatic fever was the most common cause of acquired heart disease in children worldwide. With the control of rheumatic fever in industrialised countries, rheumatic heart disease became relatively rare in these settings by the 1980s, except for occasional outbreaks,39 and showed very high rates in certain populations, such as Australian Aborigines and New Zealand Ma¯ori.40 By the mid-1980s, the long-term consequences of KD were recognised in Japan and North America and it was apparent that KD had replaced rheumatic fever as the most common cause of acquired heart disease in children in industrialised countries, especially Japan and the USA, which had reliable epidemiological data. By late 1990s KD was increasingly recognised in China and India, while rheumatic fever appeared to be in decline. In Chandigarh (Northern India) for example, approximately 10 times more children are diagnosed with KD than with acute rheumatic fever annually, although formal prospective epidemiological data are not available. Anecdotally paediatricians across India are reporting similar trends.41 As many children with KD are still not being diagnosed and treated, it is possible that KD may emerge as the most common cause of paediatric acquired heart disease in India, as in other industrialised settings.14 ,30 ,42
KD should no longer be considered to be a disease only of more affluent populations; it has public health implications for all countries. The consequences of unrecognised—and hence untreated—KD in childhood may manifest several decades later, with potential implications for the burden of adult heart disease.42 This will have economic implications for developing countries because coronary artery disease post-KD may affect individuals at the peak of their economic productivity. Therefore the consequences of KD are likely to pose significant challenges to the healthcare system, especially in populous countries such as China and India due to the high costs of treatment in the acute stage, and the potential for lifelong sequelae.
Recent modelling suggests that by 2030, 1 in 700 individuals in Taiwan and 1 in 1600 individuals in the USA will have a history of KD in childhood.43 Similar projections, which necessitate accurate national epidemiology, are needed for countries such as India and China, which have a large and probably underappreciated KD burden. These data will help inform policy and planning of healthcare resources.
In summary, KD is now a well recognised and common cause of paediatric acquired heart disease globally. In resource-poor settings it is likely that many children remain untreated and, coupled with a high and increasing incidence in many Asian countries, this will mean that the adult coronary artery disease burden from KD is likely to be significant and will increase.
Acknowledgments
The authors thank Nigel Curtis for helpful comments on an earlier version of the manuscript.
References
Footnotes
Contributors SS reviewed and analysed the literature and wrote the initial draft. PV provided inputs with regards to recent epidemiological figures from various countries and helped collate and analyse data with regards to the two figures. DB edited and critically reviewed the manuscript and incorporated several additional data, especially with regards to studies from the UK, Australia and New Zealand. All the authors have been actively involved in editing, approving and finalising the submitted version of the manuscript.
Competing interests None declared.
Provenance and peer review Commissioned; externally peer reviewed.