Article Text

Abstract
Delayed puberty (DP) is defined as the lack of pubertal development by an age that is 2–2.5 SDs beyond the population mean. Although it generally represents a normal variant in pubertal timing, concern that DP could be the initial presentation of a serious underlying disorder has led to a diagnostic approach that is variable and may include tests that are unnecessary and costly. In this review, we examine available literature regarding the recommended diagnostic tests and aetiologies identified during the evaluation of youth with DP. We view this literature through the prism of the seemingly otherwise well adolescent. To provide further clinical context, we also evaluate the clinical and laboratory data from patients seen with DP in our centre over a 2-year period. The literature and our data reveal wide variability in the number of tests performed and raise the question of whether tests, other than gonadotropins, obtained in the absence of signs or symptoms of an underlying disorder are routinely warranted. Together this information provides a pragmatic rationale for revisiting recommendations calling for broad testing during the initial diagnostic evaluation of an otherwise healthy adolescent with DP. We highlight the need for further research comparing the utility of broader screening with a more streamlined approach, such as limiting initial testing to gonadotropins and a bone age, which, while not diagnostic, is often useful for height prediction, followed by close clinical monitoring. If future research supports a more streamlined approach to DP, then much unnecessary testing could be eliminated.
- DELAYED PUBERTY
- ETIOLOGY
- INVESTIGATIONS
- CHOOSING WISELY
Statistics from Altmetric.com
INTRODUCTION
Delayed puberty (DP) affects approximately 2% of adolescents.1–3 Patients with DP are cared for by family physicians, general paediatricians and paediatric subspecialists. DP can be a source of significant anxiety for patients and their parents. Although it generally represents a normal variant in pubertal timing, it can also be the initial presentation of a serious underlying disorder. Despite the clinical importance of DP, the initial diagnostic approach to this condition is variable and may include tests that are unnecessary and costly. This article will review the current recommendations regarding the initial work-up of DP in the seemingly otherwise well adolescent and will provide a rationale for revisiting those recommendations.
What is delayed puberty?
DP is defined as the lack of the initial signs of puberty (Tanner stage 2 breast development in girls or testicular enlargement to ≥4 mL in boys) at an age that is 2–2.5 SDs beyond the population mean.1–3 The presence or absence of pubic hair is not part of this definition because it can be due to androgen production from the adrenal gland (adrenarche) instead of the gonad. Traditionally, the age cut-offs for DP are a chronological age of 13 years in girls and 14 years in boys.1–5
Differential diagnosis
The differential diagnosis of DP is wide (table 1). The most common aetiology is constitutional delay of growth and puberty (CDGP), a non-pathological state in which the maturation of the hypothalamic-pituitary-gonadal (HPG) axis is delayed and puberty begins at an age at the extreme end of the normal spectrum.4 ,9 CDGP is a diagnosis of exclusion, and alternative causes of DP need to be considered.4 ,10 ,11 These causes can be divided into three main categories: (1) hypergonadotropic hypogonadism, which is characterised by elevated levels of follicle-stimulating hormone (FSH) and luteinising hormone (LH) and is due to gonadal failure or the inability to synthesise or respond to sex steroids; (2) permanent hypogonadotropic hypogonadism, which is characterised by low levels of FSH and LH and can be caused by an underlying central nervous system (CNS) abnormality, can be associated with other neuroendocrine deficiencies or be isolated/idiopathic; and (3) functional hypogonadotropic hypogonadism (FHH), which is also characterised by low levels of FSH and LH but which represents a transient delay in HPG axis maturation due to an associated condition, such as coeliac disease, inflammatory bowel disease or anorexia nervosa.
Common causes of delayed puberty
Few studies have attempted to evaluate the relative frequencies of the various causes of DP.4 ,9 ,12 ,13 In one large retrospective cohort study from an academic centre, the most common diagnosis was CDGP, in both boys (63%) and girls (30%), followed by FHH (20% of boys and 19% of girls), hypergonadotropic hypogonadism (7% of boys and 26% of girls) and permanent hypogonadotropic hypogonadism (9% of boys and 20% of girls).4 A more recent study evaluated 451 Danish boys with DP and found that 64% had CDGP, 18% had FHH, 2.9% had permanent hypogonadotropic hypogonadism and 0.4% had hypergonadotropic hypogonadism.9
History and physical examination
Given the extensive differential diagnosis of DP, all patients should undergo a complete history and physical examination. This evaluation should focus on red flags that could help identify an underlying aetiology (table 2). A thorough family history, including childhood growth patterns and age at pubertal onset of parents and siblings, should be obtained since a family history of DP is found in 50–75% of patients with CDGP.10 ,14
Red flags on history and associated aetiologies
A complete physical examination, including height, weight and growth velocity, may also provide clues about the cause of the DP (table 3). In addition, careful determination of sexual maturity by Tanner staging1 ,2 and measuring testicular volume is key to confirming the diagnosis and can help identify early signs of sexual development that may go unnoticed by patients and/or parents.
Physical examination findings and associated aetiologies
Initial screening tests
The goal of a thorough history and physical examination is to allow physicians to focus their investigations and avoid unnecessary diagnostic tests. In many patients, however, the history and physical examination will be unremarkable and which screening tests to order is unclear. Nearly all published algorithms5 ,7 ,15 call for measurement of LH and FSH to separate hypergonadotropic hypogonadism from the other causes of DP. However, the list of other initial diagnostic tests recommended in the literature is broad, variable and based largely on expert opinion. The suggested initial evaluation could include full blood count, erythrocyte sedimentation rate, electrolytes, liver function tests, urea, creatinine, oestradiol, testosterone, insulin-like growth factor 1 (IGF-1), thyroid function tests, prolactin, bone age, karyotype and MRI of the brain.5 ,7 ,15 The differentiation between CDGP and congenital (idiopathic) hypogonadotropic hypogonadism (CHH) remains difficult. Tests that have been proposed to distinguish the two include inhibin B, antimullerian hormone, basal gonadotropin (LH and FSH) levels, gonadotropin-releasing hormone (GnRH) stimulation or GnRH-agonist stimulation tests and human chorionic gonadotropin stimulation tests.8 ,11 ,16
The utility of specialised, second-line tests in distinguishing CDGP from CHH and of MRI to diagnose CNS abnormalities has been addressed in previous papers and is outside the scope of this review.8 ,11 ,16 Here we seek to discuss the utility of the first-line screening tests recommended to differentiate CDGP from FHH.
Are all the FHH screening tests warranted in each patient?
After identifying the patients who have hypergonadotropic hypogonadism, an important goal is to identify patients with FHH, the cause of DP in up to 19% of cases.4 ,9 Identifying and treating the cause of the FHH will lead to initiation of puberty and improve the overall health of the patient. However, each of the individual conditions within this diagnostic category is a relatively rare cause of DP. For example, out of the 232 subjects with DP in one study only 6 (2.6%) had growth hormone deficiency (GHD), 3 (1.3%) had hypothyroidism and 1 (0.4%) had coeliac disease.4 A 2015 study found similar results with 14 (3.1%) of 451 patients being diagnosed with GHD, 9 (2%) with hypothyroidism, 1 (0.2%) with hyperthyroidism, 1 (0.2%) with hyperprolactinemia and none with coeliac disease.9 Neither of these studies reported whether or not patients with these underlying diagnoses had suggestive findings on history or physical examination. If such findings were present, then these data would argue even more strongly against large panels of screening tests in otherwise well-appearing adolescents. Overall, the rarity of each of the underlying diagnoses raises the question of whether routinely obtaining all the recommended diagnostic tests is warranted.
In preparation for writing this article, we performed a local quality improvement project and examined which tests are included in the initial evaluation of DP in our clinic and how frequently each of the tests led to a diagnosis or affected the patient's management. A chart review of all patients with DP seen in the Division of Endocrinology at the Hospital for Sick Children between August 2012 and July 2014 was performed. Sixty-four patients underwent their initial evaluation for DP during this time. Similar to previous studies,4 ,9 the most common diagnosis among our patients was CDGP. Among the patients who were previously healthy, 70% had CDGP, 18% had FHH, 7% had permanent hypogonadotropic hypogonadism and 4% had hypergonadotropic hypogonadism. Among the patients with a previously diagnosed chronic disease, most (85%) had FHH (eg, inflammatory bowel disease) with the remaining patients having hypergonadotropic hypogonadism (eg Fraser syndrome). Seventeen patients had a previously diagnosed endocrinopathy known to cause DP (ie, panhypopituitarism) and were excluded from our analysis.
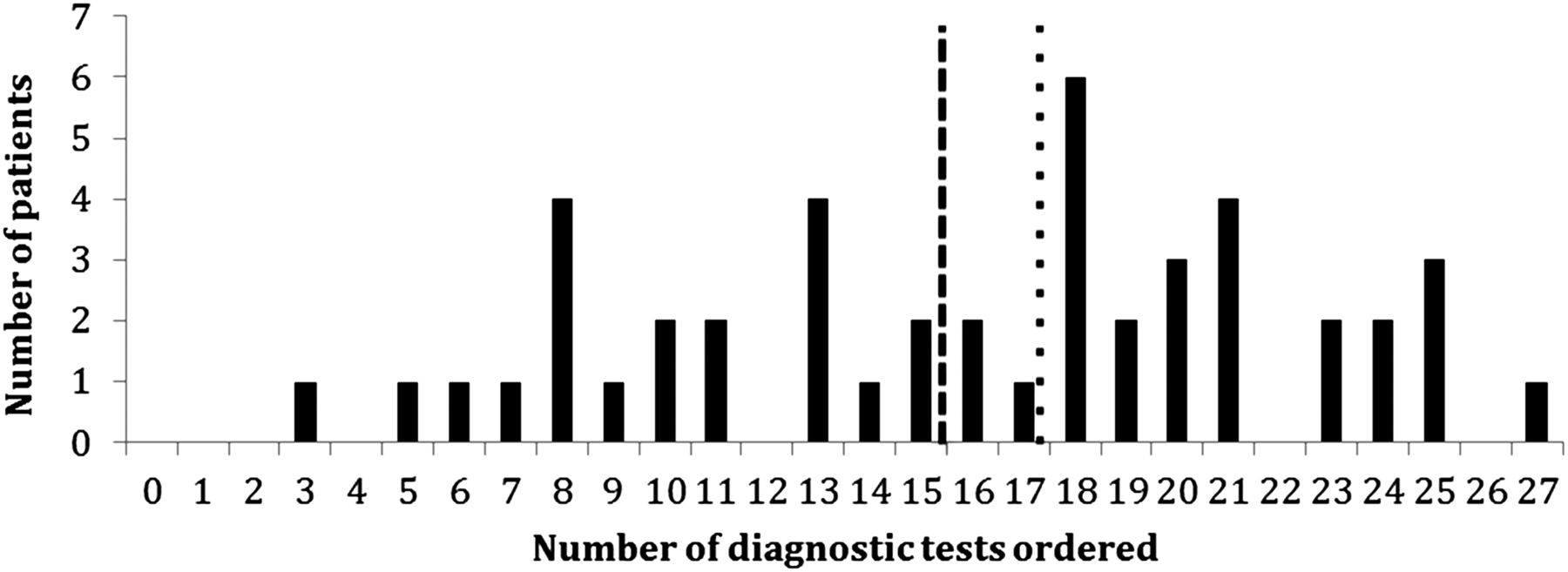
Wide inter-practitioner variability in the number of diagnostic tests ordered, ranging from 3 to 27, was observed. The mean number of diagnostic tests ordered at the patient's initial visit was 16 with a median of 17 (figure 1). Table 4 shows the subset of tests that were most frequently ordered and how often they led to a diagnosis in our patients.
Frequency that the most common diagnostic tests were ordered and the percentage of abnormal results that led to a diagnosis

Number of individual diagnostic tests ordered during the initial evaluation of patients with delayed puberty. An individual diagnostic test was defined as any investigation that can be ordered separately. Dashed line=mean; dotted line=median.
LH and FSH were helpful in diagnosing the patients with hypergonadotropic hypogonadism. Conversely, diagnostic tests ordered to identify FHH in the seemingly well child, including thyroid function testing, coeliac screen and tests of systemic illness (full blood count, liver function testing, electrolytes and renal function), were not helpful. None of our patients were diagnosed with a thyroid abnormality or coeliac disease during their evaluation for DP. In addition, all patients diagnosed with FHH had suggestive findings on history or physical exam. For example, the two patients with GHD diagnosed by stimulation testing had poor growth velocity; the patient with anorexia nervosa had a history of food restriction and low weight for height; and the patient diagnosed with inflammatory bowel disease (IBD) had a history of weight loss and haematochezia.
Our review of the literature as well as our recent clinic experience raises important questions about the utility and cost effectiveness of the screening tests routinely performed to identify FHH in the otherwise seemingly well adolescent. It is important to note that the list of potential initial evaluations recommended in the existing literature5 ,7 ,15 includes tests that assess for aetiologies other than FHH and many of these also do not seem warranted as first-line investigations. For example, a karyotype would assess for causes of gonadal failure (Turner syndrome or Klinefelter syndrome) and is likely not needed unless there is clinical suspicion or elevated gonadotropin levels. An MRI would assess for causes of permanent hypogonadotropic hypogonadism; however, without findings suggestive of a CNS lesion, this can likely be postponed until a young man is 14.5–15 years old or a young woman is 13.5–14 years old to allow 6–12 months of observation for spontaneous entry into puberty.5
Should the current approach to DP be changed?
The majority of children with DP have CDGP. It is likely that the true prevalence of CDGP is even higher than reported in the literature since the studies were all performed at tertiary care centres and patients with CDGP are often cared for by primary care physicians and community paediatricians. FHH is the second most likely aetiology; however, there are a wide number of diagnoses that can lead to FHH and each is individually rare. Therefore, broad, routine testing for aetiologies of FHH during the initial evaluation of an otherwise seemingly well adolescent with DP is probably low yield. Based on the available evidence, we hypothesise that fewer routine investigations could be performed than previously recommended; however, additional research is needed prior to making specific recommendations.
Much unnecessary testing could be eliminated if future research corroborates our analysis. For example, a streamlined approach (figure 2) might involve a thorough history and physical examination to assess for findings that point to a particular diagnosis. A bone age, while not a diagnostic test, could be obtained since it allows for height prediction and counselling of patients and their families. First-line laboratory investigations could include only serum gonadotropins to assess for hypergonadotropic hypogonadism. If serum gonadotropins are low, other testing would be based on pertinent positives on the history or physical exam. For example, thyroid function testing could be ordered in a patient with symptoms of hypothyroidism such as an increased weight to height ratio, cold intolerance, fatigue or a goitre. If there is not a suggestive history or physical examination, the patient could be followed clinically with further investigations done if there is a lack of spontaneous endogenous puberty after a 6–12-month observation period. Additional investigations could also be considered if there is a change in the history or physical examination or if the clinical course is not as expected, such as if a young man being treated with a course of testosterone does not show signs of height acceleration since this could be suggestive of a form of FHH (eg, secondary to coeliac disease). Our recommended algorithm could be altered in the future if tests that reliably distinguish CDGP from isolated congenital hypogonadotropic hypogonadism are identified.

{kind=link}
{kind=link}
Possible algorithm for the initial evaluation of a patient with delayed puberty. CDGP, constitutional delay of growth and puberty; CHH, congenital hypogonadotropic hypogonadism; FHH, functional hypogonadotropic hypogonadism; FSH, follicle-stimulating hormone; IGF-1, insulin-like growth factor-1; LH, luteinising hormone; PHH, permanent hypogonadotropic hypogonadism.
An assessment for GHD by measurement of IGF-1 as a first-line investigation should be reserved for the child with a reduction in growth velocity. While patients with CDGP can show a reduced growth velocity, it is not as severe as those with GHD. Further investigations for GHD should only be done if (1) the patient's height is <2 SDs below the mean and their growth velocity is 1 SD below the mean for at least 1 year or (2) the patient is of normal stature but their growth velocity is either 2 SD below the mean for 1 year or 1.5 SD below the mean for 2 years.17 While IGF-1 is a commonly used screening test for GHD, low levels should be interpreted in the context of a patient's bone age and pubertal status. Patients with CDGP may have reduced growth hormone secretion for age due to their DP, thus it is important to recognise that routine testing for GHD may yield false positive results.5 ,18 GH secretion is low in early puberty, increases as puberty progresses19 ,20 and sex steroids are important for GH secretion.21 ,22 For patients with an abnormal growth velocity and low IGF-1, a growth hormone stimulation test with sex steroid priming should be done to confirm GHD.
Limitations and future research
Although our review of available data argues against routine coeliac screening in patients with DP, we recognise the available literature is sparse and a definitive recommendation cannot be made. There are reports of coeliac disease being diagnosed during the evaluation of DP, but it is not known whether the prevalence of coeliac disease in otherwise asymptomatic children with DP is greater than the general population rate of 0.7–0.9%.23–28 Considering this the other way around, one study found the rate of DP among a cohort of newly diagnosed children with coeliac disease to be only 0.4%.29 This finding argues against the possibility that the low rates of coeliac disease observed in studies of DP stem from many individuals having been diagnosed with coeliac disease by primary care providers and referred to paediatric gastroenterologists instead of paediatric endocrinologists. Certainly coeliac disease can be missed because patients often present without gastrointestinal manifestations;30 however, in the absence of other features such as low weight for height, bowel symptoms or a positive family history, the available data suggest that the likelihood of coeliac disease as the aetiology of DP is low.4 ,9 On the other hand, a recent study reporting an increased association of coeliac disease (OR of 1.6) with delayed menarche among a large population of adults31 raises caution about this line of reasoning.
It is also important to note that the two large studies reporting the aetiologies of DP were not designed to determine the utility of diagnostic testing.4 ,9 Prospective data regarding how often coeliac disease and other conditions are diagnosed during the evaluation of otherwise asymptomatic youth are needed to resolve definitively questions about the utility of routine screening.
Conclusions
DP is encountered by many physicians who care for adolescents. Despite it being a common clinical condition, the diagnostic approach to DP remains highly variable and is often extensive. Available evidence raises the question of whether only limited investigations are warranted during the initial assessment of an otherwise seemingly well adolescent with DP. We recognise that our proposal to limit the initial testing done for DP may be controversial; however, we hope this article and the current focus on diminishing unnecessary testing, such as the Choosing Wisely Initiative,32 will prompt further research that compares the utility of broader screening with a more streamlined approach.
Acknowledgments
The authors thank Dr Jennifer Harrington for providing critical review and helpful comments prior to manuscript submission.
References
Footnotes
Contributors LA and SZ contributed equally. LA and SZ were involved in data collection and analysis and wrote the first draft of the manuscript. LA, SZ and MRP contributed to the critical review of the literature, editing and revising of the manuscript and approved the final version submitted for publication.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.