Article Text

Abstract
Background The National Confidential Enquiry describes the epidemiology of children admitted to hospital with head injury.
Method Children (<15 years old) who died or were admitted for >4 h with head injury were identified from 216 UK hospitals (1 September 2009 to 28 February 2010). Data were collected using standard proformas and entered on to a database. A descriptive analysis of the causal mechanisms, child demographics, neurological impairment, CT findings, and outcome at 72 h are provided.
Results Details of 5700 children, median age 4 years (range 0–14.9 years), were analysed; 1093 (19.2%) were <1 year old, 3500 (61.4%) were boys. There was a significant association of head injury with social deprivation 39.7/100 000 (95% CI 37.0 to 42.6) in the least deprived first quintile vs. 55.1 (95% CI 52.1 to 58.2) in the most deprived fifth quintile (p<0.01). Twenty-four children died (0.4%). Most children were admitted for one night or less; 4522 (79%) had a Glasgow Coma Scale score of 15 or were Alert (on AVPU (Alert, Voice, Pain, Unresponsive)). The most common causes of head injury were falls (3537 (62.1%); children <5 years), sports-related incidents (783 (13.7%); median age 12.4 years), or motor vehicle accidents (MVAs) (401 (7.1%); primary-school-aged children). CT scans were performed in 1734 (30.4%) children; 536 (30.9%) were abnormal (skull fracture and/or intracranial injury or abnormality): 269 (7.6%) were falls, 82 (10.5%) sports related and 100 (25%). A total of 357 (6.2%) children were referred to social care because of child protection concerns (median age 9 months (range 0–14.9 years)).
Conclusions The data described highlight priorities for targeted age-specific head injury prevention and have the potential to provide a baseline to evaluate the effects of regional trauma networks (2012) and National Institute of Health and Care Excellence (NICE) head injury guidelines (2014), which were revised after the study was completed.
- Accident & Emergency
- Injury Prevention
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
What is already known on this topic
Childhood head injuries are a common cause of hospital admission.
There are no national epidemiological studies of the causes and demographics of hospital admissions for children with head injury.
What this study adds
The peak prevalence of hospital admissions for childhood head injury is in infants, who carry the greatest risk of abnormality on CT scan.
There is a need for targeted age-specific prevention initiatives.
Baseline data are provided for future evaluation of the effects of the regional trauma network established 2012 and the National Institute of Health and Care Excellence (NICE) head injury guidelines (2014).
Introduction
Children present to hospital everyday with head injuries. However, the incidence is difficult to estimate and varies according to the definitions used and the point in the care pathway that children are ascertained. In 2012–2013, 34 932 hospital episodes were recorded for children with a head injury (International Classification of Diseases, 10th Edition (ICD-10) S00–09) in England1 representing an estimated annual incidence of 400 per 100 000 children younger than 15. Although the majority of childhood head injuries are minor, an estimated 5% have intracranial complications1 and associated morbidity and mortality,2 with long-term disability and intellectual, personality and behavioural problems.3 ,4 It is increasingly recognised that children with mild head injuries may have persisting cognitive and behavioural consequences from post-concussion or post-traumatic stress disorders.5
There are surprisingly few recent studies of childhood hospital admissions for head injuries. Publications describe the epidemiology of admissions to intensive care units with traumatic brain injury6 or minor head injuries5 ,7 or are regional.8–10 The Confidential Enquiry into Head Injury in Childhood was the principal project within the Centre for Maternal and Child Enquires (CMACE) in 2009–2012 and provided the opportunity to describe the characteristics of childhood head injury in children younger than 15 years old from a representative national dataset.
Methods
Data collection
The Confidential Enquiry collected data prospectively from 1 September 2009 to 28 February 2010. Data were extracted from case notes of children (<15 years old) who were admitted to hospitals across England, Wales, Northern Ireland and the Channel Islands or who died as a result of a head injury. While it is recognised that this time period might under-represent the peak of head injuries seen in the summer months, 6 months fitted with the resources timescale and capacity of the research team and was deemed reasonable for sustaining hospital participation. A total of 245 hospitals were approached; 230 agreed to participate (see online supplementary file 1) and a local head injury enquiry coordinator was appointed in each hospital. The characteristics of the participating hospitals are described elsewhere.11 Admission was defined as the child being treated or observed as an inpatient for more than 4 h. Children with superficial or facial injuries were excluded.
Supplemental material
From a review of the literature and clinical guidelines, data collection forms were designed to follow the child's pathway of care. Two questionnaires (see online supplementary files 2 and 3) documented the incident, child demographics, prehospital and hospital care, investigations, details of hospital transfers, and outcome at 72 h after admission. The coordinator in each hospital collected the data and returned it to CMACE on a monthly basis facilitated by email and telephone prompts and support. Completed forms were scanned and data entered on to a secure database.
Supplemental material
Supplemental material
CMACE government funding ended in 2011. A review was held to determine the future of the dataset, and it was decided that a further organisation should continue the analysis. The data were transferred to Cardiff University in July 2012. CMACE had Section 251 approval to obtain patient-identifiable information without consent. The project was approved by the Central Manchester Research Ethics Committee (Ref 09/H1008/74) and registered with hospital R&D or clinical governance departments in the participating hospitals. Approvals were renewed when the project was transferred to Cardiff University for analysis (Ref 09/H1008/74).
The Glasgow Coma Scale (GCS) scores12 were assessed on admission to the emergency department and used as indicators of the severity of neurological impairment. In a proportion of cases without a GCS score, the AVPU (Alert, Voice, Pain, Unresponsive)13 ,14 score was recorded. For the purpose of analysis when the GCS score was missing, AVPU scores were used. Four categories were created based on an equivalence study by Mackay et al;15 ‘GCS=15/Alert,’ ‘GCS=13–14,’ ‘GCS=9–12/responsive to voice,’ and ‘GCS≤8/response to pain or unresponsive’. A CT scan was deemed abnormal if stated as such in the clinical notes and included intracranial abnormality (within the brain or extra-axial structures) or skull fracture.
The postcode of the child's residence in England was mapped into the lower super output area (LSOA). Index of Multiple Deprivation (IMD) scores were calculated for all LSOAs and grouped into five quintiles based on these scores. The quintile of deprivation was taken as an ecological measure of deprivation for a child (5th quintile representing the greatest level of deprivation). The number of cases per million of the child population in each quintile was calculated and expressed as risk ratios/100 000 population for each quintile.
Data analysis
Data were compared with Hospital Episode Statistics (HES) data ICD-10 (S01–S09)16–18 for age and nation of origin to determine whether the dataset was representative of all children admitted to hospital with head injury for the year 2009–2010. Data from the two questionnaires were merged and imported by IBM SPSS V. 2019 statistical software. The statistical package was used to create tables and cross-tabulations, fit binary logistic regression models, and perform χ2 tests of categorical data. The Kolmogorov–Smirnov test was used for data that were not normally distributed, and z scores were used to determine the difference between risk ratios/100 000 population. For all statistical tests, p<0.05 used to denote significance.
Results
Data were collected on 6270 children from 216/ 230 (94%) of the participating hospitals; 570 children were excluded (outside the age range (63), admitted for reasons unrelated to head injury (173), not admitted to hospital (44), or data forms were not returned (290)), leaving 5700 children for analysis.
Overall, 5131 (90%) of the children attended a hospital in England, 177 (3%) in Northern Ireland, and 392 (7%) in Wales. Overall, 4768 (83.7%) were admitted to a general hospital, and the remainder to hospitals with neurosurgical or specialist children's units. Infants younger than a year accounted for 1093 (19%), 2042 (35%) were aged 1–4 years, 1100 (19%) were aged 5–9 years, and 1447 (25%) were aged 10–14 years (age was missing for eight cases). The regional and age distribution of this dataset matched those reported in hospital admission data 2009–2010.16–18 Thus the dataset was deemed representative of children admitted with head injury to hospitals in England, Wales and Northern Ireland.
The admission rate in September was higher than in any other month in the study (figure 1). More than half of the children, 2929 (51.4%), arrived at the hospital between 13:00 and 19:00 (figure 2). Neither the number nor the time of admission varied significantly for different days of the week.

Month of admission for 5700 children with head injury.

Time of arrival in emergency department in the first hospital.
Sociodemography
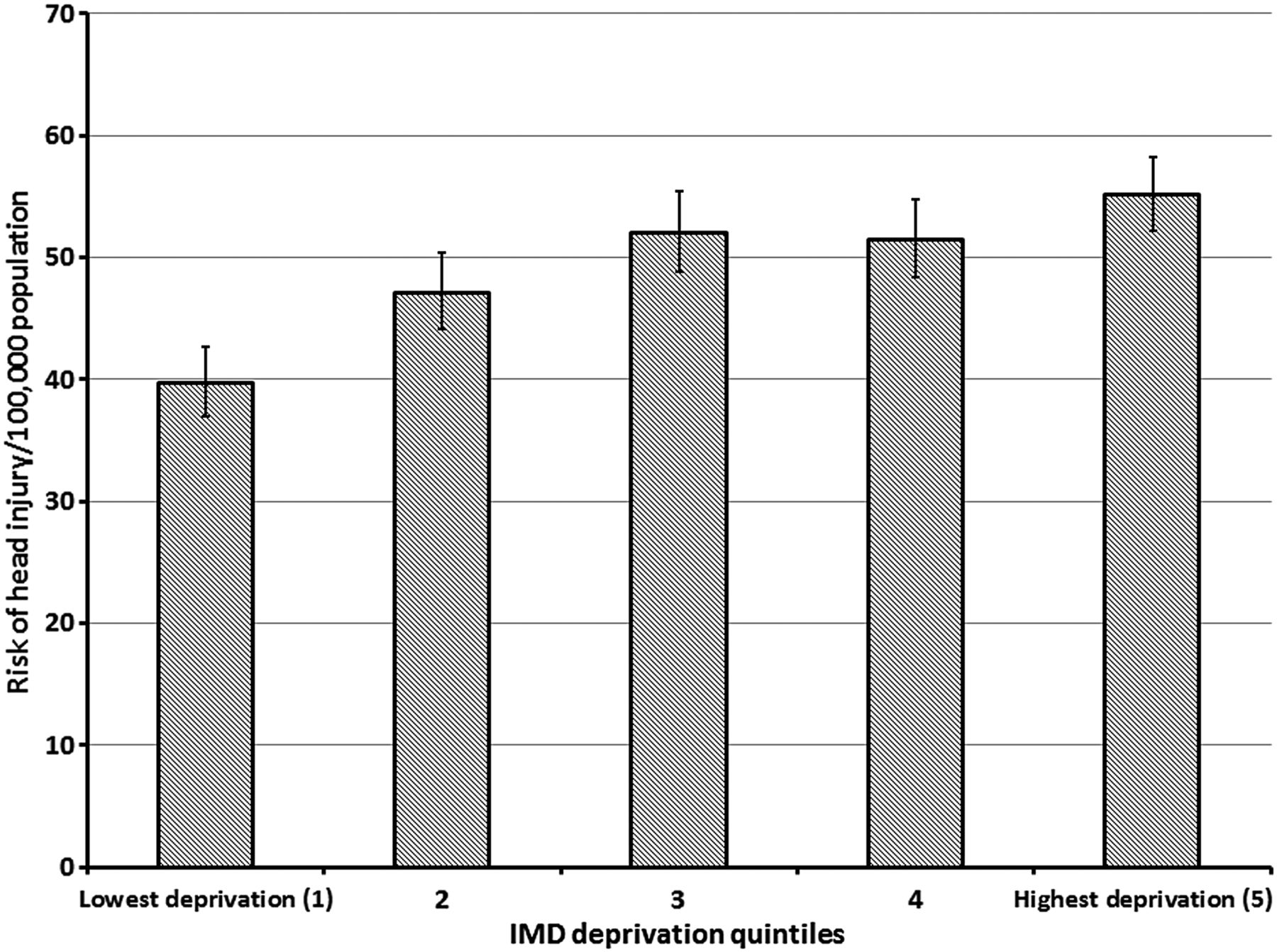
More than half, 3135 (55%), were younger than 5 years old, with peak prevalence in infants; 3500 (61.4%) were male, and the male to female ratio increased with age (figure 3). The IMD scores were available for 4882/5131 (95.1%) of the cases from England. The risk of head injury/100 000 population increased with social deprivation from 39.7/100 000 (95% CI 37.0 to 42.6) in the least deprived first quintile to 55.1 (95% CI 52.1 to 58.2) in the most deprived fifth quintile (p<0.01) (figure 4).

Age distribution in years and gender of children with head injuries. ▪ Female; ▪ Male.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Risk of head injury/100 000 of children with 95% CIs for quintiles of deprivation (according to the Index of Multiple Deprivation (IMD)) in England.
Mortality rate
The overall mortality was 24 (0.4%). The median age of children who died was 67 months (range 0–14.8 years) (IQR 115.5); 18 were boys. Five children died at the scene of injury or on route to hospital, and six in the emergency department. All 13 who died during hospital admission had a GCS<8 recorded in the emergency department and intracranial injury, five of whom had associated skull fractures, four of which were complex fractures. Fourteen children had been involved in motor vehicle accidents (MVAs; three passenger-related, three involved cyclists, and eight were pedestrian-related), four were cases of suspected abusive head trauma, three were falls-related, and other mechanisms were recorded in three cases. Only three children were taken directly to a hospital with paediatric major trauma facilities; nine children were transferred to a second hospital to access neurosurgery facilities. The majority (20) of deaths occurred within the first 24 h of the incident.
Cause of head injuries
Half of the incidents, 2882 (50.6%), happened in the home, 874 (15.3%) in school/nursery, and 780 (13.7%) on road/street/motorway; 645 (11.3%) took place at other locations—for example, park, swimming pool, supermarket (missing data, 519 (9.1%)).
The majority, 3537 (62.1%), of head injuries were the result of falls in preschool children (table 1). Among causes of head injuries in infants, 887/1093 (81.1%) were falls and this included babies who had been dropped or fallen from furniture, Moses baskets, car seats, etc.
Cause of head injury in children: gender, age, number and proportion of (a) children referred to social services and (b) abnormal head CT scans by cause
Sports and recreation activities caused 783 (13.7%) of the injuries in the older children; there was a strong male preponderance. The most common sports associated with injury were: rugby, 143 (39.6%); football, 115 (31.9%); horse-riding, 62 (17.2%); trampolining, 28 (7.8%); hockey, 11 (3%). The recreational activities included sledging (38/154 (24.7%)), using a scooter (27 (17.5%)), and skateboarding (24 (15.6%)).
The 403 (7.0%) MVAs principally affected primary-school-aged children; 279 (69.2%) were pedestrians (median age 6.5 years), 35 (8.7%) were cyclists (median age 12.2 years), and 89 (22.1%) were in cars (median age 11.3 years).
The injury was the result of impact in 701 (12.3%) cases (median age 3.7 years): colliding with each other; running into walls, doors, radiators, etc; household item falling on the child. In 119 (2.1%) cases, the child was the victim of assault.
Overall, 357 (6.2%) of the children were referred to social care for a child protection investigation (median age 13 months (range 0–14.9 years)). These cases were associated with a history of assault or where the cause of head injury was unknown. There was a significant (p<0.001) association between the children referred to social care because of child protection concerns and social deprivation. Prevalence ranged from 25/775 (3.2%: 95% CI 2.2% to 4.7%) in the least deprived quintile to 129/1273 (10.1%: 95% CI 8.6% to 11.9%) in the most deprived quintile.
Severity of injury
A GCS score was recorded in 4182 (73.4%) cases. When it was not recorded, there was an AVPU score in 986 (17.3%) cases. The majority, 4522 (79.3%), of children had a GCS score of 15 or AVPU of Alert. There was a greater tendency not to record the level of consciousness in infants and those who were younger than 5 years than in the older age groups, and a trend towards greater neurological impairment with age (table 2). The relative OR for neurological impairment (GCS≤14) with respect to ‘fall from <1 m or <5 stairs’ for ‘MVA’, ‘sport/recreational’ and ‘fall from height’ was 4.00 (95% CI 2.99 to 5.36), 1.96 (95% CI 1.50 to 2.56) and 1.35 (95% CI 1.05 to 1.73), respectively. For ‘assault’ and ‘impact’, these ORs were not significant.
Neurological status of children with head injury and number and proportion of children with abnormal head CT scan in each age group
Additional injuries that were serious enough in themselves to warrant hospital admission were recorded in 1751 (30.7%) of the children; 490 (28%) were to the head or neck, 41 (2.9%) to the chest or abdomen, 19 (1.1%) were spinal, 90 (4.6%) were to the limbs, 16 (0.9%) to the pelvis, and 2 (0.1%) were burns. There was a statistically significant association (χ2=53.98, df=3, p<0.001) between additional injuries and low GCS score.
A head CT was performed in 1734 (30.4%) children, 249 (14.4%) of whom had intracranial injury (14 had an associated depressed fracture and 113 a simple linear fracture). A total of 148 (8.9%) had a simple skull fracture only, 20 (11.5%) had a depressed fracture only, and 48 (2.9%) had other findings (eg, subarachnoid cysts, extracerebral fractures or swellings). CT was reported as abnormal, but details of findings were missing for 72 cases. Abnormalities were therefore recorded on CT in 536 (9.4%) cases overall. The proportion of cases of abnormal CT was greatest in infants and children between 10 and 14 years and varied with cause of injury. Of the children who had fallen, 269/3537 (7.6%) had an abnormal CT, as did 100/403 (24.8%) of children whose injury was due to an MVA or the cause was unknown (26/106 (24.5%); table 1).
Status at 72 h after the injury
The majority of children, 4857 (88.3%), were admitted for one night or less. At 72 h after the injury, 132 (2.3%) were still inpatients in the first hospital, 385 (2.3%) had been transferred to the second hospital, and the status of 17 (3%) was not known.
Discussion
The Confidential Enquiry provides a detailed description of the cause, pattern and severity of childhood head injuries in England, Wales and Northern Ireland. It confirms that the majority of children had a minor head injury and were admitted for 24 h or less. One in 10 children had an intracranial injury or skull fracture. The mortality rate was 1 in 250, predominantly among victims of MVAs or abusive head trauma.
The proportion of children with minor head injury remains similar to previous studies described in a systematic review which gave a range of 76–92%.20 This has changed little over the past 25 years2 ,4 and represents a significant workload for health services. It is increasingly recognised that children with mild traumatic brain injury can have cognitive impairment or post-concussion syndrome21 ,22 and must be carefully assessed and given appropriate post-head-injury advice to identify and minimise sequelae.23
The peak prevalence was in children younger than a year, which differed from other studies, where the peak was in children aged 1–2 years.8 ,9 ,24 This was a surprising finding in a group of children who were not yet walking, but included babies who had been dropped or fallen from items of furniture or from baby products.25 While a lack of supervision or vigilance may have contributed to the injuries in the first place, parental anxiety may influence hospital attendance, and clinician concern may increase the rate of admission for observation and investigations in this very young population.
The association between social deprivation and childhood injuries was confirmed in a systematic review by Laflamme et al.26 The authors propose that ‘children from poor families…are more exposed to a wider range of hazards, and their care provider or themselves lack the means to protect themselves…or the ability to give adequate parental supervision, parental knowledge about safety mechanisms to prevent child injury is lacking’.
The likelihood of having an abnormal CT scan was 1 in 13 for a young child with a head injury from any fall, rising to 1 in 4 for high-velocity head injuries from an MVA or where the cause of injury was unknown. A proportion of the latter group had suspected abusive head trauma, which would account for the high morbidity.
The associations between age, causation and social deprivation have the potential to inform targeted prevention. Falls were most prevalent in infants and toddlers and took place in the home. This would suggest the need for inclusion in home-based safety interventions.27 Falls prevention has been recognised as one of five injury prevention priorities in a joint report from Public Health England and the Child Accident Prevention Trust supported by the Royal Society for the Prevention of Injuries.28 A more detailed analysis of this dataset identified specific items from which children had fallen.25
Older children experienced more sports and recreational injuries. The male preponderance8 ,29–31 is likely to reflect exposure, as rugby and football were listed as the most common activities. The proportion of children involved in an MVA was lower than in previous studies.6 ,8 ,9 Although these figures fit with the general reduction in MVAs,32–34 caution should be exerted when interpreting the findings from this study completed during winter months when children are not playing outside. Environmental prevention interventions including sports and cycle helmets, traffic calming measures, and road safety provision must be sustained for this age group.
An estimated 6.2% were referred to social care for child protection concerns, predominantly infants; the diagnosis of physical abuse or neglect must always be considered in the absence of a plausible explanation or where there are concerns about the level of appropriate supervision.
The peak time of injury was between early afternoon and 8 o'clock and has been reported in previous publications of childhood trauma.6 ,35 This referral pattern has implications for the optimal service planning of paediatric emergency departments.
A study limitation is that data were collected for a 6-month time period during the winter. This was not ideal, but the data collection was only funded for a 6-month time period. Figures may under-represent childhood head injuries that show peak prevalence in the summer.6 ,36 The nature of the data collection resulted in data being missed to a varying extent, which limited the statistical outcomes. However, for all categories analysed, there were less than 10% missing data fields. The dataset had the same age and regional distribution as seen in national HES data, and monthly distribution of cases enrolled into the study followed a similar distribution to that for serious injuries set out in the TARNLET report 201435 over the same 6-month period. Data were returned from more than 90% of eligible hospitals, and we are confident that the sample is representative of the national picture for the time period studied.
The Confidential Enquiry enabled us to describe the patterns of hospital admission for children with head injury across the UK. Since the data were collected, health services for these children have been revised, with the introduction of regional trauma networks in April 201237 and revision of the National Institute of Health and Care Excellence (NICE) head injury guidelines in 2014.23 This dataset provides a baseline national profile of head injuries in children to evaluate these health service and clinical reforms.
Acknowledgments
This project/audit is commissioned by the Healthcare Quality Improvement Partnership (HQIP) as part of the National Clinical Audit and Patient Outcomes Programme (NCAPOP). We thank the local coordinators at each of the 216 hospitals, without whom these data could never have been compiled (see online supplementary file 1 for lists of the participating hospitals). This is one of a series of forthcoming publications using the study data.
References
Footnotes
Twitter Follow Richard Edwards at @paedneurosurg
Contributors LT: undertook the statistical analysis and wrote the first draft of the manuscript. RH: designed the original data collection tools, supervised data collection, cleaning and data entry of the data collected within the original Confidential Enquiry into Head Injury in Childhood (CMACE). GP: director of the CMACE confidential enquiry, supervised the design and running of the project, and has been involved in editing the manuscript. RE, PH, IM, RCP: members of the project Independent Advisory Board and gave advice and editorial supervision at regular intervals during the study analysis. AK: principal investigator on the data analysis, coordinated the study writing, checked and edited the manuscript, and agreed the concept and methodology of this particular analysis.
Funding Health Quality Improvement Partnership, grant number 504835.
Competing interests None declared.
Ethics approval Central Manchester Research Ethics Committee (Ref 09/H1008/74).
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement The original data from this study have been destroyed in line with the requirement of the section 251 specification.