Article Text

Abstract
Background Short-course oral corticosteroids are commonly used in children but are known to be associated with adverse drug reactions (ADRs). This review aimed to identify the most common and serious ADRs and to determine their relative risk levels.
Methods A literature search of EMBASE, MEDLINE, International Pharmaceutical Abstracts, CINAHL, Cochrane Library and PubMed was performed with no language restrictions to identify studies in which oral corticosteroids were administered to patients aged 28 days to 18 years of age for up to and including 14 days of treatment. Each database was searched from their earliest dates to December 2013. All studies providing clear information on ADRs were included.
Results Thirty-eight studies including 22 randomised controlled trials (RCTs) met the inclusion criteria. The studies involved a total of 3200 children in whom 850 ADRs were reported. The three most frequent ADRs were vomiting, behavioural changes and sleep disturbance, with respective incidence rates of 5.4%, 4.7% and 4.3% of patients assessed for these ADRs. Infection was one of the most serious ADRs; one child died after contracting varicella zoster. When measured, 144 of 369 patients showed increased blood pressure; 21 of 75 patients showed weight gain; and biochemical hypothalamic–pituitary–adrenal axis suppression was detected in 43 of 53 patients.
Conclusions Vomiting, behavioural changes and sleep disturbance were the most frequent ADRs seen when short-course oral corticosteroids were given to children. Increased susceptibility to infection was the most serious ADR.
Trial registration number CRD42014008774. By PROSPERO International prospective register of systematic reviews.
- General Paediatrics
- Paediatric Practice
- Pharmacology
- Therapeutics
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
What is already known on this topic
Short-course oral corticosteroids are widely used in children to treat conditions such as asthma and croup.
Corticosteroids are known to be associated with many adverse drug reactions (ADRs).
What this study adds
Vomiting, changes in behaviour and sleep disturbance are the most frequent ADRs associated with short courses of corticosteroids. The incidence for each is between 5.4% and 4.3%.
Vomiting is the most common reason for discontinuing corticosteroids.
Increased susceptibility to infection is the most serious ADR associated with short courses of corticosteroids, with up to 1% of patients experiencing it.
Introduction
For over 50 years, corticosteroids have been used in a wide array of medical conditions as therapeutic and diagnostic tools, predominantly for their immunosuppressant and anti-inflammatory properties. Adverse drug reactions (ADRs) to corticosteroids are known to be associated with the size of the dose, the route of administration and the length of time for which the drug is prescribed. Many ADRs have been reported, such as mood and behaviour changes, vomiting, hypothalamic–pituitary–adrenal (HPA) axis suppression, increased blood pressure and insomnia.
The duration of corticosteroid therapy varies depending on the medical condition being treated and the pathology of the patient. Different definitions have been used for short duration or short courses of corticosteroids. The current British guideline for treatment of acute asthma advises using oral corticosteroids from 3 to 7 days,1 however the previous guideline (2008) advised use from 7 to 14 days.2
While ADRs caused by corticosteroids are well recognised and documented in the summaries of product characteristics (SPC) for relevant products, the toxicity of short-course oral corticosteroids has not been extensively evaluated and their relative risks are unclear. We therefore performed a systematic review to determine the toxicity associated with short-course oral corticosteroids, to identify the most common and serious ADRs and to determine their relative risk levels. We defined short-course oral corticosteroids as use for 14 days or less.
Methods
A systematic literature search was performed to identify all papers describing toxicity of corticosteroids in children. Six databases were searched up to December 2013: MEDLINE, EMBASE, International Pharmaceutical Abstracts, CINAHL, Cochrane Library and PubMed. The databases were searched separately and combined together to remove duplications. The search strategy included all languages and involved the keywords ‘prednis* or dexamethasone or betamethasone’ which are the most frequent medications given orally to children for short periods. ‘Corticosteroid’ was added to cover all other oral corticosteroid medication. The keywords ‘toxicity* or adverse drug reaction* or adverse event* or side effect* or adverse effect*’ were used as recommended by the BMC Medical Research Methodology for systematic reviews of adverse effects.3 Additionally, the keyword ‘safety*’ was used as in a previous systematic review.4 The terms recommended by search strategies for MEDLINE were used to cover the paediatric age group ‘child* or children* or p*ediatric* or infant* or adolescent*’.5 The terms neonate, newborn and gestation were excluded. The keywords oral, tablet, syrup and PO (abbreviation meaning by mouth) were used to cover all possibilities of oral administration of corticosteroids.
Inclusion criteria were original research studies assessing corticosteroid toxicity in children from 28 days up to 18 years of age. These included randomised controlled trials (RCTs), case series, case reports, cohort studies and letters. Five per cent of randomly selected abstracts were independently assessed for eligibility by a second reviewer for assurance that no relevant studies were missed. Data including the number of patients, drug name, duration of use, diagnosis, number and type of ADRs were extracted.
Exclusion criteria included review articles, editorials, studies that did not give ADR data, studies in adults, studies involving adults and children in which paediatric data were not presented separately, and studies in which corticosteroids were not given orally and/or were administered for more than 14 days.
Meta-analysis of included RCTs was performed using RevMan 5.2. This is software provided by Cochrane, used for organising the quality assessment for RCTs and for carrying out meta-analysis. The quality of included RCTs was assessed using the Cochrane collaborations tool for assessing risk of bias in randomised trials.6 Any study showing a high risk of bias on three or more parameters was thereafter excluded.
Prospective cohort studies were assessed using the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) checklist,7 for which a score of over 70% is required for inclusion. Other studies were quality assessed using the Health Technology Assessment checklist.8 All studies achieving at least satisfactory criteria were included. All quality assessments were independently assessed for eligibility and scored by two reviewers using a specially designed form. Any discrepancies were resolved by a third reviewer.
The incidence of ADRs was calculated from the RCTs and prospective cohort studies when more than one study reported the ADR.
Results
Eight thousand and ninety-five articles were identified in total. Thirty-eight articles met the inclusion criteria after four papers were added from manual searches of bibliographies,9–46 and five articles were excluded after quality assessment. The remaining articles were excluded for the reasons shown in figure 1.
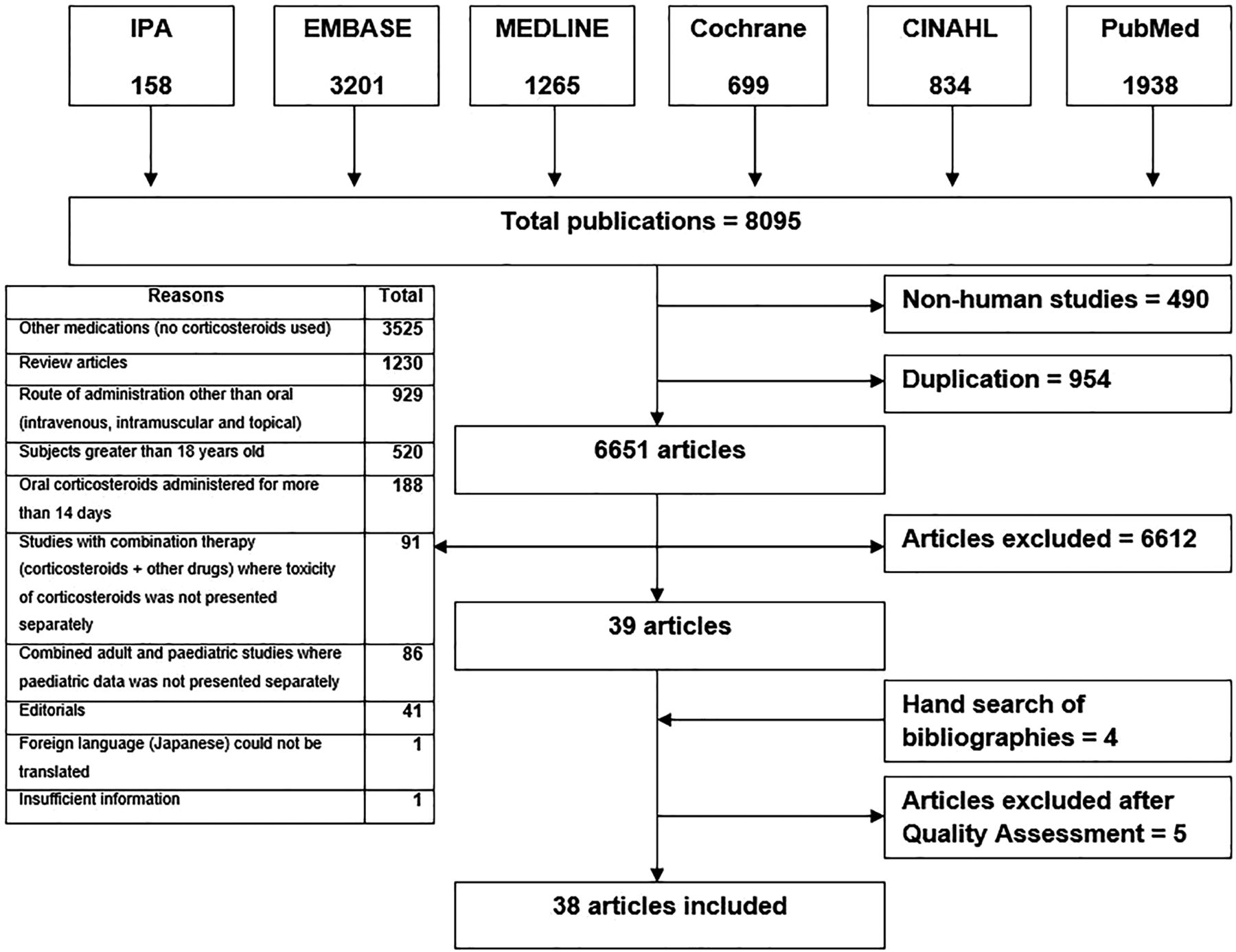
Flow chart of the literature search performed.
Corticosteroids were used to manage various medical conditions, including asthma, bronchiolitis, croup, acute renal failure, allergic rhinitis, dengue fever, infantile spasms, nephrotic syndrome, acute leukaemia, acute idiopathic thrombocytopenic purpura and systemic lupus erythematosus. Prednisolone and dexamethasone were the most commonly used drugs.
The studies included a total of 3200 patients and 850 ADRs (table 1). RCTs accounted for over half of the studies, 89% of patients and 60% of ADRs.9–30 The five prospective cohort studies included less than 10% of patients (n=305) but reported one-third of the ADRs.31–35 Prospective cohort studies detected more ADRs per patient than RCTs.
Thirteen studies looked for all possible symptomatic adverse events10 ,12–16 ,18 ,21 ,24 ,27–30 and one of them also evaluated HPA axis suppression.20
Four studies looked for vomiting only,9 ,11 ,22 ,26 and one study looked specifically for vomiting, nausea and abdominal pain.34
Two studies evaluated HPA axis suppression only,17 ,35 and one study evaluated blood pressure and HPA axis suppression.19
One study looked for sleep disturbance only,33 one for behavioural change only,32 and one evaluated bone mineralisation only.20
Two studies were questionnaires based on parental response to specific questions about specific ADRs such as behavioural changes.23 ,31
One study evaluated patient's blood pressure and blood glucose.25
Summary of included articles
Overall, six studies measured patient's blood pressure,12 ,19 ,21 ,25 ,29 ,30 four studies measured blood glucose12 ,25 ,29 ,30 and two studies measured weight.21 ,31
Twenty-one different ADRs were reported from the RCTs and prospective cohort studies (tables 2 and 3). The three most common side effects were vomiting, changes in behaviour and disturbed sleep, affecting between 5.4% and 4.3% of children.
Observed/reported adverse drug reactions (ADRs) from RCTs and prospective cohort studies
Adverse drug reactions (ADRs) from RCTs and prospective cohort studies requiring specific measurements
Six RCTs evaluated blood pressure in 369 patients. Four studies reported increased blood pressure in 144 of 186 patients.19 ,21 ,25 ,30 Two studies showed no change in blood pressure in 183 patients.12 ,29 Overall, 39% of patients measured showed increased blood pressure. The definition of increased blood pressure varied between studies. One study defined it as diastolic blood pressure >85 mm Hg.21 Mean increases of 3–7 mm Hg were described in one study.25
Four studies (three RCTs, one prospective cohort study) and one case series specifically evaluated HPA axis suppression.17–19 ,35 ,36 Forty-three of the 53 patients tested showed biochemical HPA axis suppression. Meta-analysis across three RCTs showed statistically significant biochemical HPA axis suppression associated with oral corticosteroids compared with inhaled corticosteroids (fixed model, I²=54%, p=0.00001, RR=6.7). This risk was greater with oral prednisolone than with inhaled budesonide, nebulised fluticasone and intranasal beclomethasone (figure 2).

Relative risk of hypothalamic–pituitary–adrenal axis suppression: oral prednisolone and inhaled corticosteroids.17–19
Eighteen different ADRs were reported from case series and case reports with a total of 51 ADRs in 31 patients (table 4). Varicella zoster infection was reported in three patients taking oral prednisolone.39–41 All were admitted to intensive care and one died.
Adverse drug reactions (ADRs) from case series and case reports
Medication was stopped in 44 patients due to ADRs. The rate of discontinuation was 1.4%. Vomiting was the most common reason from seven RCTs and involved 36 children (35 with prednisolone and one child with dexamethasone).9 ,10 ,14 ,15 ,22 ,26 ,27 Behavioural changes were the second most common reason for discontinuing the medication (four children) from two RCTs30 ,33 and one cohort study.42 The ADR resulting in discontinuation was not stated for three children in one RCT.16
Three studies compared prednisolone (base) tablet or syrup and oral dexamethasone for the risk of vomiting.11 ,14 ,15 Vomiting was reported in 38 out of 411 children taking prednisolone, and 11 out of 416 children taking dexamethasone. The risk of vomiting was significantly greater with prednisolone base tablet or syrup (figure 3) (fixed model, I²=30%, p=0.0001, RR=3.62). Prednisolone sodium phosphate solution, however, had a lower risk of vomiting than both (prednisolone (base) solution and oral dexamethasone).22 ,34

{kind=link}
{kind=link}
{kind=link}
Three studies (one RCT, one cohort study and one case series) evaluated weight changes in patients.21 ,31 ,37 Thirty of the 84 patients measured showed weight gain. The definition of an increase in body weight varied between studies, one study defined the increase in body weight as more than 500 g over the pretreatment value.21
Discussion
The most serious side effect associated with short courses of oral corticosteroids was infection due to their immunosuppressant action. Five RCTs reported that 20 children experienced infection during treatment periods (incidence 0.9%). Three cases were reported of children infected with varicella zoster, one of whom died and the other two were admitted to the intensive care unit with severe complications.39–41
HPA axis suppression is another potentially serious ADR associated with the use of oral corticosteroids. This suppression may lead to stress-induced acute adrenal crisis or growth retardation. In four studies specifically looking for this, 43 children showed a statistically significant biochemical suppression of the HPA axis. One case series also showed a significant occurrence of transient HPA axis suppression in 3 of 11 children with a 5-day course of prednisolone (2 mg/kg/day). All the children returned to a normal level of endogenous cortisol secretion within 10–12 days after discontinuation of the corticosteroids.17–19 ,35 ,36 Overall, when this was measured, 81% of children receiving short-course oral corticosteroids showed biochemical HPA axis suppression. Studies in adults suggest that high-dose oral prednisolone (50 mg/day) for 5 days does not suppress the HPA axis.47 A recent study found no differences between short-course oral and inhaled corticosteroids in terms of biochemical HPA axis suppression48 and stated that the clinical consequences of biochemical suppression needs further study.
The three most commonly observed ADRs associated with short-course oral corticosteroids were vomiting, changes in behaviour and disturbed sleep. Vomiting was the most common side effect with an incidence of 5.4% of patients and was the most frequent reason for withdrawal of oral corticosteroids. Our systematic review suggests that different dosage forms of oral prednisolone had a different incidence of vomiting. Prednisolone sodium phosphate solution was less likely to cause vomiting than other formulations (prednisolone base solution and dexamethasone solution).22 ,34
Mood swings and behavioural disturbance were the second most frequently observed adverse events with an incidence of 4.7%. Mood swings (anxiety, hyperactivity and aggressive behaviour) were significantly more frequent with higher doses (2 mg/kg/day or 60 mg/m²/day) of oral prednisolone than with lower doses (1 mg/kg/day).23 ,31 ,32 In adult patients, behaviour and mood changes were distinctly less common at doses of prednisolone under 20 mg/day compared with patients who received 60 mg/day.49
Sleep disturbance was the third most frequent observed adverse event caused by oral corticosteroids, with an incidence of 4.3%. Two studies (one RCT and one cohort study) reported 101 children had sleep disturbances. An observational study also reported that all children who received oral dexamethasone for the treatment of leukaemia experienced sleep disturbance.33 One RCT reported an infant who received oral prednisolone for the treatment of infantile spasms with this event.30
Corticosteroids lead to an increase in blood pressure by increasing the resistance in the body's vascular system, increasing intracellular volume, and increasing cardiac contractility. Overall, even though more than one-third of the children tested experienced an increase in blood pressure, the majority did not need antihypertensive drugs or withdrawal of medication. Two patients with infantile spasms had an increase in blood pressure above 120/90 mm Hg and received diuretics without stopping their medication.30 The clinical significance of raised blood pressure following short-course corticosteroids needs further study.
Prospective cohort studies were the most effective at detecting ADRs. RCTs are the gold standard for determining effectiveness of therapy, but are often underpowered to evaluate toxicity.
In conclusion, this systematic review showed the most serious ADR associated with short-course oral corticosteroids was infection which was reported in 1% of patients. The most frequent ADRs were vomiting, behavioural change and sleep disturbance. Vomiting was the main reason for treatment discontinuation. Weight gain was experienced by more than one-third of patients when this was measured.
References
Footnotes
Contributors FA, IC and SC conceived the idea and designed the study as part of FA’s PhD. FA did the literature search and extracted the data and wrote the first draft. IC and SC reviewed and validated the extracted data and revised the paper.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.