Article Text

Abstract
Objectives This study aimed to investigate the incidence of short stature at 3 years of age in a Japanese cohort of late preterm infants who were born at 34–36 weeks’ gestational age (GA). We compared these late preterm infants with term infants (37–41 weeks’ GA), and evaluated the effect of birth weight on the incidence of short stature.
Methods A longitudinal population-based study of 26 970 neonates who were born between 34 weeks’ and 41 weeks’ GA in 2006–2008 was conducted in Kobe, Japan. Of these neonates, 1414 were late preterm and 25 556 were term infants. The late preterm infants were then divided into three subgroups based on birth weight as determined by Japanese neonatal anthropometric charts for GA at birth: large-for-GA (n=140), appropriate-for-GA (AGA, n=1083), and small-for-GA (SGA, n=191). The incidence of short stature at 3 years of age was calculated in the late preterm group and compared with that in the term group, and between the AGA and SGA groups with late preterm birth.
Results The incidence of short stature in the late preterm group was 2.9%, which was significantly higher than that in the term group (1.4%). Late preterm SGA infants developed short stature with a significantly higher (9.4%) incidence than that of late preterm AGA infants (2.1%).
Conclusions The incidence of short stature in 3-year-old children who were late preterm infants has a 2-fold higher risk than that in term infants. The risk of developing short stature is increased 4.5-fold if they are SGA.
- Growth
- Epidemiology
- Comm Child Health
Statistics from Altmetric.com
What is already known on this topic?
-
Late preterm infants have an increased risk of neonatal mortality and morbidity including neurodevelopmental disorders in infancy when compared with term infants.
What this study adds?
-
Late preterm infants have a twofold higher risk of short stature at 3 years of age than term infants.
-
The risk of short stature is increased by 4.5-fold if they are born small-for-gestational age, regardless of birth length and ponderal index values.
Introduction
Late preterm infants are defined as those who are born at 34–36 weeks’ gestational age (GA).1 During the last 30 years, births have decreased from 1.58 million in 1980 to 1.03 million in 2012 in Japan. However, the proportion of preterm births between 32 weeks’ and 36 weeks’ GA, including late preterm birth, increased by 3.6% in 1980 to 5.0% in 2012.2 Therefore, health outcomes in late preterm infants have attracted attention in Japan.
Late preterm infants are at higher risk of neonatal morbidity than term infants who are born at 37–41 weeks’ GA, with feeding difficulties, hypoglycaemia, jaundice, respiratory distress and sepsis.1 ,3 Neurodevelopmental and educational outcomes are also worse in late preterm infants compared with those in term infants.4–6 Growth impairment, such as short stature, is an important factor to examine in the follow-up of late preterm infants. However, no population-based studies have focused on the incidence of short stature in late preterm infants. One hypothesis is that late preterm birth is a risk factor for short stature. Additionally, because it is not clear if late preterm birth and some physical factors at birth are risk factors for short stature, another hypothesis is that the ponderal index (PI), which indicates the intrauterine nutritional state (possibly, fetal programming), is used as a predictive index for short stature in infancy.
The objectives of this population-based study were (1) to longitudinally investigate the incidence of short stature at 3 years of age in children who were late preterm infants using a cohort of neonates who were born and followed up in Kobe, Japan, and to compare it between children who were late preterm and term infants, and (2) to investigate the effects of GA and physical factors at birth (birth weight (BW), birth length (BL), and PI) on the incidence of short stature at 3 years of age.
Patients and methods
Study design
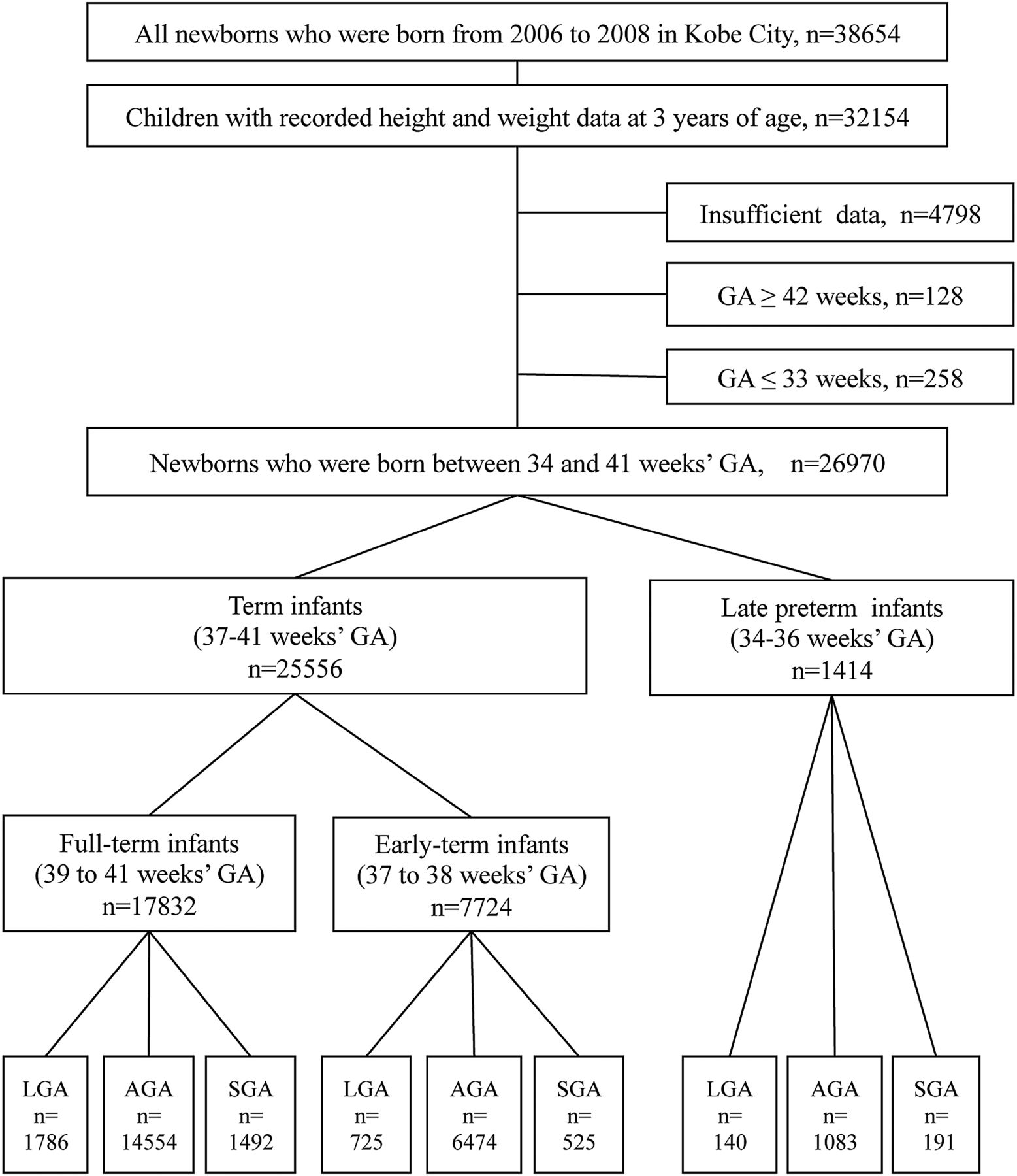
A population-based study of 32 154 children who were born between 2006 and 2008 and followed up with height and weight measurements until 3 years (36–47 months) of age was conducted in Kobe City, Japan (figure 1). Written informed consent from the parents of the children was obtained. Information regarding data at birth, such as GA, BW, BL, the mother's history of childbirth, pregnancy-induced hypertension and smoking during pregnancy were collected on the basis of the maternity health records, which were managed in Kobe City Public Health Centers. The children's height and weight were measured at 3 years of age and collected at different Kobe City Public Health Centers, which are located at 11 places in Kobe.

Flow chart of the subjects.
Data were managed based on the act of personal information protection in Kobe City. The analysis using anonymous data was approved by the Planning and Coordination Bureau of Kobe, and was then carried out at Kobe University Graduate School of Medicine.
Subjects
The height and weight data at 3 years of age were recorded in 32 154 children. Of these children, 5184 were excluded because of insufficient data for analysis of this study (n=4798) or gestation at birth was ≥42 weeks (n=128) or ≤33 weeks (n=258). Of the remaining 26 970 children, 1414 (5.2%) were late preterm births and 25 556 (94.8%) were term births. The 25 556 term infants were divided into full term (39–41 weeks’ GA, n=17 832) and early term infants (37–38 weeks’ GA, n=7724). Each group was then divided into three subgroups based on Japanese neonatal anthropometric charts for GA at birth:7 BW ≥ the 90th centile (large-for-gestational age (LGA)), BW between the 10th to 90th centiles (appropriate-for-gestational age (AGA)), and BW < the 10th centile (small-for-gestational age, (SGA), figure 1).
Among the 4798 children with insufficient data, 85 were born at ≤33 weeks’ GA, 207 were born at 34–36 weeks’ GA, 3201 were born at 37–41 weeks’ GA, 11 were born at ≥42 weeks GA, and 1294 had an unknown GA. The proportion of effective and insufficient data was similar in those born at 34–36 weeks’ GA and those born at 37–41 weeks’ GA (34–36 weeks’ GA: effective data, n=1414 (87.2%) and insufficient data, n=207 (12.8%); 37–41 weeks GA: effective data, n=25 556 (88.9%) and insufficient data, n=3201 (11.1%)).
Methods
We analysed (1) the background characteristics at birth, (2) the proportion of SGA infants, (3) the incidence of short stature, (4) the severity in short stature, (5) the effects of GA and BW on the incidence of short stature and (6) the effects of BL and PI on the incidence of short stature, and compared them among the groups.
Definitions and calculations
BL was the length from the crown to heel at birth. All neonates, regardless of GA, underwent measurement of the BL with a measuring tape or ruler by trained midwives or nurses. The newborns were classified as BL ≥ 10th centile and BL <10th centile based on Japanese neonatal anthropometric charts for GA at birth.7 PI was calculated as follows: PI=100×BW (g)/BL (cm3).8 PI <2.2 and PI ≥2.2 shows asymmetrical and symmetrical fetal growth restrictions, respectively.8–10 Short stature was defined as a 2 SD score below the mean height for their age (36–47 months of age).11 Calculations of SD scores for BW, BL and height at 3 years of age were performed by using nordiFIT software (Novo Nordisk Pharma, Tokyo, Japan). This software can calculate SD scores according to sex-specific standards for BW and BL by GA, or height during infancy in the Japanese population.7 ,11
Statistical analyses
Statistical analyses were performed with the Student's t test or the χ2 test as appropriate using Excel Statistics (Statcel 3; Social Survey Research Information, Tokyo, Japan). Residual analysis using Microsoft Excel R was used for the analysis of the severity in short stature. Significant differences were deemed statistically significant when p<0.05.
Results
Background characteristics at birth
The background characteristics at birth of our cohort are shown in online supplementary table. BW, BL and their SD scores were significantly higher in LGA infants and lower in SGA infants than in AGA infants in the late preterm birth and term birth groups, as we expected. The proportion of a first birth in LGA infants was significantly higher than that in AGA infants, but no differences were found between SGA and AGA infants in all GA groups. The proportion of pregnancy-induced hypertension in SGA infants was significantly higher than that in AGA infants. In the full term group, the proportion of smoking during pregnancy in mothers who had SGA infants was significantly higher than that in those who had AGA infants.
Proportion of SGA infants
The proportion of SGA infants who had a late preterm birth (191/1414, 13.5%) was significantly higher than that of SGA infants who had a term birth (2017/25556, 7.9%, p<0.001). The proportion of SGA infants who had late preterm birth was also significantly higher than that of SGA infants who were early term (525/7724, 6.8%, p<0.001) and full term (1492/17832, 8.4%, p<0.001).
Incidence of short stature
The incidence of short stature in late preterm infants was 2.9%, which was significantly higher (2-fold) than that of term infants (1.4%, figure 2A). The incidence of short stature was highest in children with late preterm birth, followed by early term and full term birth (figure 2B). No effects of multiple births on short stature were found in children with late preterm birth (data not shown).
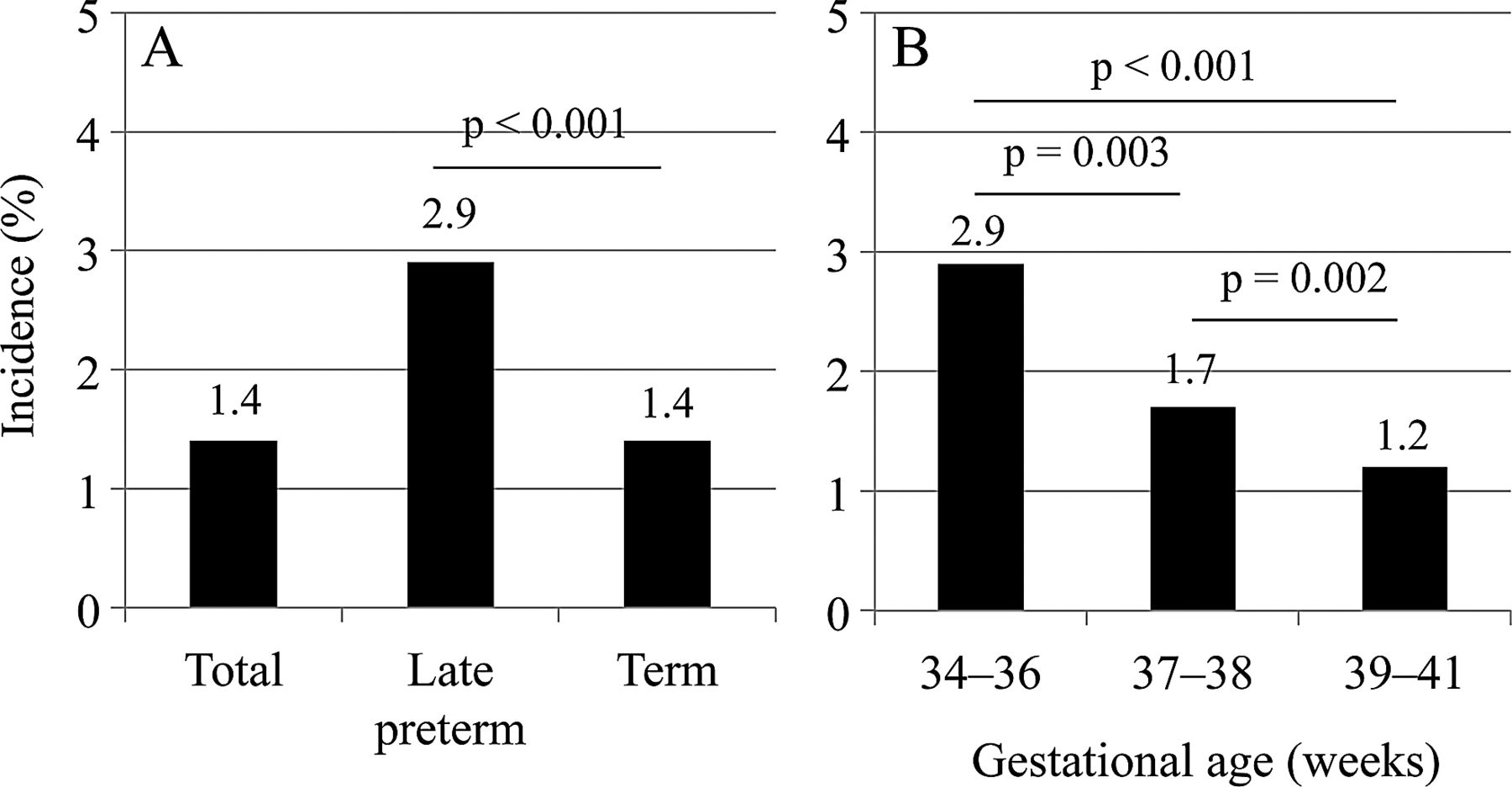
Incidence of short stature in children who were born at late preterm and term (A), and in those who were born at 34–36 weeks’ gestational age (GA) (late preterm), 37–38 weeks’ GA (early term), and 39–41 weeks’ GA (full term) (B).
Severity in short stature
No statistically significant difference in the proportion of children with a severely short stature was found between the late preterm and term birth groups (table 1).
Comparison of severity in short stature at 3 years of age between children who had a late preterm birth and a term birth
Effects of GA and BW on the incidence of short stature
Figure 3 shows the effects of GA and BW on the incidence of short stature. In children born AGA and SGA, there was a significantly higher incidence of short stature in the late preterm and early term groups than in the full term group. However, no significant difference in the incidence of short stature was observed among children who were born LGA in the late preterm, early term and full term groups. We compared the incidence of short stature between children who were born AGA and SGA or LGA in the late preterm, early term, and full term groups. There was a significantly higher incidence of short stature in children who were born SGA than in those who were born AGA in all of the groups (4.5-fold 3.5-fold and 3-fold increases, respectively). In children who were born LGA, there was a significantly lower incidence of short stature than in those who were born AGA in the early term and full term groups, but not the late preterm group.

Effects of gestational age (GA) and birth weight on the incidence of short stature. *p<0.05, **p<0.01 compared with full term infants (39–41 weeks’ GA). AGA, appropriate-for-gestational age; LGA, large-for-gestational age; SGA, small-for-gestational age.
Effects of BL and PI on the incidence of short stature in AGA and SGA infants
In the early term and full term groups, but not but the late preterm group, AGA and SGA infants with a BL <10th centile had a significantly higher incidence of short stature than those with a BL ≥10th centile. Children with a PI <2.2 did not have a higher incidence of short stature than those with a PI >2.2 in all of the GA groups (figure 4).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Effects of birth length (BL) and ponderal index (PI) on the incidence of short stature in children who were born appropriate-for-gestational age (AGA) and small-for-gestational age (SGA).
Discussion
This population-based study showed for the first time that the incidence of short stature at 3 years of age in Japanese children who were born at late preterm was twofold higher than that in those born at term. Late preterm children who were born SGA had a significantly (4.5-fold) higher incidence of developing short stature than did those born AGA. In our study, 9.4% of late preterm infants who were SGA developed short stature at 3 years of age. This finding is similar to that in a Japanese study on a small number of SGA infants born between 32 weeks’ and 36 weeks’ GA (9%).12
Some population-based studies have already reported that there is a high incidence of short stature during infancy in those who were very premature infants, such as infants born <32 weeks GA.13 ,14 However, there are few reports focusing on late preterm infants. Boyle et al13 showed in their population-based study in the UK that height decreased across GA with increasing prematurity, and this effect was present at 3 years of age. They measured the mean height value of children who were late preterm infants (95.2 cm) and compared it with those who were born at 39–41 weeks’ GA (95.6 cm). A novel finding in our study was the higher incidence of short stature in children who were late preterm infants than that in those who were term infants, without a difference in the proportion of children with a severe short stature. Because this finding suggests that late preterm birth is a risk factor for the incidence of short stature at 3 years of age, prevention of preterm delivery, even late preterm birth, is important.
Concordant with many previous studies,12 ,15–17 our study also observed that SGA had a high risk for developing short stature in Japanese children who were late preterm and term infants. These results suggest that low BW affects the incidence of short stature when newborns have the same GA at birth. In our study population, the proportion of SGA in late preterm infants was approximately twofold higher than that in term infants. We speculate that a reason for the higher incidence of short stature in children who were born late preterm infants than in those who were born term infants might be due to a high proportion of SGA in late preterm infants. Suggested mechanisms of short statured children born SGA include a diminished sensitivity of somatotroph cells, pituitary growth hormone resistance and immaturity of the growth hormone receptor.18 Genetic abnormalities of the insulin-like growth factor-1 gene or insulin-like growth factor-1 receptor gene are other reported causes of short-statured children born SGA.19–22 Some children with a short stature should undergo extensive medical examinations and may receive growth hormone therapy as short-statured children born SGA.23 Our results suggest that SGA is an important factor for developing short stature at 3 years of age.
A short BL is a risk factor for short stature at an adult age in term infants with SGA.17 Therefore, we investigated the effect of BL on the incidence of short stature at 3 years of age. Our results suggest that BL affected short stature at 3 years of age in SGA, and in AGA, in term infants. However, no effect of BL on the incidence of short stature in those who were late preterm infants was found, suggesting that late preterm birth is at risk of short stature, regardless of BL. We also chose PI as another physical index at birth and determined the effect of PI on the incidence of short stature at 3 years of age. The PI shows impaired fetal growth in newborns at birth, with the intrauterine nutritional state as a possible index of fetal programming.8–10 ,18 Contrary to our hypothesis, our results suggest that PI cannot be used as a predictive index for short stature at 3 years of age.
The major limitation of this study is that the cause of short stature and obstetric antecedents could not be identified. This is because our population-based study used data from health check-ups. Second, the measuring technique of BL with a tape measure or ruler was suboptimal. Third, we could not obtain data of parents’ height also to predict the final height of their children. However, despite having some limitations, this study showed, for the first time, the incidence of short stature at 3 years of age in children who were late preterm and term infants using a population-based study. Further studies are required to investigate the incidence of short stature in children who were born extremely preterm infants, who should be at higher risk than late preterm infants.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online supplement
Footnotes
-
MN and IM contributed equally.
-
Contributors MN and IM conceptualised and designed the study, carried out the initial analyses and drafted the initial manuscript. TY, KF, DK, TK and AS analysed the data and reviewed the manuscript. YI carried out statistical analyses. EU and CS collected the data in this study. KI and HY critically reviewed the manuscript. All authors approved the final manuscript as submitted and agree to be accountable for all aspects of the work.
-
Funding This work was supported in part by Scientific Grants-in-Aid from the Ministry of Education, Culture, Sports, Science and Technology of Japan (23791224), the Morinaga Hoshi-kai Foundation (H24), and the Public Health Research Foundation (2013).
-
Competing interests None.
-
Patient consent Obtained.
-
Ethics approval Review board at the Planning and Coordination Bureau of Kobe.
-
Provenance and peer review Not commissioned; externally peer reviewed.