Article Text

Abstract
Objective: To investigate factors associated with school attendance and physical function in paediatric chronic fatigue syndrome/myalgic encephalopathy (CFS/ME).
Design: Cross-sectional study.
Setting: Regional specialist CFS/ME service.
Patients: Children and young people aged under 18 years.
Outcome measures: Self-reported school attendance and physical function measured using the physical function subscale of the Short Form 36.
Methods: Linear and logistic regression analysis of data from self-completed assessment forms on children attending a regional specialist service between 2004 and 2007. Analyses were done in two groups of children: with a completed Spence Children’s Anxiety Scale (SCAS) and with a completed Hospital Anxiety and Depression Scale (HADS).
Results: Of 211 children with CFS/ME, 62% attended 40% of school or less. In children with completed SCAS, those with better physical function were more likely to attend school (adjusted odds ratio (OR) 1.70; 95% CI 1.36 to 2.13). This was also true for those with completed HADS (adjusted OR 2.05; 95% CI 1.4 to 3.01). Increasing fatigue and pain and low mood were associated with worse physical function. There was no evidence that anxiety, gender, age at assessment, family history of CFS/ME or time from onset of symptoms to assessment in clinic were associated with school attendance or physical function.
Implications: Paediatricians should recognise that reduced school attendance is associated with reduced physical function rather than anxiety. Improving school attendance in children with CFS/ME should focus on evidence-based interventions to improve physical function, particularly concentrating on interventions that are likely to reduce pain and fatigue.
Statistics from Altmetric.com
Chronic fatigue syndrome (CFS) or myalgic encephalopathy (ME) is the commonest cause of school absence in the UK.1 It is a relatively common condition, affecting between 0.1% and 2% of children aged under 18 years.2 3 4 5 6 7 CFS/ME is defined in the Royal College of Paediatrics and Child Health (RCPCH) evidenced-based guidelines of the management of CFS/ME as ‘“generalised fatigue persisting after routine tests and investigations have failed to identify an obvious underlying cause’.8 The National Institute for Health and Clinical Excellence (NICE) recently recommended that a minimum of 3 months of fatigue is required before a diagnosis of CFS/ME is made in children.9
CFS/ME has a negative impact on education for most children with the condition.10 Sixty-eight per cent of children report that having CFS/ME prevented them attending school at some stage, with a mean time out of school estimated at more than one academic year.11 Children with CFS/ME can also have poor physical function, with over 57% of children being bed-bound at some stage.11 Despite this there is currently little evidence on the factors that affect school attendance and physical function in children with CFS/ME.
This study investigated the relationship of school attendance, physical function, fatigue, pain, mood, time to assessment, age, sex and family history in children diagnosed with CFS/ME in a specialist CFS/ME clinic.
Methods
Patient cohort
The Bath specialist paediatric CFS/ME service covers a region in the south west of England with a population of some 400 000 children aged 5–19 years (2001 census). The service also offers assessment and treatment to children from out of the region who cannot access specialist services. More than 150 children and young people are assessed and treated each year. Children are assessed and offered treatment in outpatient clinics unless they are too severely affected to attend clinic, in which case they are seen at home.
Inventories
Before assessment, self-completed inventories measuring fatigue, anxiety, pain and physical function were collected: The 11-question Chalder fatigue scale was scored using the 0–3 method for scoring each question (0 for “less than usual”, 1 for “no more than usual”, 2 for “more than usual” and 3 for “much more than usual”).12 For the 10-question physical function subscale of the Short Form 36 (SF-36)13 (a well-validated health survey questionnaire) children scored between 1 (“yes limited a lot”) and 3 (“no not limited at all”) for each question, so that children with the worst physical function scored 10 whereas those with good physical function scored 30. A visual analogue scale was used to measure pain, with a score of 0 for “no pain” and 100 for “pain as bad as possible”.
Two inventories were used to assess mood. In the first 2 years of recruitment, the Spence Children’s Anxiety Scale (SCAS)14 was used for children aged up to 14 years and the Hospital Anxiety and Depression Scale (HADS) was used for children aged 14 years and over. After the second year of recruitment, the SCAS was used on all children. After the fourth year of recruitment the HADS was used in the assessment of children aged 12 years and older. The SCAS is a 38-question scale (with an additional six filler questions), which measures the frequency with which a child experiences symptoms relating to anxiety. Each question is scored as “never” (0), “sometimes” (1), “often” (2) and “always” (3). The HADS is a 14-question inventory with both anxiety and depression subscales.
Inventories were coded as missing if more than one question was missing, apart from the SCAS, which was coded as missing when there were more than two missing items. On the HADS, each seven-item subscale was excluded if there was more than one question missing. Questions for which two answers were given were coded as missing. Total scores were corrected for the number of missing items.
School attendance was measured by asking how the young person would describe their attendance (as a percentage of expected attendance). For analysis, school attendance was dichotomised as 40% or less or over 40%. Family history was collected during the clinical assessment as the presence or absence of CFS/ME in either the parents or siblings of the child assessed. Time to assessment was calculated as the time from symptom onset to assessment in the CFS/ME specialist clinic.
Statistical methods
We used logistic regression to investigate associations of school attendance with physical function (SF-36), fatigue, pain and anxiety (and depression in those over 14 years of age). We used linear regression to investigate associations of physical function with fatigue, pain and mood. So that regression coefficients for the different inventories were comparable, they were rescaled so that the range for each was approximately 10. Thus, SF-36, HADS anxiety and depression were divided by 2; SCAS anxiety and pain were divided by 10 and fatigue was divided by 3. All analyses were restricted to children with no missing data in any of the variables investigated. We checked linearity assumptions by grouping exposure variables into quintiles, then plotting graphs or examining regression coefficients. All analyses were performed separately for children with completed SCAS and for those with completed HADS.
Ethics
The North Somerset and South Bristol Research Ethics Committee decided that the collection and analysis of these data was part of service evaluation and as such did not require ethical review by a NHS research ethics committee or approval from the NHS R&D office (REC reference number 07/Q2006/48).
Results
Between March 2004 and December 2007, 294 children and young people aged under 18 years were offered assessment by the specialist CFS/ME service. In 11, the diagnosis was not recorded. Thirty children did not have CFS/ME at assessment and 42 did not fill in any pre-assessment questionnaires and were excluded from subsequent analyses. Of the remaining 211 children, 14 had incomplete information on the Chalder fatigue scale and 10 had incomplete information on the SF-36 score. Information on school attendance was missing for nine children.
Anxiety was measured using the SCAS in 162 children: 76 (86%) of those aged 13 years or younger and 86 (70%) of those aged 14 years or older. Anxiety was measured using the HADS in 108 children: 16 (18%) of those aged 13 years or younger and 92 (75%) of those aged 14 years or older. Seventy-three children had measures of both anxiety scores.
One hundred and sixty-two children (81% of 199 with sufficient information) would have been given a diagnosis of CFS/ME using the Centers for Disease Control and Prevention (CDC) criteria.15 16 Of those who would not have been given a CDC diagnosis, 23 had fewer than four symptoms and 14 others did not have fatigue for 6 months before assessment.
Table 1 shows characteristics of the 211 children with CFS/ME who provided some information on pre-assessment questionnaires. The median age was 14.6 years, and 146 (68%) were girls. The median time from symptom onset to assessment in clinic was 18 months. No information was available on family history for 32 children. Thirty-six children (20% of those in whom family history was available) had a first-degree relative with a history of CFS/ME.
Characteristics of children and young people with CFS/ME who provided some information on pre-assessment questionnaires
Although the majority of children were seen from within the region covered by the service, 29 (14%) children were referred from out of the region. There was little evidence of differences in severity between these children within and out of the region, apart from a difference in disability as measured by the SF-36, which was more severe for out-of-region (mean 16.9) than in-region (mean 20.4) assessments (difference −3.5, 95% CI −5.6 to −1.5).
Factors associated with school attendance
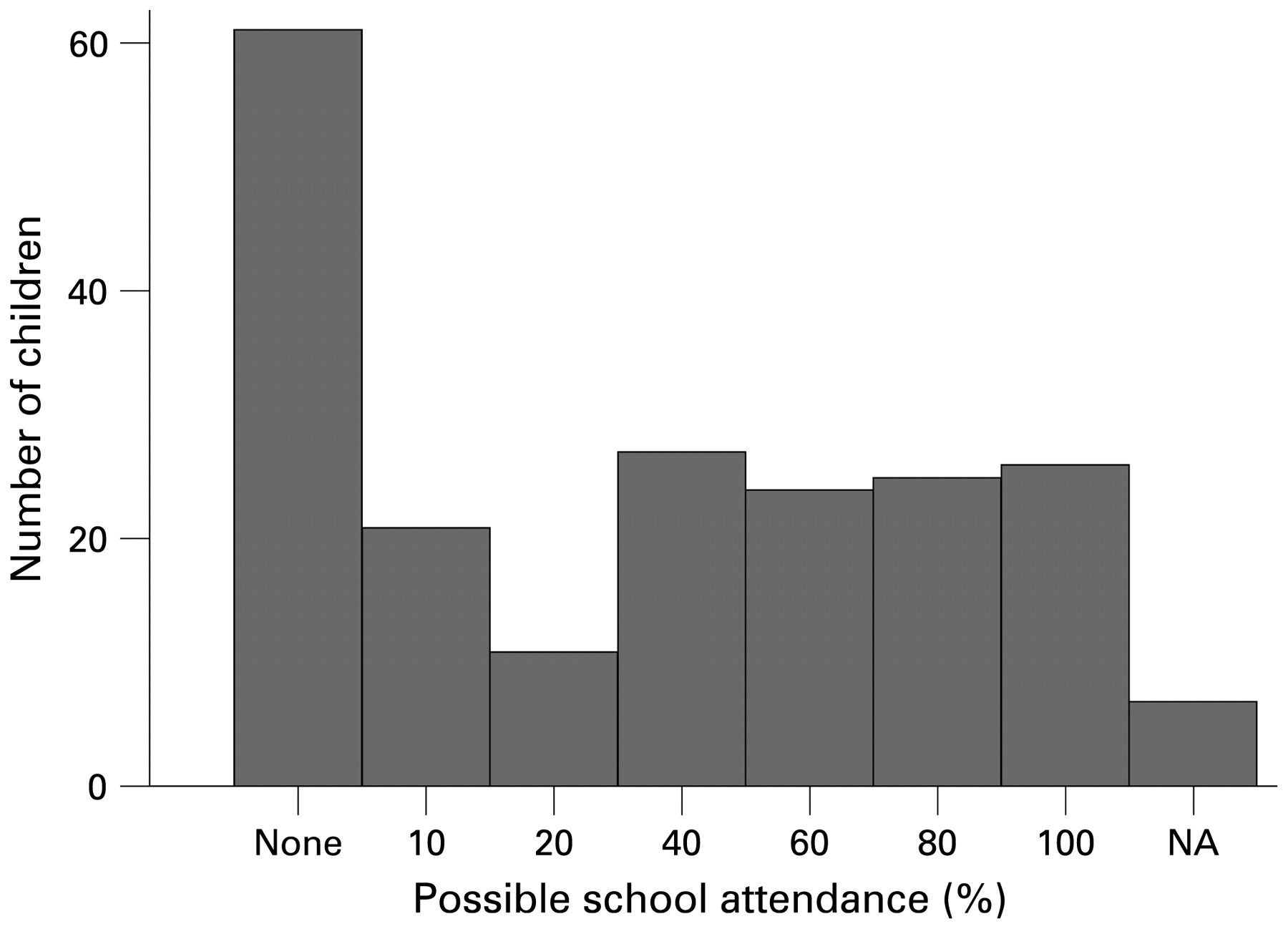
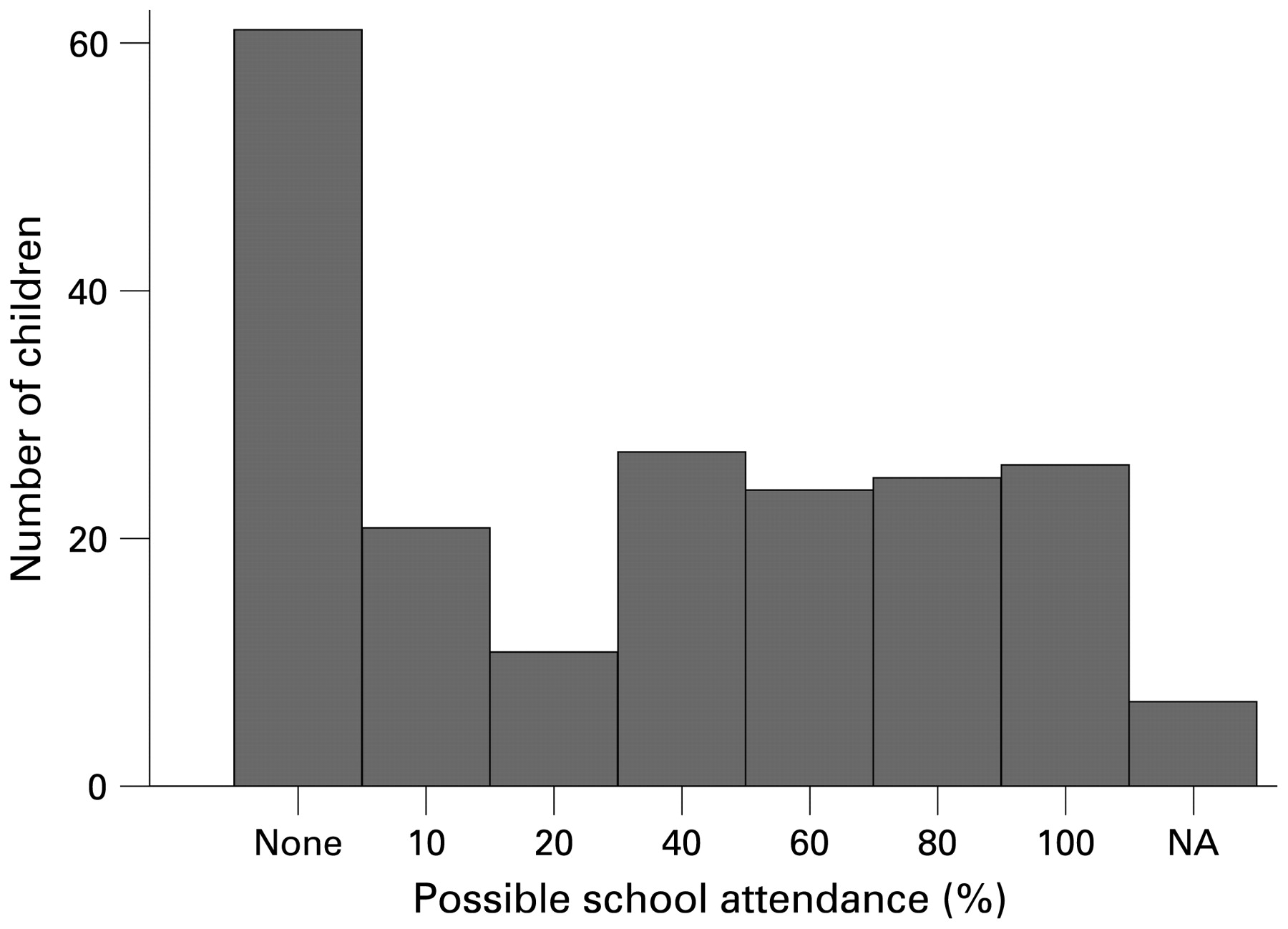
Figure 1 shows the distribution of school attendance. Only 11% of children attended full-time school, whereas 28% were unable to attend school at all. Forty-nine per cent of children attended 20% or less and 62% attended 40% or less. Table 2 shows associations of fatigue, mood and pain with school attendance (dichotomised as ⩽40% or >40%). Among 130 children in whom both the SCAS and other inventories were measured, children with better physical function measured by the SF-36 score were more likely to attend school (adjusted odds ratio (OR) 1.70 per two-unit increase, 95% CI 1.36 to 2.13). There was no evidence that anxiety score measured using the SCAS was associated with school attendance. Associations with total fatigue and pain score were attenuated after adjusting for the other variables. There was no evidence that gender, age at assessment or time from onset of symptoms to assessment in clinic were associated with school attendance.
{kind=link}
Histogram of school attendance (percentage of possible attendance).
OR (95% CI) for the association of fatigue, mood and pain with school attendance (more or less than 20% attendance at school)*
In 80 older children who completed the HADS, reduced physical function measured by the SF-36 was again associated with school attendance (adjusted OR 2.05 per two-unit increase; 95% CI 1.4 to 3.01; p<0.001). In this group, we found no evidence that anxiety score, depression or pain were associated with school attendance after adjusting for the other variables.
Factors associated with physical function
The children and young people in this study had a median SF-36 physical function subscale of 20 (interquartile range 16–23). The lowest possible score is 10, which means “limited a lot” in all areas including activities of daily living such as bathing and dressing. The highest possible score of 30 means “not limited at all”. Ninety-eight per cent of children and young people were limited to some extent in mobility or activities of daily living, according to their SF-36 scores.
Table 3 shows regression coefficients for the association of fatigue, mood and pain with physical function measured by the SF-36. In 136 children in whom both the SCAS and the other inventories were measured there was clear evidence that both increasing fatigue and increasing pain scores were associated with worse physical function, after adjusting for age and sex. An association of physical function with SCAS anxiety was attenuated after adjusting for other variables. In 87 older children in whom HADS anxiety and depression were measured, increasing fatigue, depression and pain were associated with worse physical function. There was no evidence, in either group, that gender, age at assessment, family history or time from onset of symptoms to assessment in clinic were associated with physical function.
Regression coefficients (95% CI) for the association of fatigue, mood and pain with the SF-36 measure of disability*
Discussion
This group of 211 children diagnosed with CFS/ME by a specialist paediatric CFS/ME clinic were severely affected, with nearly a third attending no school at all and over 60% of children attending only 2 days of school or less. Only four children (2%) were not limited in mobility or activities of daily living. The factor most strongly associated with reduced school attendance was poor physical function. Worse physical function was associated with higher levels of fatigue, pain and low mood. We found no evidence that school attendance was associated with anxiety measured either by the SCAS or the HADS. Anxiety was only weakly associated with physical function and this association was attenuated after adjusting for other factors.
Strengths and weaknesses
This is the first study to look at the relationship between school attendance and physical function with fatigue, pain and mood in children and young people with CFS/ME. Data were collected prospectively in a large unselected group of children and young people attending a paediatric CFS/ME clinic with a high response rate to a large number of questionnaires. However, as the study cohort was from a regional specialised service, it is possible that the children described are more severely affected than those attending a general paediatric clinic, and the results may not be generalisable to general paediatric or community services.
In addition, the study used self-completed inventories to measure school attendance, physical function, fatigue and pain. Parents and indeed clinicians may have a different view on the physical ability, fatigue or pain their child experiences and this has not been measured. We did not obtain additional information from schools about school attendance but clinically have found that the young person-completed inventories for school attendance correlate highly with school attendance records.
This study used the RCPCH criteria to make a diagnosis of CFS/ME in children unlike previous studies,2 4 which used adult-defined criteria such as those defined by the CDC. Unlike the CDC criteria, the RCPCH criteria do not require a minimum time for fatigue although recent guidance from NICE recommends a minimum time of 3 months.
What is already known on this topic
CFS/ME in children is common, affecting up to 2% of children aged under 18 years.
Most children with CFS/ME have poor physical function, with up to 57% of children bed-bound at some stage.
The majority of children with CFS/ME miss significant amounts of school.
What this study adds
Children with poor physical function are more likely to have reduced school attendance.
Poor physical function in children with CFS/ME is associated with pain, fatigue and low mood.
There was little evidence of associations between school attendance and either anxiety or fatigue in children with CFS/ME.
Results in context with previous literature
The female to male ratio in this study is consistent with specialist cohorts,11 17 18 but is higher than in population-based studies, in which the number of females and males can be roughly equal.6 7 The children in our cohort were more severely affected than a previous relatively small cohort (29 children),10 in which 14% were normally physically active. This could be because children took longer to present to our specialist service compared with previous studies in which a median time from symptom onset to assessment of 8.5–11 months has been reported.10 17 19 As in other studies10 11 we showed that children with CFS/ME missed a significant amount of school.
In our study nearly 20% of children assessed had a first-degree relative with CFS/ME, which is consistent with other studies describing a high degree of familial aggregation in the families of children with CFS/ME.20 21 22
Previous studies have demonstrated that children with CFS/ME have higher levels of anxiety and depression than unaffected children of similar ages.23 24 However, we found no evidence that anxiety or depression were associated with school attendance. It may be that anxiety and depression are consequences of CFS/ME rather than being characteristics associated with the severity of the condition (in particular school attendance). This is consistent with the only longitudinal study to date, which did not show that childhood or adolescent psychological distress was associated with the risk of lifetime CFS/ME.25 In our cohort the most important factor associated with school attendance was physical function.
We showed that poor physical function, as measured using the SF-36, was associated with low mood measured by the HADS. However, as this is a cross-sectional study, we are unable to determine the direction of causality. A large study conducted in 14 countries suggested that fatigue and depression acted as independent risk factors for each other in adults, emphasising that assumptions should not made about the direction of causality.26
Implications
Paediatricians who see children with CFS/ME should recognise that reduced school attendance is likely to be associated with reduced physical function rather than anxiety. This suggests that efforts to improve school attendance in children with CFS/ME should focus on evidence-based interventions to improve physical function9 particularly concentrating on interventions that are likely to reduce pain and fatigue.
Acknowledgments
The authors would like to thank the young people and their families who took part.
REFERENCES
Footnotes
Funding The Linbury Trust funded this study.
Competing interests Declared. EC is a medical advisor for the Association for Young People with ME (AYME).