Article Text

Abstract
Objective: To develop and evaluate “Families for Health”, a new community based family intervention for childhood obesity.
Design: Programme development, pilot study and evaluation using intention-to-treat analysis.
Setting: Coventry, England.
Participants: 27 overweight or obese children aged 7–13 years (18 girls, 9 boys) and their parents, from 21 families.
Intervention: Families for Health is a 12-week programme with parallel groups for parents and children, addressing parenting, lifestyle change and social and emotional development.
Main outcome measures: Change in baseline BMI z score at the end of the programme (3 months) and 9-month follow-up. Attendance, drop-out, parents’ perception of the programme, child’s quality of life and self-esteem, parental mental health, parent–child relationships and lifestyle changes were also measured.
Results: Attendance rate was 62%, with 18 of the 27 (67%) children completing the programme. For the 22 children with follow-up data (including four who dropped out), BMI z score was reduced by −0.18 (95% CI −0.30 to −0.05) at 3 months and −0.21 (−0.35 to −0.07) at 9 months. Statistically significant improvements were observed in children’s quality of life and lifestyle (reduced sedentary behaviour, increased steps and reduced exposure to unhealthy foods), child–parent relationships and parents’ mental health. Fruit and vegetable consumption, participation in moderate/vigorous exercise and children’s self-esteem did not change significantly. Topics on parenting skills, activity and food were rated as helpful and used with confidence by most parents.
Conclusions: Families for Health is a promising new childhood obesity intervention. Definitive evaluation of its clinical effectiveness by randomised controlled trial is now required.
Statistics from Altmetric.com
The prevalence of obesity in UK children continues to rise and its prevention and management is now a public health priority.1 2 Childhood obesity increases the risk of type 2 diabetes, cardiovascular disease, cancer, and psychosocial problems such as low self-esteem and stigma.3 It predicts adult obesity in 40% to 70% of children, with concomitant risks to adult health.4
A current challenge is how best to manage children who are already obese or overweight. Systematic reviews have reported an inadequate evidence base with no studies from the UK5 and have highlighted the importance of family involvement.6 The UK National Institute for Health and Clinical Excellence concluded that programmes incorporating behavioural treatment alongside physical activity and diet were effective, particularly if parents were given the responsibility for behaviour change.7
Primary research contributing to this field includes a report from Epstein’s group from New York who showed that family based behavioural treatment (FBBT) targeted at the parent and child together was more effective as regards long term weight management than targeting the child alone.8 Golan from Israel compared parents with children as the exclusive agents of change, finding a greater reduction in overweight for the parent group.9 A further randomised controlled trial (RCT) by Israel et al demonstrated that a behavioural programme was more effective when run with a parent training course,10 indicating that parenting skills help to sustain improvement.
These trials, although suggesting that family interventions are effective, were all carried out in clinical settings. There is a lack of evidence on community-based interventions. However, recent UK research on community interventions to manage childhood obesity include pilot studies on the WATCH IT programme from Leeds11 and MEND (mind, exercise, nutrition, Do it!) from London.12
The home environment is important in the aetiology of childhood obesity. Parenting styles and skills have been shown to predict children’s BMI, fruit and vegetable intake, healthier eating, physical activity and sedentary behaviours.13–15 Therefore, it is important for programmes to address parenting skills as well as lifestyle.
The aim of the current project was to develop and pilot a new family based group intervention, “Families for Health”. This differs from other programmes being researched in the UK in its emphasis on parenting, relationship skills and emotional and social development, which may enhance long term sustainability. It is delivered in a community setting, with potential for increased access. The model is one of training local facilitators in order to increase local capacity.
METHODS
Development of the Families for Health programme
The programme was developed to a specification by a practitioner experienced in the development and delivery of parenting programmes and in training facilitators, in conjunction with a multi-disciplinary professional and academic advisory group. It is a 12-week programme involving a 2½ h weekly session, comprising parallel programmes for overweight/obese children aged 7–11 and their parents. Parents and children meet mid-session to share an activity and a healthy snack.
The sessions combine proven elements from parenting programmes, school based emotional development programmes and family lifestyle programmes. Parenting aspects draw on the UK based Family Links Nurturing Programme,16 which has received positive evaluations in qualitative research and “pre-post” evaluation.17 18 Healthy eating components draw on nutritional recommendations in the Balance of good health.19 Parents are encouraged to control the home eating environment and monitor children’s food intake, known to be effective strategies.20 21 Restriction of children’s eating was not employed, as this may lead to weight gain.22 The programme promotes a sustainable healthy approach to family-wide lifestyle change. Further details are given in appendix A.
Piloting of the Families for Health programme
The programme was piloted twice in Coventry at a leisure centre, on Saturday mornings (10 am–12:30 pm) from September to December 2005 and on Monday evenings (5 pm–7:30 pm) from January to March 2006. The parents’ and children’s groups were each led by two facilitators. The programme developer was one of the facilitators for the parents’ groups and other facilitators were recruited from local services and included a health visitor, a school nurse, a school lifestyle worker, a nutritionist and a mental health worker. The facilitators undertook a 3-day training course followed by weekly supervision during the programme, provided by the programme developer.
The sample size was pragmatic, selected to include the experience of a range of different families and to estimate effect sizes for sample size calculations in the design of a subsequent RCT, if indicated. We aimed to recruit 20 families.
Recruitment of families
Families with children aged 7–11 years who were overweight (BMI ⩾91st to 98th centile) or obese (BMI ⩾98th centile) according to UK 1990 BMI reference charts23 were eligible. They were excluded if they did not speak English or if the child had a medical cause of obesity.
Several recruitment strategies were piloted. A range of health professionals were asked to recruit families, and when this strategy failed, press releases were sent from the University of Warwick’s communications office, resulting in articles in local newspapers and radio interviews. In the second pilot two primary schools distributed flyers.
Evaluation design
Process evaluation examined the success of recruitment methods, the type of families recruited, attendance and drop-out. Families who attended at least half of the sessions were considered to have completed the programme. Families who withdrew were asked for their reasons. At the end, parents completed a questionnaire giving their perception of the programme and stated whether they were using their new skills and knowledge confidently (Likert scale, 1–5). “Before and after” evaluation was undertaken to compare quantitative measures at baseline with those at the end of the programme (3 months) and at 9 months’ follow-up.
Measures of overweight
The primary outcome measure was change in the children’s BMI z score from baseline. One investigator (WR) measured weight to the nearest 0.1 kg with Tanita scales (TBF-300MA; Tanita, Yiewsley, UK) and height to the nearest 0.1 cm (Leicester height measure; Child Growth Foundation, London, UK). BMI (weight(kg)/height(m)2) was converted into z scores using the Child Growth Foundation’s programme based on UK 1990 data.23 Waist was measured to the nearest 0.1 cm and translated into z scores.24 Percentage fat was measured by the scales using bio-impedance.
Psycho-social measurements
Children’s quality of life was measured using PedsQL 4.0 for ages 8–12.25 Children completed the 23-item self-report and parents the parent-proxy version. Children’s self-esteem was measured using the 36-item Self-Perception Profile for Children.26 Parents completed the 15-item Child-Parent Relationship Scale27 and the Short Depression-Happiness Scale.28
Eating and activity behaviour
Children completed a 24 h food recall using the Day in the Life Questionnaire to determine portions of fruit and vegetables.29 Parents completed the Family Eating and Activity Questionnaire, with summary scores calculated for activity/inactivity balance, stimulus exposure (eg, unhealthy snacks at home), eating related to hunger, and eating style.30
Children’s physical activity was measured using a 7-day recording with a uniaxial accelerometer with step function (GT1M; ActiGraph, Pensacola, FL). A diary was completed at the same time. Average minutes per day undertaking moderate to vigorous physical activity (MVPA) was calculated using Freedson’s equation,31 using 4 METS as a cut-off. Average daily steps were also calculated. To be included in the analysis, 4 days of monitoring were needed for a reliable measurement.32
Ethics approval
The project was approved by Coventry Research Ethics Committee (NHS) and registered with Coventry Teaching PCT.
Statistical analysis
Binary and categorical data were summarised by frequencies and percentages, and descriptive statistics (means, standard deviations) are given for continuous outcomes. Six families enrolled more than one child. To account for the hierarchical nature of the data induced by family clustering, we fitted linear mixed models with random family effects for differences in scores between both (i) baseline and the end of the programme (3 months) and (ii) baseline and 9-month follow-up. Intention-to-treat analyses are presented for both groups combined. Differences between the two groups (Saturday and Monday) were investigated; results are presented separately where significant differences were identified. We refer to differences as statistically significant when the two-sided p value is smaller than 0.05. Analyses were conducted using SAS v 9.
RESULTS
Recruitment and baseline characteristics
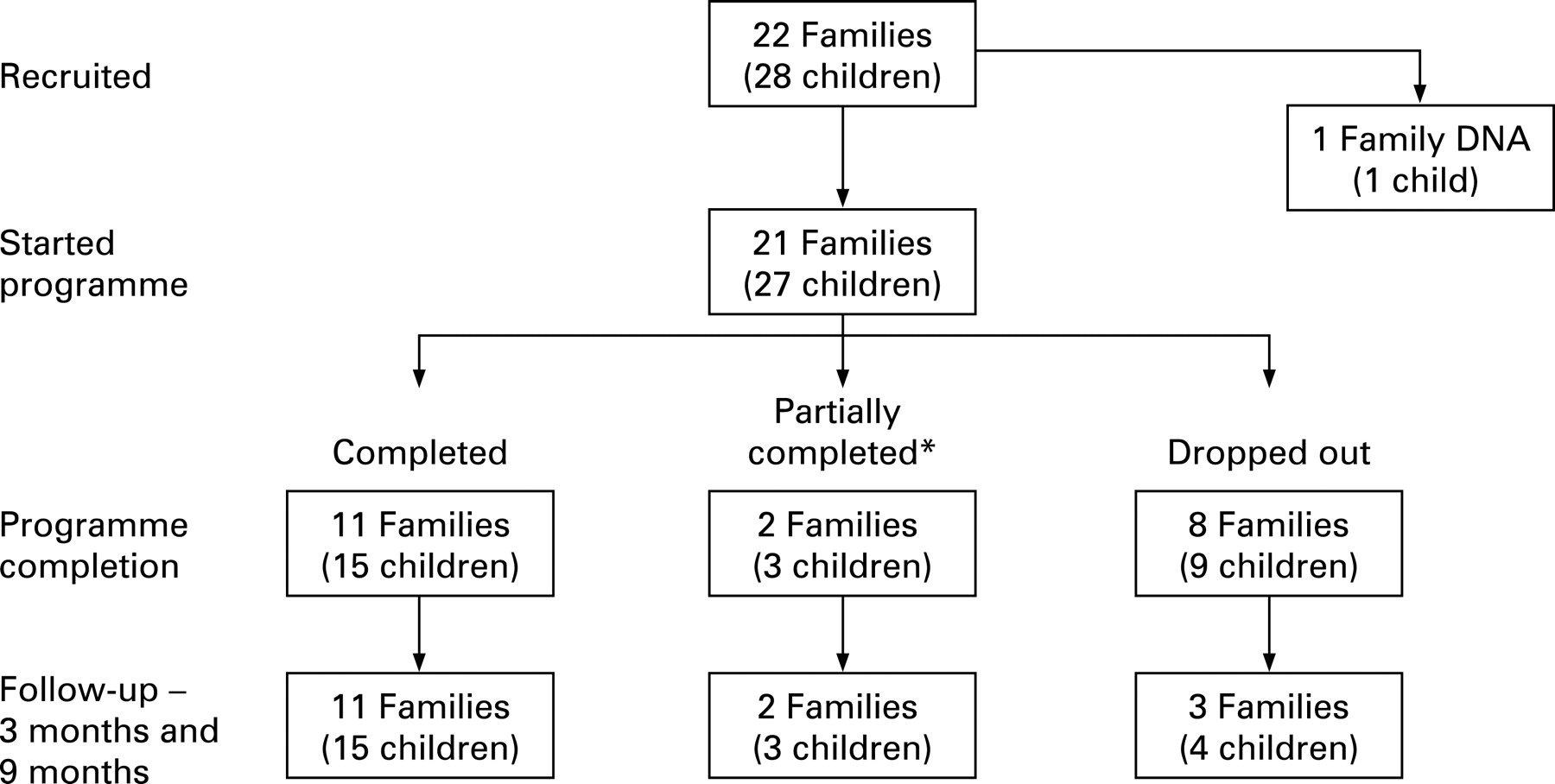
A total of 21 families (27 children) were recruited and started the programme (fig 1). Of these, five families were recruited by health professionals, 13 families self-referred following publicity in the local media, and three came via recommendations from family/friends. No families were recruited through the school flyer.

{kind=link}
Table 1 shows demographic data and baseline BMI for the participants. Two thirds of the children were girls. The ethnic mix was typical of Coventry (84% white in the 2001 Census). Most children were obese, with three overweight children being siblings of obese index children. Three children were above the target age range of 7–11.
Attendance
Attendance was 62%. Of the 27 children who started the programme, 15 (56%) completed, three (11%) partially completed (attended half the sessions, but attended irregularly) and nine (33%) withdrew (fig 1). Four families cited practical reasons for dropping out (new baby, new job, domestic issue, demands of work), one disliked the programme, and three gave no reason.
Engagement with the programme was better on Saturday morning, with 75% attendance and only one family withdrawing. The Monday evening programme achieved only 52% attendance and seven families (eight children) withdrew.
Attrition
We sought follow-up data on all families. Twenty two of the 27 children (from 16 families) contributed data, including four who withdrew (fig 1).
Perception of the programme
Sixteen parents completed the questionnaire. The percentage of parents rating the various components as helpful (scoring 4 or 5) was high for parenting skills (84%), activity (79%) and food (83%). These new skills and knowledge were being applied confidently by 63%, 57% and 73% of parents, respectively.
Change in BMI z scores
The primary outcome, change in BMI z score, was reduced from baseline by −0.18 (95% CI −0.30 to −0.05, p = 0.008) at the end of the 3-month programme. This was maintained at the 9-month follow-up (−0.21, 95% CI −0.35 to −0.07, p = 0.007) (table 2). The fully engaged group (n = 15) showed a slightly greater reduction in BMI z score at 9 months (−0.26, 95% CI −0.40 to −0.12) than overall. Other measures of overweight (waist z score, % body-fat) were also significantly reduced.
Psycho-social measurements
From the parents’ perspective, each aspect of the child’s quality of life improved at 3 months (the end of the programme) but not at 9-month follow-up compared to baseline (table 2). Significant improvements in physical functioning were reported by children at 3 and 9 months, but other aspects of quality of life were unchanged. Children’s self-esteem showed no change for the six domains (table 2). The relationship between parents and children improved significantly at 3 months, although statistical significance was lost by 9 months (table 3). Parents’ mental health improved significantly at both time points.
Lifestyle change
The Family Eating and Activity questionnaire showed that children were significantly less exposed to unhealthy foods in the home (“stimulus exposure”) and had developed an improved eating style; both changes were maintained to 9 months. However, fruit and vegetable consumption had not changed significantly at the end of the programme or at 9 months (table 3).
What is already known on this topic
The most promising interventions outside the UK for the management of obesity in children under age 12 are when parents are given the main responsibility for change.
What this study adds
The Families for Health programme is a promising new childhood obesity intervention which shows benefits in measures of overweight and other health outcomes.
Children became significantly less sedentary at both time points, based on the balance of activity/inactivity reported by parents (table 3).30 This is consistent with the significant increase in average steps per day of children at the 9-month follow-up (table 3). However, the average minutes per day doing MVPA was unchanged (table 3), although the two groups differed in their response. Group 1 reduced their daily MVPA from 71 to 64 min (mean difference −8, 95% CI −22 to 5.9, p = 0.22) from September to December, and group 2 showed a significant increase from 40 to 55 min (mean difference 15.5, 95% CI 0.7 to 30.4, p = 0.042) from January to April.
Completers versus drop-outs
There was no differences in baseline BMI or gender between the 18 children who completed the programme and the nine who withdrew, but there appear to be differences depending on how they were recruited. Only two of the 13 families who self-referred after publicity in the local media withdrew, whereas three of the five families referred by health professionals and all three of the families who enrolled following recommendations by friends/family withdrew.
DISCUSSION
Families for Health differs from other childhood obesity programmes currently being researched in the UK in its emphasis on parenting and relationship skills. It is based in a community setting and the model is one of training local facilitators in order to increase local capacity and sustainability. This pilot study with 21 families suggests that the programme may reduce overweight and improve other health related outcomes.
The programme attracted participants from diverse family types and socio-economic groups. Unpaid publicity in the local media proved to be the most effective recruitment strategy, and families recruited in this way were more likely to complete the programme (self-referral may indicate commitment to change).34 The overall drop-out rate of 33% is within the range for other obesity management interventions.7 Our pilot showed that timing of sessions influenced attendance and completion, with Saturday morning being much better than Monday evening, largely because of the practicalities of attending this 2½ h programme after school. Parents indicated that the programme was helpful, with new skills and knowledge being used confidently.
The achievement of a significant reduction in BMI z score of −0.21 at the 9-month follow-up (6 months after completion of the intervention) is very encouraging. This may underestimate the benefit on obesity as children referred to hospital outpatient clinics may actually increase BMI by 0.2 z score over this timescale.11 Although benefits are difficult to assess without a control group, our results are similar to those of other UK based interventions aimed at this age group, notably MEND which showed a −0.24 difference in BMI z score between randomised groups at a 6-month follow-up.35
Quality of life scores (PedsQL) for the 28 overweight/obese children at baseline of 65.3 (self-report) and 67.7 (parent) are much lower than scores for “healthy” children from Wales (UK) and USA but similar to those for children with chronic diseases and obese children in USA.36 37 It is therefore encouraging that the parent-proxy scores in both physical function and psycho-social health increased significantly at the end of the Families for Health programme. The difference lost statistical significance by 9 months, but the clinical significance of these improvements in quality of life should not be underestimated. Children reported improved physical functioning, which may help engagement in physical activity.
Surprisingly, a review of the literature showed that the association between obesity and self-esteem in children is modest in community samples, although it shows a stronger link in clinical samples.38 Baseline scores for children participating in Families for Health appeared lower than those of Scottish children, at least on the athletic and appearance domains,39 but the programme has shown no change. The validity of Harter’s Self-Perception Profile has been questioned for intervention designs in British children,40 suggesting that further work may need to use an alternative measure.
Improvements on the Family Eating and Activity Questionnaire30 could be attributable to social desirability response bias, with answers from parents reflecting perceived expectations. Interviews with parents, however, validated the questionnaire findings, with some families indicating they had bought dinner tables and had stopped having sweets/snacks in the home.
Changes in activity levels, however, were only partially demonstrated. The inactivity/activity balance on the Golan questionnaire did improve significantly, with children becoming less sedentary.30 Increased step-counts at 9-month follow-up also indicated the success of the programme to encourage 10 000 steps per day. However, minutes of MVPA did not change as a result of Families for Health, although the second group showed a significant increase from baseline in January to the end of the programme in April. This highlights a problem with looking at changes over time. Children are less active in winter,41 and as we did not have a full 12-month follow-up, habitual activity was measured at different times of year, making interpretation difficult. Although MVPA did not change, the two other measures suggest an increase in habitual activity.
The relationship between parents and children improved significantly at the end of the programme, reflecting the emphasis in Families for Health on parenting and relationship skills. Giving parents the main responsibility for the behaviour change in the family is central to the success of the Families for Health pilot and may enhance long term sustainability. This will be examined in a 2-year follow-up.
CONCLUSION
The Families for Health programme is a promising new childhood obesity intervention which has the potential to make a real difference to help families with children who are overweight or obese, impacting on obesity and other health outcomes. This programme warrants further piloting and evaluation in a randomised controlled trial.
Acknowledgments
Thanks to Michelle Oldfield for administrative support; the facilitators, Mandy Coombes, Clair Hobbs, Daksha Myrie, Dawn Swan and Stephen Withers; Coventry Sports and Leisure Centre; and to the families who took part. The materials for this programme were developed by Candida Hunt and the University of Warwick. Candida Hunt developed the training programme, trained children and parent group facilitators and facilitated the parents’ groups. Professor Jane Barlow, Chris Burrows, Dr Laurel Edmunds, Dr Krystyna Matyka, Dr Anita Morgan and Elizabeth Wilcock sat on the Research Advisory Group which provided advice and support for the development of the programme and the evaluation. Dr Moria Golan provided advice on the development of the programme.
Appendix A
Details of the Families for Health programme
Parents’ programme
The approaches used included facilitated discussion, role play, goal setting, skill practice, a solution focused approach rather than a focus on problems, and homework. The topics covered included support with both parenting skills and family lifestyle. Parenting skills topics included giving praise, raising self-esteem, positive discipline, consistently enforced family rules, relationships’ education, emotional health and developing autonomy. Family lifestyle topics included controlling the child’s eating environment to limit exposure to unhealthy foods, making healthy choices available, food labels, portion sizes, family meal times; cooking advice and the opportunity to try new foods; decreasing sedentary behaviour (eg, limiting TV); and increasing sustainable physical activity.
Children’s programme
There were three components. First, information on healthy eating using the Balance of good health,19 and emphasis on food labels, trying new foods and practical food preparation (served at the mid-session break with parents). Second, circle time enabled discussion of the emotional aspects of the children’s lives and of living with obesity, to develop their emotional literacy, raise self-esteem and build confidence. Third, emphasis was given to physical activity aimed at increasing activity levels by participation in games, new physical activities that could be sustained, and the use of pedometers to encourage 10 000 steps per day.
REFERENCES
Footnotes
Funding: The development and piloting of the Families for Health (FFH) programme was funded by a Public Health Initiative award from the Department of Health. Coventry Teaching PCT supported the pilot both practically and financially.
Competing interests: None.
Ethics approval: The project was approved by Coventry Research Ethics Committee (NHS) and registered with Coventry Teaching PCT.
Linked Articles
- Atoms