Article Text

Abstract
Objective: To identify risk factors associated with obesity in primary school children, with a particular focus on those which can be modified. To identify critical periods and growth patterns in the development of childhood obesity.
Methods: 871 New Zealand European children were enrolled in a longitudinal study at birth and data were collected at birth, 1, 3.5 and 7 years of age. Data collected at 7 years included weight, height, bioelectrical impedance analysis (BIA), television viewing time and a 24 h body movement record (actigraphy). The outcome measure was percentage body fat (PBF), which was calculated at 3.5 and 7 years using BIA. Univariate and multiple regression analyses were carried out using PBF as a continuous variable.
Results: Multivariable analysis found maternal overweight/obesity, maternal age, female gender, sedentary activity time and hours of television viewing to be independently associated with PBF at 7 years. Growth variables (birth weight, rapid weight gain in infancy, early (1–3.5 years) and middle childhood (3.5–7 years)) were also independently associated with adiposity at 7 years. There was a strong correlation between PBF at 3.5 years and PBF at 7 years.
Conclusions: Many primary school aged children start on the trajectory of obesity in the preschool years, which suggests interventions need to start early. Maternal overweight/obesity, television watching, sedentary activity time and rapid weight gain in infancy, early and middle childhood are risk factors for childhood obesity, and are all potentially modifiable.
Statistics from Altmetric.com
The prevalence of childhood overweight and obesity has increased by 2–4-fold over the past two decades in developed countries.1 Such a dramatic increase in prevalence suggests environmental factors are very important as the cause of this “obesity epidemic”. Obese children and adolescents can develop serious chronic disease sequelae, including type 2 diabetes and metabolic syndrome.1 2 Obesity often persists into adulthood and is associated with increased morbidity and mortality.3 4
International studies that have investigated risk factors for childhood obesity have mainly been cross-sectional, have often been underpowered, have often inadequately accounted for confounding variables, have not investigated multiple potential factors simultaneously and have not used objective measures.5 As a result the evidence that links risk factors to childhood obesity is often weak, although there is increasing evidence that the environment in early life is important.6–9
The aim of this study was to determine the biological, maternal, socio-economic and environmental factors associated with overweight and obesity in New Zealand 7-year-old children, with particular emphasis on the modifiable factors to guide prevention strategies. As a longitudinal cohort study with prospectively collected data, it provides more robust evidence of causation of the determined risk factors.
METHODS
Subjects
The Auckland Birthweight Collaborative (ABC) study, which has been described in more detail previously, was designed as a case–control study to determine risk factors for small for gestational age (SGA) infants.10 Between 16 October 1995 and 12 August 1996, babies born and resident in the Waitemata Health or Auckland Healthcare regions were eligible for inclusion and from 12 August 1996 to 30 November 1997, babies born and resident in the Auckland Healthcare region were eligible for inclusion. Preterm infants (<37 completed weeks of gestation), multiple births and those with congenital abnormalities were excluded. The sample was selected disproportionately to include all infants born at term and SGA (⩽10th percentile for sex and gestation for New Zealand)11 and a random sample of appropriate for gestational age (AGA) infants (>10th percentile for sex and gestation). The AGA infants were randomly sampled at a rate of 1 in 16 during the first period of the study and this was increased to 1 in 8 in the second period when only the Auckland healthcare region was involved.
Variables/data collection
Phase 1 (birth data)
Women were interviewed during the week following delivery and obstetric records were reviewed. Variables from this phase included self-recalled maternal weight before pregnancy and height (from which maternal body mass index (BMI) was derived), maternal age, socio-economic information, smoking in pregnancy and hypertension in pregnancy.
Phase 2 (12-month data)
Parents completed a postal questionnaire when the infant was 1 year of age. Data collected included the duration of breast feeding. Growth information from the child’s well-child health book (a parent-held record of a child’s health, growth and development) was also extracted by the parent.
Phase 3 (3.5-year data)
Children attended the Children’s Research Centre (CRC) at Starship Children’s Hospital, Auckland, when they were between 3.5 and 4 years of age. The assessment included data on growth and body composition.
Phase 4 (7-year data)
Most children attended the CRC at 7 years of age for assessment of growth and body composition, while 92 children (15.6%) were visited at home.
Activity record
A 24-h physical activity record (actigraphy) was collected to objectively measure levels of physical activity. Children wore a MTI accelerometer around their waist, positioned on the right hand side, for the day before their follow-up appointment. The activity variables estimated were total physical activity counts, mean activity counts and minutes of sedentary, moderate and vigorous activity,12 which correspond to <3 metabolic equivalent tasks (METs; equivalent to sitting), 3–5.9 METs (walking) and ⩾6 METs (running), respectively.13
Growth variables
Growth measurements (height (length for ages under 1 year) and weight) were collected at all phases of the study. Due to the timing of routine well-child health visits by community child health nurses, the best measurement of early growth was at around 9 months of age.
Height (length) and weight measurements were available at birth and at approximately 9 months, 3.5–4 years and 7–8 years of age. These measurements were then converted to standard deviation scores (SDS) using the LMS models produced for British children.14 To determine growth rates for each of the growth periods, the change in SDS was divided by the time interval between the measurements (as it varied between children) to give change in SDS/month. These growth rates were then categorised into quarters for analysis, with the highest quarter representing the children who had the greatest change in SDS/month or upward centile crossing.
Outcome measure
Weight was measured in 0.1 kg increments on a single set of electronic scales that were regularly calibrated (Tanita, Tokyo, Japan), and height was the average of three measurements taken using a stadiometer (Pharmacia Upjohn, London, UK) that was fixed to the wall.
Bioelectrical impedance analysis (BIA) was performed to assess body composition using a BIM4 machine (Impedimed, Brisbane, Australia). The equation used to calculate fat free mass (FFM) was: FFM = 0.65(height2/impedance)+0.68×Age+0.15.15 Percentage body fat (PBF) was the outcome measure analysed in this paper. PBF was calculated using (weight−FFM)/weight×100).
Statistical analysis
Analysis of PBF was carried out in Proc Surveyreg in SAS v9.1. The SURVEYREG procedure performs regression analysis for sample survey data. This procedure can handle complex survey sample designs, including designs with stratification, clustering and unequal weighting. This procedure was used with appropriate weighting to allow for the disproportionate sampling of the SGA infants in the original sampling. Univariable and multiple regression techniques used PBF as continuous variables. A multivariable model was fitted including variables identified as significant at the 10% level in univariate analysis. Non-significant variables were removed in a stepwise manner.
A second multivariable model was fitted using the variables from the first multivariable model, and then those variables associated with growth were added. This was done because approximately 20% of growth measurements were missing at various time points.
Ethical approval
Ethical approval was obtained from the local ethics committee.
RESULTS
Subjects
Participation rates for non-European ethnic groups were poor so analysis was restricted to European children. A total of 871 infants were born to mothers who identified themselves as European, of whom 385 (44.2%) were SGA and 486 were AGA.10 Of the 871 European babies enrolled at birth, 744 (85.4%) participated at 1 year, 550 (63.2%) at 3.5 years and 591 (67.9%) at 7 years of age. There were 241 (40.8%) participants at 7 years of age who were born SGA and 350 who were born AGA.
The mean ages at which growth measurements were taken were 8.7 months (interquartile range (IQR) 8.4–9.5) for the 9-month data, 3.9 years (IQR 3.8–3.9) for the 3.5-year follow-up, and 7.3 years (IQR 7.2–7.3) for the 7-year follow-up. Table 1 gives the characteristics of the participants at 7 years of age.
Measures of obesity and their distribution
The rates of overweight and obesity at 7 years of age, using internationally recognised gender and age specific BMI cut-offs, were 15.3% and 7.6%, respectively.16
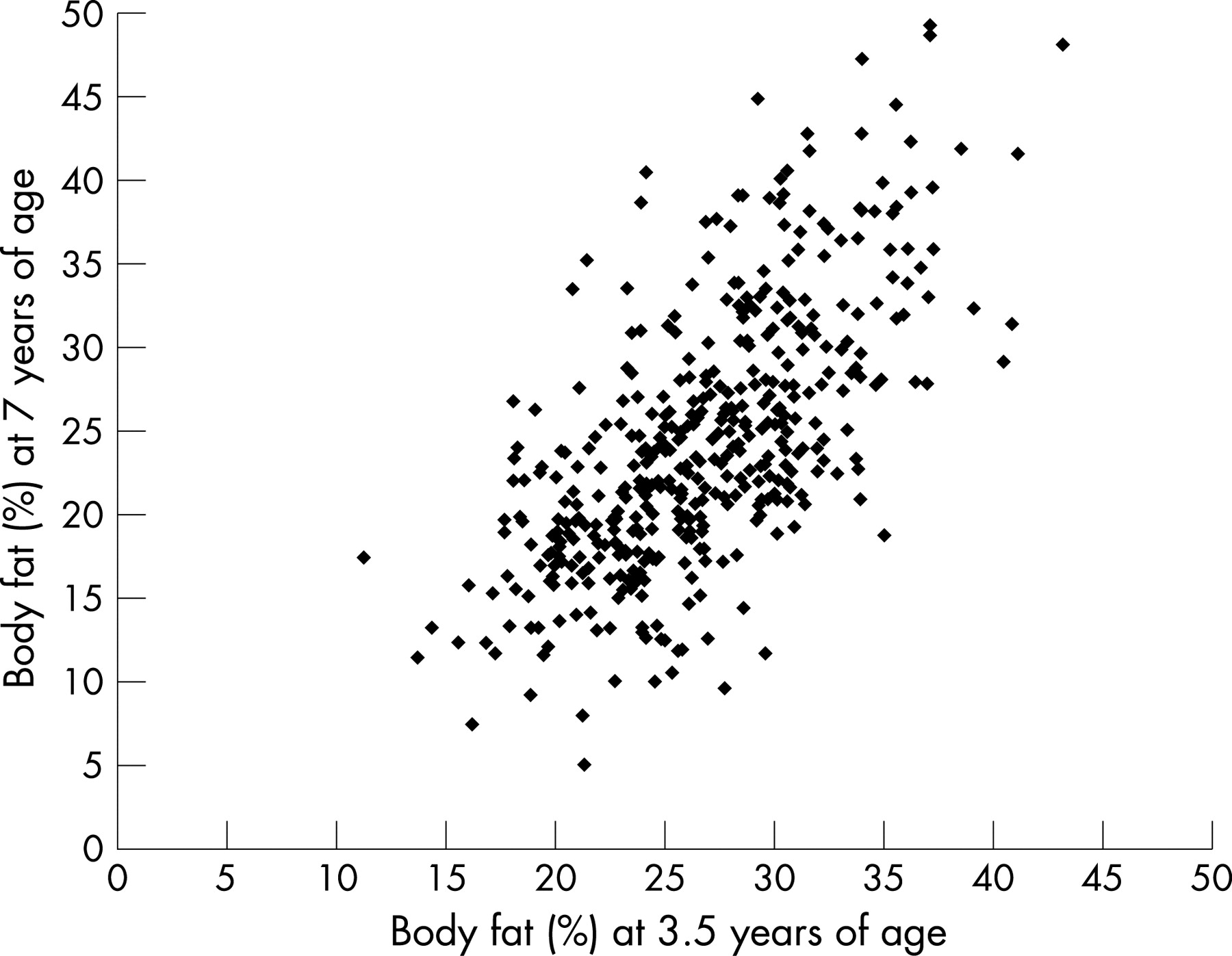
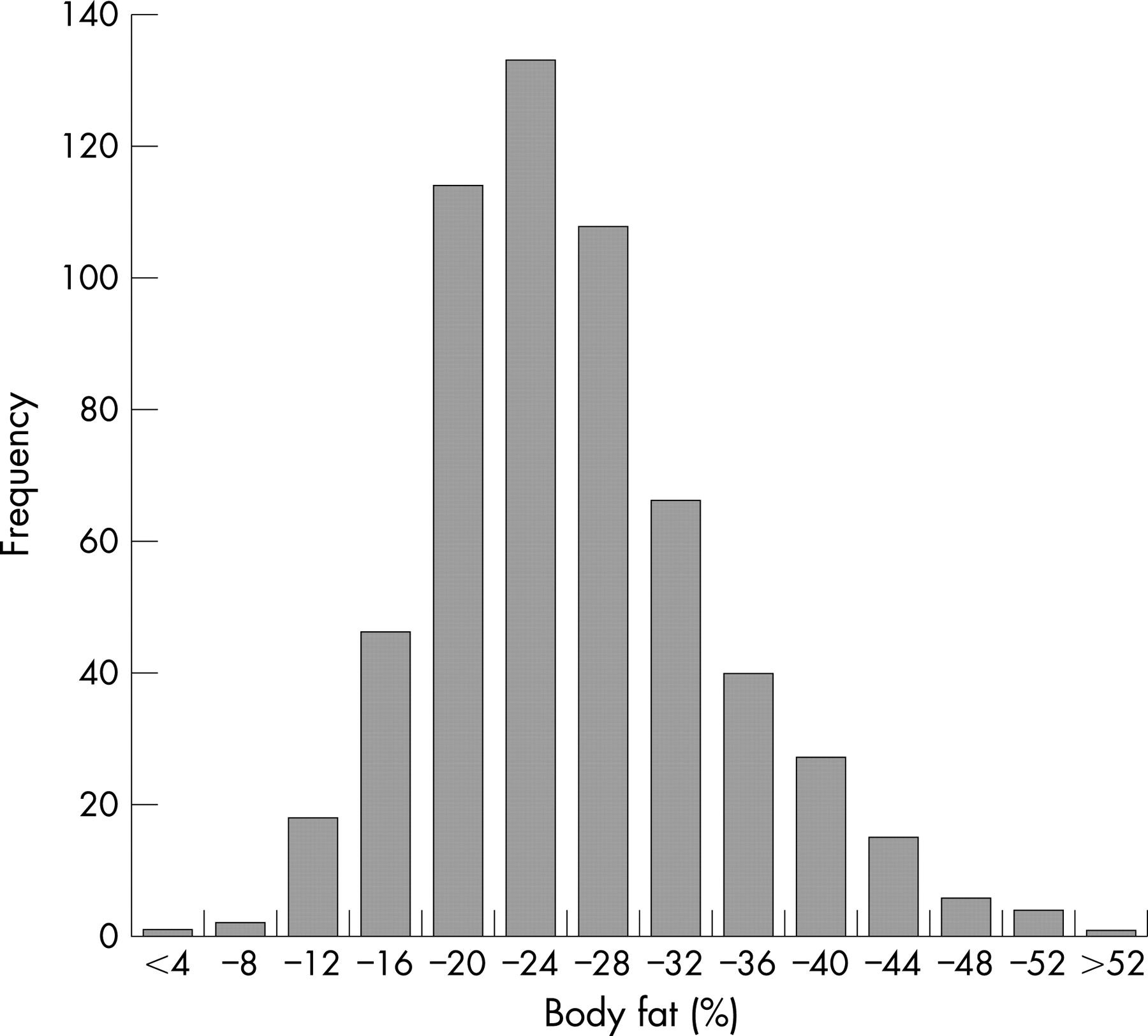
Figure 1 shows the distribution of PBF at 7 years of age with an average PBF of 24.5% (standard deviation 7.9). Girls had 1.8% (95% CI 0.2% to 3.4%) higher PBF compared with boys. The correlation between BMI and PBF at 3.5 years was 0.62 and this increased to 0.78 at 7 years. There was a strong correlation between PBF at 3.5 and 7 years (r = 0.67, p<0.001) (fig 2).

{kind=link}
{kind=link}
Risk factors associated with PBF at 7 years
Children born SGA had significantly lower PBF at 3.5 years (25.5% vs 27.6%, p<0.001) and at 7 years (23.3% vs 25.3%, p = 0.0032) compared with those born AGA. Further analyses took into account the disproportionate sampling of SGA in the original sample.
Variables that were not associated with PBF were smoking in pregnancy, measures of socio-economic status, breast feeding, moderate activity, and mean and total activity counts.
In multivariate analysis, the variables that remained significantly associated with PBF were maternal BMI, maternal age, female gender, hours of television viewing and sedentary activity (table 2). Although maternal age remained significant in the multivariate analysis, a consistent relationship between maternal age and PBF was not seen.
Children with overweight mothers (BMI 25–30) had 3.7% more body fat, and children with obese mothers (BMI>30) had 4.0% more body fat compared with those born to mothers who were not overweight or obese. Compared with children who watched less than 1 h of television per day, children who watched more than 3 h/day had 5.2% more body fat and those who watched 1–3 h/day had 2.5% more body fat. For every additional hour of sedentary activity during waking hours children had 0.8% more body fat.
Birth weight and changes in weight SDS were associated with PBF at the univariate level and continued to show independent effects on PBF in the multivariate model (table 3). Birth weight grouped in 500 g intervals showed a positive association between body fat and birth weight, with a nearly 9% difference in PBF between those babies born below 2500 g and those born at more than 4000 g. All three growth intervals (birth to 9 months, 9 months to 3.5 years, and 3.5 to 7 years) showed increased amounts of body fat with the higher quarters of change in weight SDS per month. For each of the time periods, compared with the bottom quarter those in the top quarters of growth had similar size increases in PBF of between 6% and 7%.
In terms of growth related to height, the only effect in the multivariate analysis was with height change from 9 months to 3.5 years of age. This effect was limited to the top versus the bottom quarter (4.7%, 95% CI 1.9 to 7.4).
DISCUSSION
This study prospectively collected a wide range of data relating to maternal, socio-economic, infant, growth and lifestyle factors, which were then analysed as determinants of PBF at 7 years. Other strengths of this study were the use of BIA to accurately determine adiposity (PBF) rather than BMI, a surrogate measure of body fatness, and the use of accelerometers to objectively assess physical activity.
Five risk factors for childhood adiposity were identified: maternal overweight/obesity, maternal age, female gender, time spent watching television and time spent in sedentary activity. Of the growth variables, birth weight, rapid growth (change in weight SDS) in infancy, between 9 months and 3.5 years and between 3.5 and 7 years, and rapid linear growth (change in height SDS) between 9 months and 3.5 years were all positively associated with PBF at 7 years.
The rates of obesity and overweight at 7 years observed in this study were comparable to those reported in the recent New Zealand National Survey 2002 for 7–10-year-old children of European descent.17
Our finding that the correlation between PBF and BMI increases with age, suggests that BMI is a better proxy of adiposity in older children than in preschoolers. This has important implications for the use of BMI in clinical practice given it is currently more easily determined and its wider use.
Tracking of obesity through childhood into adulthood is well established.14 18 Our finding that PBF at 3.5 years is strongly related to PBF at 7 years provides further evidence that many start on the trajectory to overweight and obesity early in life and that interventions also need to start early.
The finding that maternal overweight/obesity significantly increases the risk of childhood obesity has been consistently reported in other studies.4 5 7 18 19 Whether this association is a result of genetic mechanisms, intra-uterine influences or shared family lifestyle factors or a combination of these mechanisms needs further elucidation.5 19
Breast feeding is reported to be protective against obesity.9 Our study did not find an association between breast feeding and PBF at 7 years. However, there were high breastfeeding rates in this study (with 97% initiating breast feeding) and in New Zealand in general, which reduces the ability to detect a small protective effect.20
Duration of television viewing was found to be a strong predictor of body fatness, supporting the findings of earlier studies. The positive association between television watching and BMI measured at 5–15 years has been found to be long lasting; television watching in childhood and adolescence were positively associated with BMI at 26 years of age.21 Several possible mechanisms by which television watching could contribute to the development of obesity have been investigated, including reduction of resting metabolic rate, reduction in physical activity, exposure to television advertisements and poor diet.22 Our finding that time spent in sedentary activity and television viewing, one of the main sedentary activities, are both independently associated with PBF, is testimony to how important sedentary behaviours are in the aetiology of obesity. In contrast, a recent study has suggested an inverse relationship between moderate and vigorous activity and obesity.23
The finding of increased body fatness with increased birth weight is consistent with the body of evidence from international studies.5 19 A strong association between rapid early weight gain and later obesity or adiposity has been consistently found, as shown in a recent systematic review of 13 studies.6 Our study is the first to examine and compare growth at several stages of early childhood; we found that each of the three growth periods (postnatal, early childhood and middle childhood) were equally critical in the development of obesity at 7 years.
Within our sample, children born SGA were more likely to be in the higher quartiles for postnatal growth, presumably reflecting “catch-up growth”. Ong et al also reported that infants of low birth weight, particularly those who were growth restricted in utero, are at increased risk of rapid postnatal weight gain, later obesity and disease in adulthood.8 24 Previously, catch-up growth has been viewed as a healthy response whereby children who were growth restricted in utero grow rapidly in the first 1–2 years of life and thus return to their genetic trajectory.8 25 However, given the growing evidence linking rapid postnatal growth with later obesity and adverse health in adulthood, this previously promoted growth pattern needs to be re-examined.6 26 27 SGA, as well as AGA, infants may be better off in later life if they grow more slowly, proportionately or along the percentile on which they were born.
What is already known on this topic
The obesity epidemic includes children.
Watching television and sedentary activity have been implicated in obesity.
What this study adds
Many primary school-aged children start on the trajectory of obesity in the preschool years.
Maternal overweight/obesity, television watching, sedentary activity time and rapid weight gain in infancy, early and middle childhood are independent risk factors for childhood obesity.
Early adiposity rebound occurring before 5–5.5 years of age has been found to predict greater adiposity in adolescence and adulthood.19 28 29 More recently, this association has been thought to occur because early adiposity rebound identifies those children who have high body fatness or are upwards centile crossing.6 30
Measuring the level of physical activity in childhood is notoriously difficult.31–34 However, of the variety of methods available, accelerometers have been well validated in children.35–37 The duration of monitoring used in studies varies but generally the longer the duration the more accurate the estimate.30 37 In this phase of the study activity monitors were worn for 24 h, hence potentially limiting the accuracy of the activity data. Despite this limitation, sedentary activity was still found to be significantly associated with adiposity.
It is acknowledged that diet could potentially confound or mediate some of the reported findings. We will report the influence of diet on obesity in a future publication.
CONCLUSIONS
This study has provided robust longitudinal evidence of important modifiable risk factors in the development of overweight and obesity in 7-year-old children. The important modifiable risk factors identified are maternal BMI, TV watching, increased sedentary activity time and rapid weight gain in infancy, early and middle childhood. Population strategies to mitigate these risk factors should be included in a comprehensive approach to paediatric obesity prevention and management. As there is clearly no single critical period for the development of childhood obesity, a life-course approach to interventions is needed.
Acknowledgments
We sincerely thank the parents and children for participating in these studies.
REFERENCES
Footnotes
The initial study was funded by the Health Research Council of New Zealand. The 12-month postal questionnaire was funded by Hawkes Bay Medical Research Foundation. The 3.5-year follow-up study was funded by the Child Health Research Foundation, Becroft Foundation and Auckland Medical Research Foundation. The 7-year follow-up study was funded by the Child Health Research Foundation. The 3.5- and 7-year follow-up studies were conducted in the Children’s Research Centre which is supported in part by the Starship Foundation and Auckland District Health Board. EA Mitchell and JMD Thompson are supported by the Child Health Research Foundation.
Competing interests: None.
- Abbreviations:
- AGA
- appropriate for gestational age
- BIA
- bioelectrical impedance analysis
- BMI
- body mass index
- CI
- confidence interval
- CRC
- Children’s Research Centre
- FFM
- fat free mass
- IQR
- interquartile range
- MET
- metabolic equivalent task
- PBF
- percentage body fat
- SDS
- standard deviation score
- SGA
- small for gestational age
Linked Articles
- Précis
- Atoms