Article Text

Abstract
Objective To develop a detailed understanding of the circumstances of sudden unexpected death in infancy (SUDI) cases subject to serious case review (SCR).
Design This was a thematic analysis of SCRs relating to cases of SUDI in England. SCRs were obtained for SUDI cases dying between 1 April 2011 and 31 March 2014. These were cases (aged 0–2 years) that presented as a SUDI and for which no clear medical or forensic cause of death was found.
Results SCRs were held for 30 SUDI cases, published reports were available for 27/30. The median (range) age at death was 2 (0–19) months. Background risk factors in families included: alcohol or drug dependency in 18/27, parental mental health problems in 14/27, domestic abuse in 9/27 and parental criminal records in 13/27. Nineteen infants had received support from social care, 10/19 were subject to child protection plans. Neglect was a feature in 15/27 cases. Parents did not engage with professionals in 18/27 cases, involving social care in 14/18, health care in 13/18 and drug and substance misuse services in 5/18. Eighteen of 27 deaths occurred in highly hazardous sleep environments, 16/18 involved cosleeping and 13/16 cosleeping deaths occurred with parents who were intoxicated with alcohol or impaired by drugs.
Conclusion Most SUDI cases occurred in hazardous sleep environments and are potentially preventable. They occurred in families well known to services with concerns about neglect, substance misuse and poor engagement. More consideration is needed on how best to support such vulnerable families.
- child abuse
- SIDS
Statistics from Altmetric.com
What is already known on this topic?
Sudden unexpected death in infancy (SUDI) occurs more commonly in socially deprived families.
Child protection concerns are a well-known but relatively rare occurrence in SUDI investigations.
The risk of SUDI is greatly increased when an infant shares a sleep surface with an adult who has consumed alcohol or drugs.
What this study adds?
Sudden unexpected death in infancy (SUDI) cases subject to serious case review (SCR) occur in families with domestic violence, mental health problems, and substance misuse, with established patterns of non-engagement with professionals.
Most SUDI cases subject to SCR occurred in highly hazardous sleep environments involving intoxicated parents sharing sleep surfaces with young infants.
SUDI cases subject to SCR often happened following a sudden change in family circumstances.
Introduction
Sudden unexpected death in infancy (SUDI) remains a significant problem with around 300–400 SUDI cases annually in England and Wales.1 SUDI is defined as the sudden and unexplained death of an infant that had not been considered as a reasonable possibility in the previous 48 hours.2 The cause of death remains unexplained in approximately two-thirds of SUDI cases and these are often categorised as sudden infant death syndrome (SIDS).3 Potentially modifiable risk factors for SIDS are well established including parental smoking, prone or side sleeping, and cosleeping with a parent who has consumed alcohol or drugs.4 SIDS has declined dramatically since the 1990s following safe sleep campaigns and now occurs largely in association with social deprivation and modifiable risk factors.5 Since 2008, all SUDI cases in England and Wales should be investigated jointly by police, health and social care.6 This process is described in box 1.
The joint agency investigation of sudden unexpected death in infancy
The joint agency investigation of sudden unexpected death in infancy (SUDI) consists of taking the deceased infant to an emergency department, a paediatrician and police officer taking a detailed medical history and account of events from the parents, a joint home visit by police and paediatrician when they examine the death scene, detailed postmortem examination and follow-up for the parents. There is interagency communication throughout the process with an initial information sharing meeting held shortly after the death and a final case discussion at the conclusion of investigations to attempt to agree the full causes of death.
In England, a multiagency enquiry called a serious case review (SCR) is carried out by the local authority where a child has died and abuse or neglect is known or suspected.6 As child protection concerns are not unusual in families with SUDI, occurring in up to 10% of deaths,7 SCRs may take place following SUDI, even though the cause of death may be considered natural.
Further details concerning SCRs are given in box 2.
Serious case reviews
Serious case reviews (SCRs) are to improve the way professionals and agencies work individually and collectively to safeguard and promote the welfare of children. The central focus of any SCR should be on the children’s experiences. SCRs are not enquiries into how a child was harmed or died, or who was responsible; these issues are for police and coroners. SCRs do not form part of disciplinary processes concerning individual professional practice.
An SCR is usually held if a child subject to a child protection plan (CPP) dies unexpectedly, although most SCRs concern children not subject to CPP. In 2013, there were 43 100 children in England and Wales subject to child protection plans,17 of whom 41 died, accounting for 1% of all child deaths and less than 0.1% of all children on CPPs.18
Although there is national analysis of SCRs, there has not yet been an attempt to study SCRs purely relating to SUDI. Given the strong association between social deprivation, unsafe sleep environments and SUDI, an analysis of SCR SUDI cases could provide new insights into the challenging family circumstances where many SUDI cases now occur, and lead to new ways of working with vulnerable families to reduce the incidence of SUDI in the future.
The aim of this study was to analyse the parental backgrounds, parenting behaviours and circumstances of death in SUDI cases that led to an SCR. The research questions were:
In SUDI cases leading to a SCR,
What background parental factors and parenting behaviours may have contributed to death?
What were the circumstances of death?
What was the rationale for holding the SCR?
Methods
As part of a wider national analysis of SCRs,8 the Department for Education (DfE) provided us with a complete list of all SCRs arising from any incident of serious harm or death occurring between 2011 and 2014 in England. Local Safeguarding Children Boards (LSCB) must notify DfE of any incident potentially requiring SCR. DfE, as the lead department for safeguarding children, maintains a database of all SCRs; SCR reports may be obtained from LSCB websites or the National Society for the Prevention of Cruelty to Children (NSPCC) national case review repository. We attempted to obtain all completed SCRs from the NSPCC repository or individual LSCBs. All SCRs were read and those relating to SUDI were identified for inclusion.
We analysed the SCRs using thematic analysis9 assisted by NVivo V.11 software. First, JJG read all 27 SCRs completely and noted ideas for coding. She then read again and coded 15 SCRs, developing the codes iteratively rather than in advance. The codes were then reviewed and refined jointly by both researchers. JJG then coded the remaining SCRs using the revised coding structure. For each code, the entire data set was checked to ensure consistency, and codes were revised and merged. Both researchers together assembled the codes into themes to answer the research questions. We analysed all SCRs continuing beyond the point of theoretical saturation which we defined as the point when few new data emerged relating to the research questions.
We included SCRs relating to infants aged under 2 years at death, whose deaths presented as SUDI, and remained unexplained despite complete investigation. Deaths occurred between 1 April 2011 and 31 March 2014.
JJG and PS are both academic community paediatricians, with clinical and research experience of managing SUDI and child protection cases.
Ethics
As this research involved secondary analysis of publicly available data, ethical approval was not required.
Results
Twenty-seven SUDI SCRs were identified from our reading of SCRs; there were a further three cases recorded on the DfE database for which no published reports were available. All 27 were included in the analysis but 6/27 were published as executive summaries with only limited information. There were 725 unexplained infant deaths in England and Wales during the years 2011–2013,10 therefore approximately 4% of unexplained SUDI cases were subject to SCR.
The median age at death was 2 months (range 0–19), nine infants were male.
Three main themes arose from the qualitative analysis: background parental factors, parenting behaviour directly contributing to death and the circumstances of death. The relationship between codes and themes is illustrated in figure 1. Illustrative quotes are shown in table 1.

Relationship between codes and themes.
Illustrative quotes from serious case reviews
Background parental factors
In 17/27 cases parents were in a relationship with each other at the time of death; further details are shown in figure 2.

Parents’ relationship status at time of death.
Most families had challenging backgrounds. Alcohol or drug misuse by parents occurred in 18 cases, mental health problems in 14 and both in 7. These are shown in more detail in table 2.
Frequency of background parental factors
Involvement with social care
Nineteen families were receiving support from social care at the time of the death with 10 infants subject to child protection plans. Further details are shown in table 3.
Details of social care involvement at time of death
In six families, older siblings had previously been subject to child protection plans, and in nine families legal proceedings to remove children had been considered or were under way.
Reluctance to engage with professionals
Eighteen families were reluctant to engage with services, with disguised compliance where parents gave the appearance of cooperating with professionals to avoid raising suspicion and minimise concerns, a feature of 5/18. Further details are shown in figure 3.
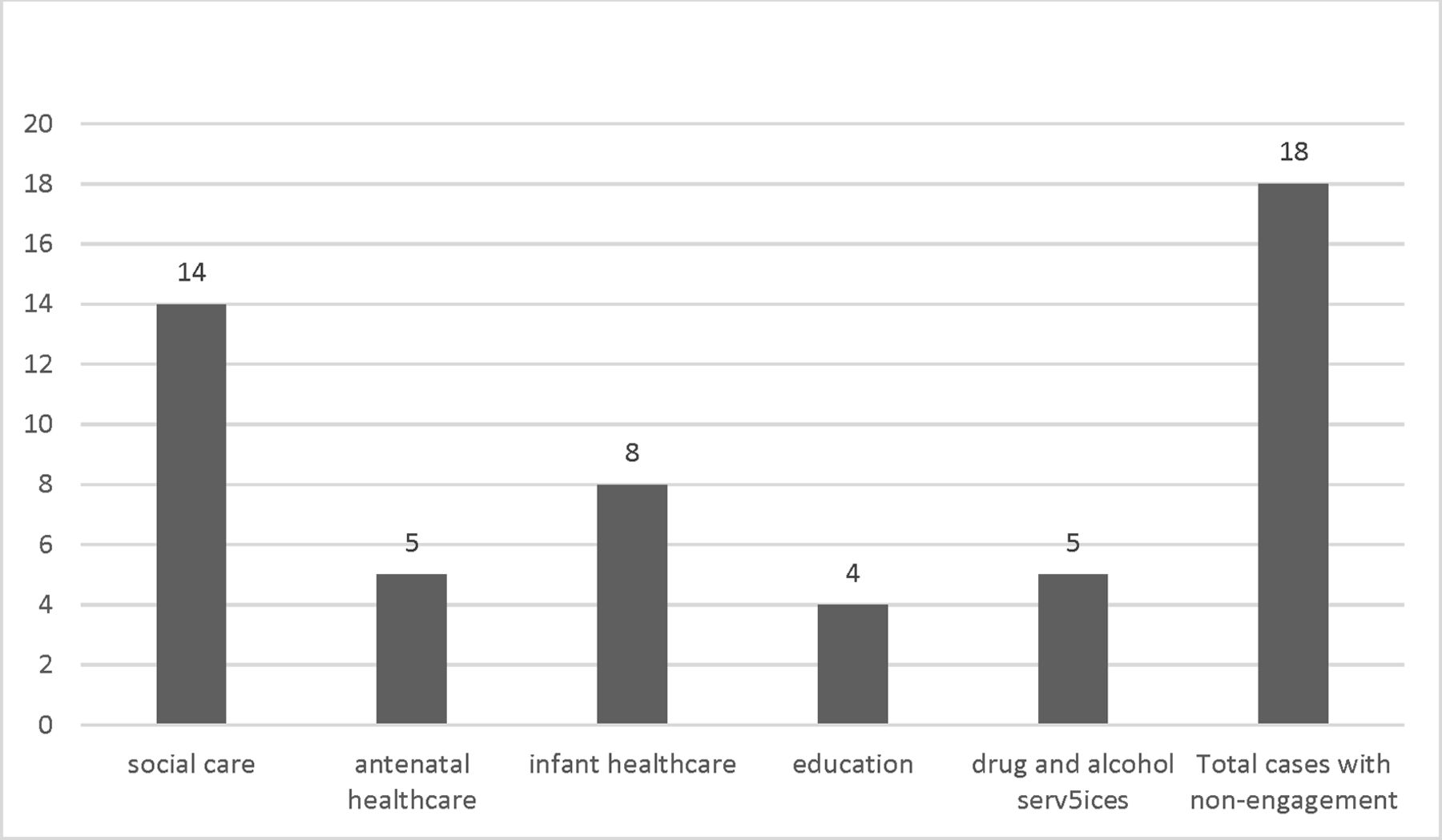
Frequency of non-engagement with services.
Parenting behaviours contributing towards deaths
Neglect
Long-standing neglect was a prominent feature in 15 cases. In 11 families siblings were reported as dirty, hungry, inadequately dressed or had severe dental caries, and seven families lived in homes described as squalid. Four mothers lacked basic parenting skills, and one father was convicted for child neglect after leaving his young children home alone.
In one case, neglect was only noted after the death when the home was found to be in an appalling condition; however, no concerns were noted in a routine visit 2 weeks previously.
Alcohol and drug misuse
In 19/27 cases alcohol or drug misuse was directly involved in the final events, and 15 parents were previously known to have issues with alcohol or drug misuse.
Safe sleep advice
Safe sleep advice shared with parents was documented in 13/27 cases. Three mothers commented that they ignored the advice as they thought ‘it couldn’t happen to me’, these deaths occurred cosleeping with intoxicated parents.
Circumstances of death
The circumstances of death are shown in table 4.
Circumstances of death
Hazardous sleep environments
Sixteen deaths occurred when parents coslept with infants, 13/16 in association with parental drug misuse or alcohol intoxication. Only five infants were found in non-hazardous sleep environments either in cots or Moses baskets.
Unplanned final events
In nine cases there were unexpected changes in family circumstances immediately prior to the death. Three infants were on child protection plans limiting paternal contact due to domestic violence, all died in their fathers’ care, one possibly due to non-accidental injury (NAI). Another infant died in mother’s sole care despite a child protection plan requiring father to supervise all maternal contacts. Two newborn infants died cosleeping with both parents after their fathers had just moved in with their mothers; one had just been returned to parents by the Court.
In three cases, infants died in unplanned cosleeping situations away from home.
Rationale for holding an SCR
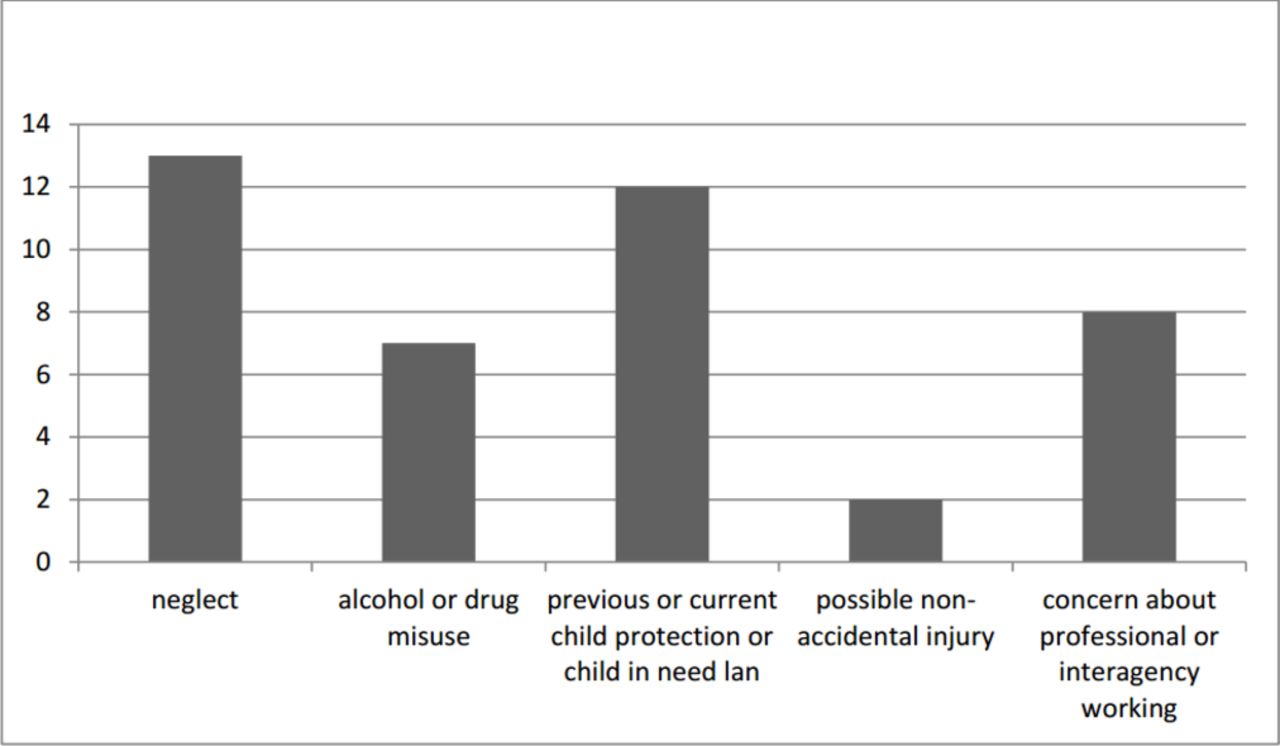
In 14 cases the rationale for holding an SCR was detailed clearly in the report; in the remainder it was implied in the descriptions of the circumstances of death. The reasons given are shown in figure 4.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Reasons stated for conducting serious case review (SCR).
In two cases, there were significant injuries suggestive of non-accidental injury, but it was not possible to prove these injuries caused death, so the cases remain as categorised as unexplained SUDI.
In four cases, carers were convicted of criminal charges following the death including child cruelty, neglect and causing or allowing a child to die.
Only eight cases listed professional working as a reason for holding the SCR; however, all SCRs detailed professional involvement with families and between professionals from different agencies.
Discussion
This study analysed 27 sudden unexpected infant deaths occurring between 2012 and 2014 that led to an SCR. Our findings concerning background parental factors and parenting behaviours contributing to deaths were that these deaths happened in families where criminal convictions, domestic violence, drug and alcohol misuse and mental health problems were commonplace. All but one family were previously known to social care, more than one-third of whom were subject to child protection plans. Non-engagement with services was a problem in two-thirds of cases resulting in families not receiving support and the degree of their difficulties being under-recognised. In a majority of cases, the circumstances of death involved alcohol and drug misuse, with more than half of the deaths involving a parent intoxicated with alcohol or drugs cosleeping with a small vulnerable infant. Frequently, there was a change in family circumstances in the days immediately prior to the death with professionals unaware of these so unable to take protective action. The rationale for holding an SCR included concerns of neglect, parental alcohol or drug misuse, deaths of children subject to child protection plans and concerns about professional working.
The findings from this study are likely to be reliable as we had nearly complete case ascertainment for SCR relating to SUDI cases for the time period in question, a robust and rigorous method of analysis and reached theoretical saturation in the analysis of cases. Previous analysis of SUDI cases in the West Midlands region of the UK found that 6/45 (13%) unexplained deaths occurred in cosleeping situations involving parental drug or alcohol misuse,11 but SCRs are only held for approximately 4% of SUDI cases. Therefore, many SUDI cases similar to those included in our analysis will not have been subject to SCR, so these results may have a wider application. The decision to hold an SCR was largely based on concerning parenting behaviours such as neglect and drug or alcohol misuse; it is therefore unsurprising that we found these behaviours to be a prominent feature in the events leading to infants’ deaths. It does not necessarily follow that these parenting behaviours were directly related to the deaths, only that they were related to the SCR decision. The detailed descriptions of families’ lives does, though, help create a better understanding of the circumstances surrounding these infants’ deaths. The study limitations include the small sample size, lack of any control data and, although the majority of SCRs contained very detailed information, those published as executive summaries only contained few details on the circumstances of death or family backgrounds. These issues potentially reduce the reliability of our conclusions. To our knowledge, no other study has focused exclusively on SUDI cases where there are concerns of child abuse or neglect; this makes our study unique. By examining the extremes of poor parental care in SUDI, this allows us to focus directly on parental actions which may be harmful to infants. In comparison, most other SUDI studies have examined cases recruited from the wider SUDI population, typically most of the cases subject to SCR would not have been recruited into a SUDI research study. Our use of SCR data means that learning from these challenging cases can be captured.
Although the SCR cases may represent an extreme end of SUDI, the differences between SCR cases and other SUDI are becoming less marked. It is well recognised that SUDI now occurs predominantly in association with socioeconomic deprivation.5 12 Similarly, a study from the USA found that 27% of SUDI cases had been referred to child protection services in life.13 It is unsurprising therefore that many of our findings relate well to previous research. The risks for infants of cosleeping with a parent influenced by alcohol or drugs are well recognised, the most recent case–control study of SUDI determined an OR of 10.34 for infants cosleeping with parents who had consumed more than 2 units of alcohol or used illicit drugs when compared with similarly high-risk socially deprived controls.14 A review of national child mortality in New Zealand found that one-quarter of SUDI occurred away from home with infants sleeping in makeshift beds15; this is similar to our results where unplanned changed in family circumstances and living arrangements immediately preceded deaths in one-third of cases. Although none of the deaths were classified as due to accidental asphyxia, the circumstances of death would suggest that asphyxia was highly probable in many cases. It is known that the UK under-recognises accidental asphyxia compared with other countries.11 16
This study shows the pathway through which vulnerable families may inadvertently expose young infants to high-risk situations subsequently resulting in sudden unexpected deaths. Frequently, such deaths are described as ‘tragic accidents’ with the implication that these are unpredictable therefore unpreventable. The narratives of the cases in this study would suggest otherwise and had parents followed UK safe sleep guidance many of these deaths are unlikely to have occurred. Health visitors and midwives should be encouraged to ask both parents about their use of alcohol and other substances, and help them develop safe sleep practices including the avoidance of cosleeping, which can then be used when parents are affected by substances. If parents are enabled to develop and understand safe sleep practices, they may be able to keep to these if there are unforeseen circumstances. Some families, however, are not willing to engage with services; and if there are concerns about parenting this has to be considered and managed as a safeguarding issue to ensure that vulnerable infants are protected. Where there are ongoing child protection concerns in relation to a family with a young infant, particularly where there may be changes in the living circumstances as a result, consideration should be given to how best to support the parents in safe infant care.
A remaining challenge is how to deliver safe sleep messages to high-risk families who may be hard to reach. Despite 25 years of safe sleep campaigns, some parents are still not receiving, not hearing, not understanding, or choosing not to follow this advice, resulting in many infants being exposed to hazardous sleep situations. Future research needs to focus on how best to support and engage with these vulnerable families.
Footnotes
Contributors PS and JJG jointly designed and conducted the study. Both PS and JJG contributed to writing the paper and have approved the final draft.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.