Article Text

Abstract
Background There has been a significant increase in the incidence of paediatric inflammatory bowel disease (PIBD) over the last 25 years although there is no recent data from England. We aimed to analyse changes in incidence within a defined English population over the last decade and compare this to recent and historical incidence data from comparable studies.
Methods The new diagnosis incidence of PIBD (age less than or equal to 16 years) was recorded from a prospective database for a geographically defined area within Southern England (2002–2012). Data were analysed for two separate time periods (cohort 1:2002–2006 and cohort 2:2008–2012) and compared to data from the British Paediatric Surveillance Unit (BPSU) survey in 1998/1999. Data were analysed by age, sex and disease type.
Results There has been an increase in incidence of PIBD from 6.39/100 000/year during cohort 1 to 9.37/100 000/year during cohort 2 (p=0.0002). This compares with the BPSU incidence data in England (1998–1999) of 5.2/100 000/year. There was no statistically significant difference in median age of diagnosis between cohorts (p=0.46).
The incidence of Crohn's disease (CD) was 3.8/100 000/year in cohort 1 rising to 5.85/100 000/year in cohort 2 (p=0.001). The incidence of ulcerative colitis (UC) was 2.01/100 000/year in cohort 1 rising to 2.62/100 000/year in cohort 2 (p=0.1458). Overall PIBD incidence is higher in males in cohort 1 (male-to-female ratio 1.35:1) and cohort 2 (male-to-female ratio 1.5:1).
Conclusions The incidence of PIBD continues to increase with a rise of almost 50% in the last decade in Southern England. The reasons for this increase remain unclear.
- Crohn's disease
- Ulcerative Colitis
- Incidence
Statistics from Altmetric.com
What is already known on this topic
-
25% of inflammatory bowel disease presents in childhood.
-
There has been a significant increase in incidence over the last 25 years.
-
The incidence varies across different populations.
What this study adds
-
There has been a 50% increase in the incidence of paediatric inflammatory bowel disease in Wessex, Southern England over the last 10 years.
-
This is mostly in cases of Crohn's disease.
-
The median age of presentation is unchanged.
Introduction
The underlying causes of inflammatory bowel disease (IBD) remain unclear and likely reflect a complicated interaction between genetic factors and a variety of environmental influences including the intestinal microbiome that combine to develop into disease.1–3
The incidence of paediatric IBD (PIBD) is increasing; a 2011 systematic review of the epidemiology of PIBD looked at 139 studies reporting the trend in incidence of disease; 77% of studies that reported incidence rates showed an increase.4This is supported by recent studies looking at incidence within populations across the UK and Northern Europe5–7 which consistently report an increase over the last 15–20 years.5–8 Twenty five per cent of the total IBD cases present in childhood or adolescence.9 The increase in PIBD is matched by an increase in adult IBD across Northern Europe.10 ,11
The incidence varies significantly between populations ranging from 0.3 to 11.4/100 000/year with the highest rates reported in North America, Scandinavia and Australasia.4 ,8 ,12 The reasons behind this geographical variability are uncertain. It is likely to reflect multiple environmental and genetic factors.12 ,13
Despite the increased disease burden seen in the UK, evident from Scottish and Irish data,5 ,6 there are no recent studies looking at incidence of PIBD in England. The most recent data come from a study published by the Lancet in 2001 from the British Paediatric Surveillance Unit (BPSU). Data covering a 13-month period from 1998–1999 showed an overall incidence of 5.2/100 000/year for PIBD in England, with a higher incidence of Crohn's disease (CD) compared to ulcerative colitis (UC).6 ,14
Several recent studies looking at the incidence of PIBD populations in Sweden, Canada, Scotland and Ireland continue to show a predominance of PIBD in male patients.5–8 Also observed in paediatric cohorts is an increased incidence of CD in contrast to the situation seen in adult IBD which shows an overall higher incidence of UC.15 This is supported by recent data from Europe and North America.5 ,8 ,16
We aimed to analyse changes in incidence within a defined English population over the last decade and compare this with historical incidence data from other comparable populations.
Materials and methods
‘Wessex’ was an historical kingdom in the South of England and the term is now used to describe a National Health Service (NHS) deanery. The ‘loose’ area included stretches from Chichester in the East to Dorchester in the West with the major centres of population being Southampton, Portsmouth and Poole. Together with these large cities, Wessex covers the New Forest National Park and incorporates the historic centres of Winchester and Salisbury, Basingstoke, the Isle of Wight and the Channel Islands. The Paediatric Gastroenterology service based at University Hospitals Southampton (UHS) covers a wider geographical region providing tertiary care for over 650 000 children less than or equal to 16 years of age including recent expansion to the north including Guildford and Frimley.
Defining the Wessex population
In order to accurately estimate incidence cases were included from areas that referred to Southampton across the entire time period studied (2002–2012). Referral from the centres of Southampton, Portsmouth, Poole, Salisbury, the Channel Islands and Dorchester remained consistent across the study period. Through interrogation 116 separate 3–4 character postcode areas were identified that reflected areas consistently referring patients to the service.
Census data for the South of England from 2001 to 2011 show a small decrease in the number of children aged 16 years and under.17 These data did not provide sufficient detail (population and age/sex data not available for each year) by postcode locality to permit analysis by age and gender of this cohort.
Using the 116 defined postcode areas the total population aged 16 and under of these areas were gathered from the Office for National Statistics (ONS), alongside data published by the Jersey and Guernsey authorities.17–19
Following guidance from the ONS single denominator population estimate from the year of 2009 was taken for the whole study. This year had the greatest amount of data (including exact age and sex data) with the highest accuracy due to work on population by postcode undertaken from the ONS.
The population of the Channel Islands was obtained from local authorities and was from the year 2009 to fit with data from the ONS. The total population of the Channel Islands was estimated to be 163 000 with a population aged 16 and under estimated to be 21 199.18 ,19
PIBD data acquisition
All patients diagnosed from 2002 to 2012 were considered.
Data on PIBD cases were obtained from a database managed internally by the Paediatric gastroenterology department at UHS. Information is stored on an APEX database system and can only be entered and altered by those granted access at UHS. It contains demographic and phenotypic data on all diagnosed patients. All patients were diagnosed according to the Porto criteria.20
In order to analyse the variation between time periods, the data were split, all new PIBD cases diagnosed in the 5 years from January 1st 2002 to December 31st 2006 (cohort 1) and all cases diagnosed during the 5 years from January 1st 2008 to December 31st 2012 (cohort 2). These cohorts were chosen to represent the 5 years from the commencement of high-quality data gathering in Wessex and the 5 most recent years. All years were analysed individually to ensure that a single year was not artificially inflating or decreasing incidence in either cohort.
All sex and subclassification analysis has been conducted directly from the data. Children were further divided into the age groups 0–5, 6–10 and 11–16 based to allow for comparison with other studies.5 Statistical analysis of the data was conducted using Pearson's χ2 test for comparison of cohort data. Statistical analysis of trends was conducted using Poisson regression models.
Results
The total number of children diagnosed with PIBD within cohort 1 (2002–2007) was 165 with a median age of diagnosis of 12 years (IQR 4 years). This compares to a total of 242 children diagnosed within cohort 2 (2008–2013) with a median age of diagnosis of 13 years (IQR 3 years), and there is no statistically significant change in median age of diagnosis between these cohorts (p=0.46). There is an increase of 46.6% in overall PIBD incidence over this time period (figure 1). The number of new cases ranged from 28 to 57 per annum (figure 2).
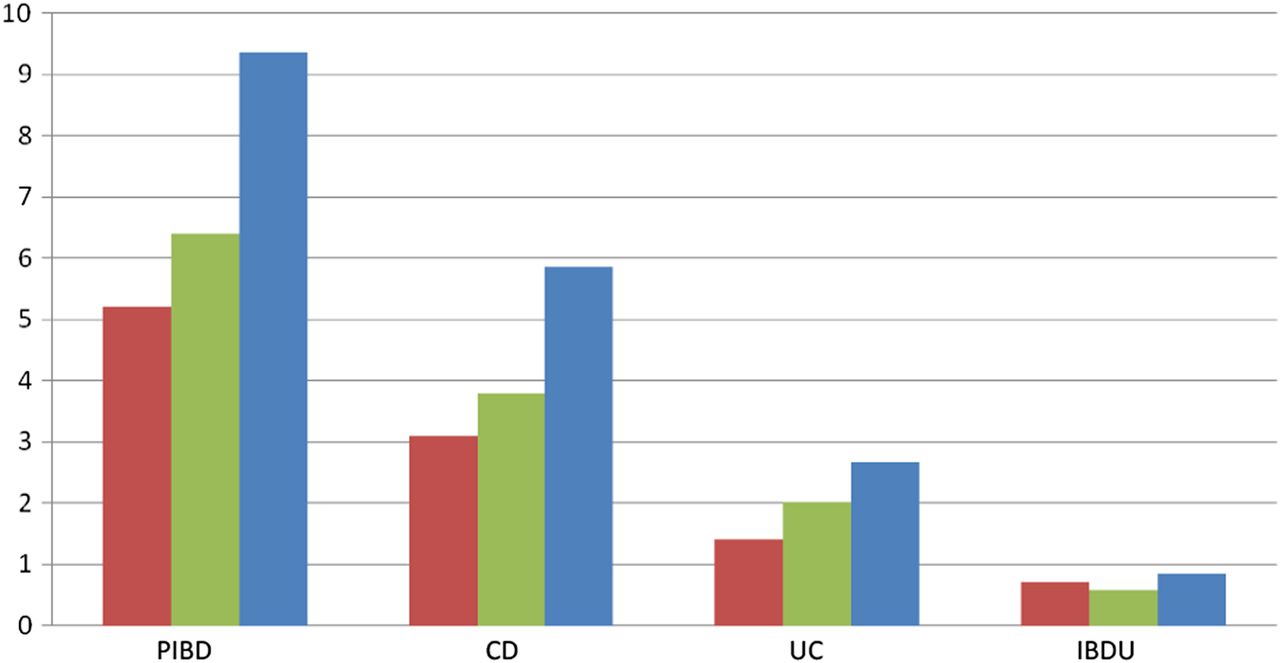
Incidence of paediatric inflammatory bowel disease (PIBD) in Wessex—comparison of incidence per 100 000/year in British Paediatric Surveillance Unit (BPSU) data: 1998–1999 (RED), cohort 1: 2002–2006 (GREEN) and cohort 2: 2008–2012 (BLUE). CD, Crohn's disease; IBDU, inflammatory bowel disease unclassified; UC, ulcerative colitis.
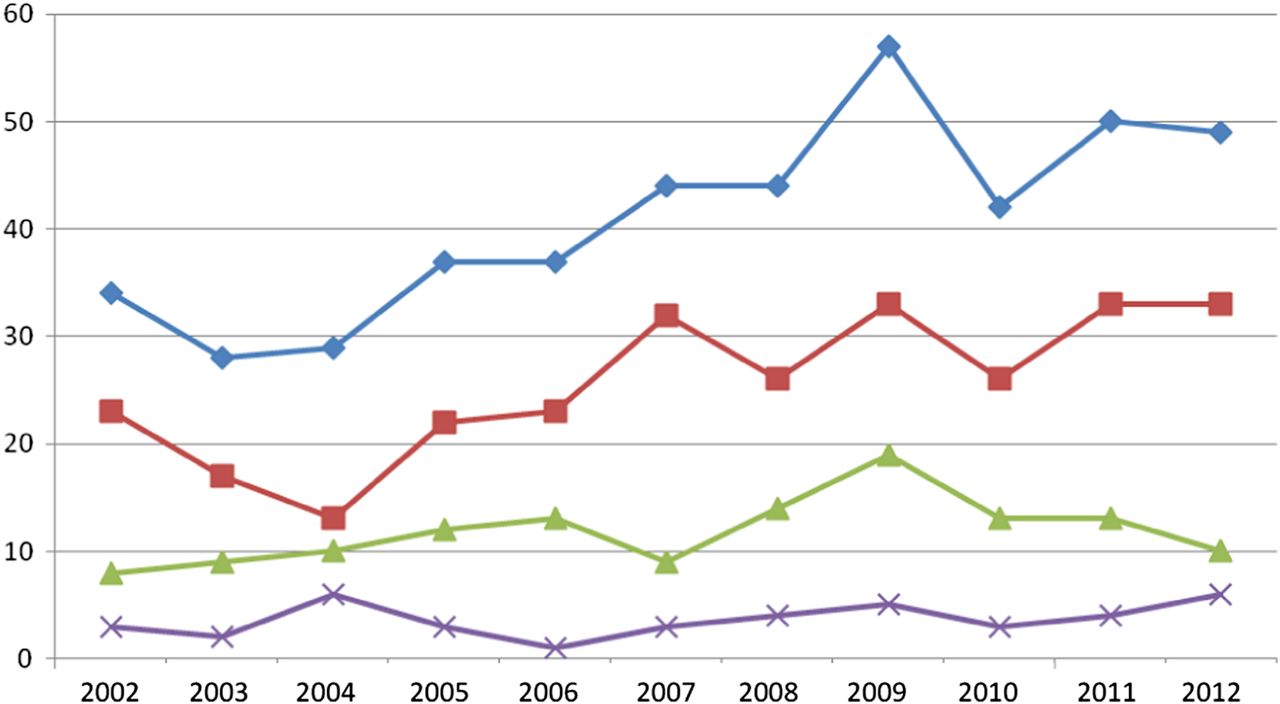
Number of paediatric inflammatory bowel disease (PIBD) cases per year in Wessex (Blue: PIBD, Red: CD, Green: UC, Purple: IBDU). CD, Crohn's disease; IBDU, inflammatory bowel disease unclassified; UC, ulcerative colitis.
Increasing incidence of PIBD in Wessex
There has been an increase in incidence of PIBD from 6.39/100 000/year during cohort 1 to 9.37/100 000/year during cohort 2. This compares with the BPSU incidence data in England (1998–1999) of 5.2/100 000/year.
Analysis of cohort data reveals a statistically significant increase in incidence of PIBD across the 11-year time period studied (p=0.0002). This was mostly reflective of an increase in CD (from 3.80/100 000/year to 5.85/100 000/year, p=0.001).
Analysis of trends between the two cohorts did not reveal a statistically significant difference 1.46, Z=1.67 (95% CI 0.94 to 2.30) (p=0.10).
Crohn's disease continues to predominate in PIBD
The overall incidence of CD in cohort 1 was 3.80/100 000/year compared to an incidence of 2.01/100 000/year for UC. This gives a ratio of 1.9 cases of CD for every 1 case of UC. In cohort 2 the incidence of CD was 5.85/100 000/year compared to an incidence for UC of 2.67/100 000/year. There is an increased ratio in cohort 2 to 2.2 cases of CD for every 1 case of UC. These data are demonstrated in table 1.
Overall incidence rates of PIBD in Wessex
Further comparison of this study's data to BPSU data (for England) shows an increase from 3.1/100 000/year for CD and 1.4/100 000 year for UC since 1998–1999 (male-to-female ratio 2.2:1).
Overall incidence of PIBD is higher in males than females
A male predominance exists for PIBD with the incidence in both cohorts being greater in males than females. Overall PIBD incidence in cohort 1 was 7.33/100 000/year for males and 5.40/100 000/year for females (male-to-female ratio 1.35:1). In cohort 2 incidence was 11.19/100 000/year for males and 7.47/100 000/year for females (male-to-female ratio 1.5:1). These data are demonstrated in table 2 which also shows disease subclassification adjusted rates.
Sex-adjusted incidence rates of PIBD adjusted for subclassification of disease in Wessex
Incidence of PIBD of all types is most common in older children
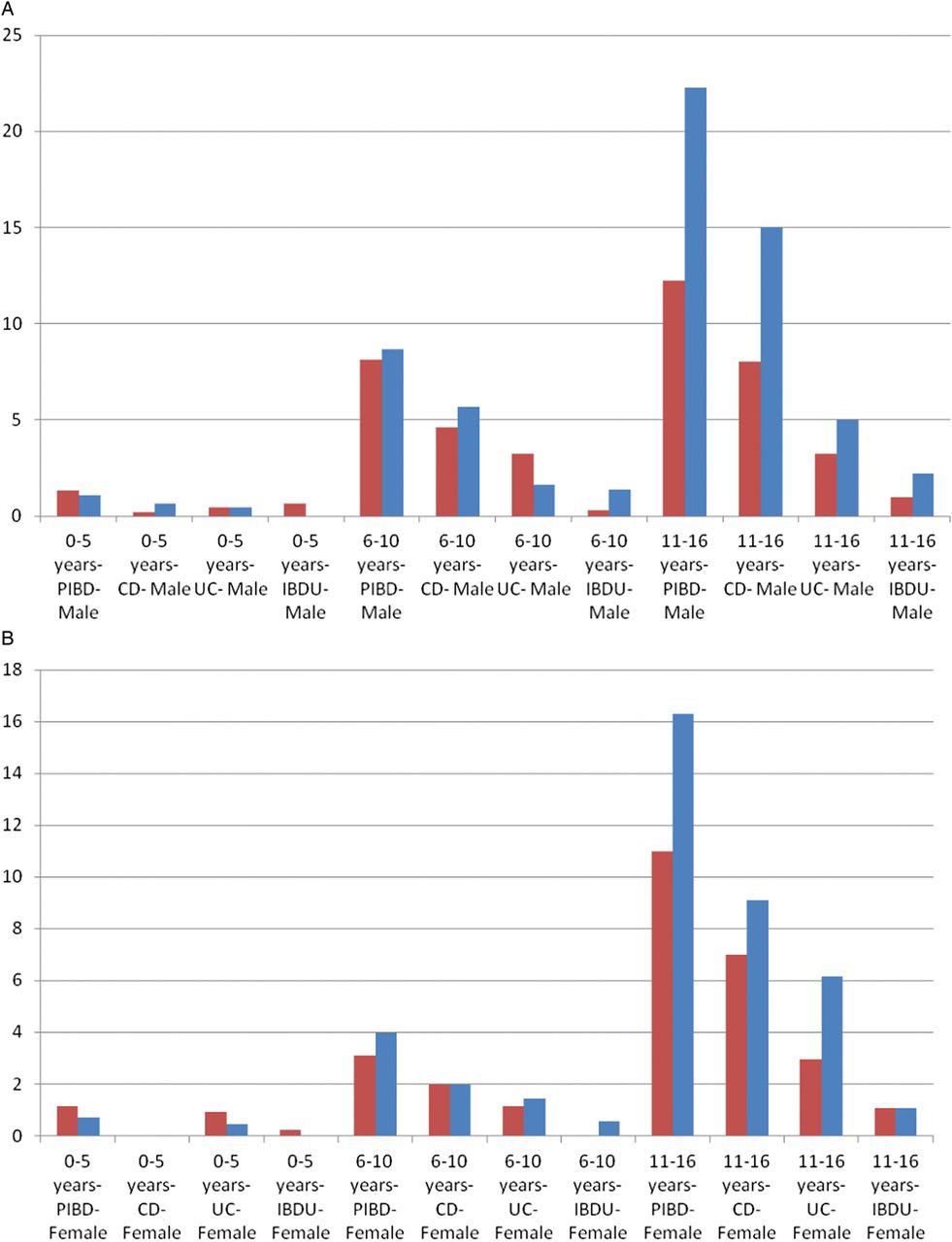
Incidence of CD, UC and inflammatory bowel disease unclassified (IBDU) is most common in the 11–16 age group with an overall incidence of 22.25/100 000/year in males and 16.3/100 000/year in females for all PIBD in cohort 2. This has increased from 12.23/100 000/year in males and 11.01/100 000/year in females for all PIBD in cohort 1. The age and sex-adjusted incidence are concordant with data from other studies (figures 3A,B).
{kind=link}
{kind=link}
{kind=link}
(A) Incidence of paediatric inflammatory bowel disease (PIBD) per 100 000/year by age group in MALES—Cohort 1 (Red), Cohort 2 (Blue). (B) Incidence of PIBD per 100 000/year by age group in FEMALES—Cohort 1 (Red), Cohort 2 (Blue). CD, Crohn's disease; IBDU, inflammatory bowel disease unclassified; UC, ulcerative colitis.
Discussion
Our data clearly show an increasing incidence of PIBD over the 11 years spanning the cohorts. There is an increase in all disease types including total cases and incidence in male and female populations. Specifically there was an increase of 46.6% in cases of PIBD diagnosed within Wessex across the two cohorts. The most significant increase is seen in the overall incidence of PIBD and in CD. There was no statistically significant change in the incidence of UC (p=0.1458) or IBDU (p=0.3236) although numbers of cases increased for both disease.
A summary of data from recent comparable studies can be seen in table 3.
Comparison of PIBD incidence data with other incidence studies (rates per 100 000/year)
Is this an actual increase in incidence of PIBD?
An obvious potential criticism of our data would be that it reflects an increase in the diagnosis of cases that were previously misdiagnosed or not diagnosed at all due to the mild nature of disease, rather than a true increase in incidence of disease. However, there are good reasons to believe that this is unlikely.5
There has been a concurrent increase in the incidence of adult inflammatory bowel disease (IBD) over the last 20 years.10 ,15 This translates to an overall increase in IBD and PIBD and does not simply reflect an increase of disease that was previously diagnosed in the adult population being diagnosed and managed by paediatricians.
The oldest comparable data available consist of one study comparing incidence of PIBD in Scotland in the years 1968 and 1983 revealed a decrease from 1.91/100 000/year to 1.56/100 000/year over these time points.21 Further analysis of disease incidence in Scotland looked at data from 1981 to 1995 and revealed an incidence for CD of 2.6/100 000/year.22
Comparison of data to more recently published studies reveals general concordance in increasing incidence rates. The benchmark survey conducted by the BPSU gathered all new cases of PIBD during a 13-month period from 1998 to 1999 and revealed an overall incidence of 5.2/100 000/year in England.14 The incidence presented here is significantly higher and in keeping with that reported from Scotland where an increase in incidence to 7.82/100 000/year for the time period 2003–2008 was demonstrated.5
Furthermore, the Wessex data from 2002 to 2007 show an incidence of 6.39/100 000/year, the study of Scottish PIBD from 2003 to 2008 demonstrates an incidence that is 1.43/100 000/year more than the Wessex data for a comparable time period.5 This is highly concordant with the difference in Scottish and English data observed in the BPSU study of 1998–1999 where Scotland demonstrated an incidence that was 1.3/100 000/year higher than that seen in England.5 ,14
Data from Ireland over a concurrent time period show a proportionally similar increase in PIBD to this study's data and show an overall lower incidence rate; PIBD incidence rises from 2.5/100 000/year in 2001 to 5.6/100 000/year in 2010.6
These are the first data published from England since the BPSU study in 1999. The data show a dramatic increase in incidence during the time since that publication. No previous data are available for Wessex and we have not identified any regional English data for comparison. We speculate that there will be a continued increase in incidence over future years, whether incidence in England will continue to rise to that reported in Canada (rate of 11.4/100 000/year),8 Sweden (12.8/100 000/year)7 and Norway (10.6/100 000/year)16 remains to be seen.
Strengths and limitations
All new diagnoses of PIBD are prospectively entered onto the database by clinicians at the time of histological diagnosis, ensuring robust collection of data for each case. A limited number of people have access to the database minimising interobserver bias across the years of data collection.
Demographic data collected at the time of diagnosis enabled the authors to accurately define the geographical area from which the IBD population was drawn. The ONS data from 2009 provide a precise estimate for population through calculations conducted by the ONS based on census and local authority data. Adjustment for any increase in referrals from outside the original area has been achieved by selection of patients with postcodes only in both cohort data sets.
One of the limitations of this study is that of possible missed cases due to referrals from the Wessex population area being picked up by another centre or managed by adult services. However, it is unlikely that many cases would be missed; indeed over the 11 years of this cohort the referral area has increased, and referral patterns have not significantly changed from the postcode areas chosen, ie patients have been managed from the 116 postcode areas chosen throughout the whole study period.
A potential weakness of this study is using the single population estimate for Wessex over the 11-year period. Several reasons led to this decision; this year had the greatest amount of data based on postcode locality from the ONS; alongside this, it was felt that by taking a time point within the second cohort a highly accurate incidence for this group would be achieved. Furthermore, over the study period the population of Southern England aged 16 years or below has decreased17 and recommendations from the ONS on population data accuracy demonstrated 2009 data as being the most robust for estimating postcode population. Analysis would achieve an accurate incidence in both groups and would specifically avoid over estimating incidence in the second cohort due to overall population decrease over this time. These factors would all lead to an underestimate of true incidence within cohort 2 and therefore the overarching increase in incidence would still remain.
Conclusion
This study shows a continuing rise in incidence of inflammatory bowel disease in children with a 46.6% increase in cases over the last decade in Southern England. The reasons for this increase are unclear and although it may partly reflect earlier diagnosis and improved referral patterns it is likely that it does represent a true increase in incidence.
References
Footnotes
-
Contributors JA collected the data, analysed the data and drafted the manuscript. AW, AB, NA, SE contributed to data collection, data analysis and commented on the manuscript. RMB supervised the project contributing to data collection, data analysis and is the guarantor for the manuscript.
-
Competing interests None.
-
Provenance and peer review Not commissioned; externally peer reviewed.