Article Text

Abstract
Introduction Aerosol therapy in infants may be greatly compromised by face mask rejection due to squirming and crying. Lung aerosol deposition in crying infants may thereby be greatly reduced. Since ‘suckling’ on a pacifier calms infants, they should more readily accept a face mask that incorporates a pacifier. However, since infants must breathe nasally while suckling, lung aerosol deposition may be reduced due to impaction in the nose.
The aim of the present pilot study was to compare lung aerosol deposition while suckling on a pacifier incorporated into a mask with that obtained while inhaling from a conventional mask.
Methods Twelve infants <12 months old and who regularly used pacifiers participated as their own controls. Lung aerosol deposition was measured scintigraphically (technetium-99mDTPA-labelled normal saline aerosol, MMAD (Mass Median Aerodynamic Diameter) 3 um and GSD (Geometric Standard Deviation) of 2) via jet nebuliser using a conventional mask versus ‘suckling’ on their pacifier incorporated into a unique mask.
Results Mean lung deposition (±SD) while suckling using a mask with attached pacifier (1.6±0.5% in the right lung) was similar to that with a conventional mask (1.7±0.9%, p=0.81).
Conclusions Lung aerosol deposition during nasal breathing while suckling on a pacifier-equipped mask is similar to that in infants breathing quietly using a conventional mask, and results comparable with previous data in infants and in nasal breathing models of an infant's upper respiratory tract. Using a pacifier during aerosol treatment in infants may be as efficient as conventional treatment without a pacifier.
Statistics from Altmetric.com
Introduction
It is known that aerosol therapy in infants is often compromised by face mask rejection due to squirming and crying.1 Lower respiratory tract deposition in crying infants may thus be greatly reduced.2,–,6 Since suckling calms infants, they should more readily accept aerosol treatments while sucking on a pacifier. Indeed, many parents report that they use pacifiers inserted directly into the mouth when delivering aerosol treatments to their infants by means of a mask. This practice is also commonly used in some countries (Dr Michael Harari, Royal Children's Hospital Melbourne Australia, personal communication). However, to the best of our knowledge, the efficiency of this practice has not previously been studied.
The nose has the highest resistance, flow and turbulence in the respiratory system.7 Mathematical models have suggested that under conditions of tidal breathing, the nose in infants may be more efficient at excluding foreign particulates from the airways compared with adults.8 Thus, the nose may be a very effective aerodynamic filter for potentially noxious particles and for therapeutic aerosols. Unsurprisingly, if the upper respiratory tract (URT) aerodynamic filter is bypassed by aerosol inhalation through the mouth, delivery of medication to the lungs of children is two to threefold greater.9 For these reasons, it is possible that lung aerosol deposition may be decreased in infants who must breathe through the nose when they use a pacifier.
What is already known on this topic
▶ Aerosol therapy in infants is often compromised by face mask rejection due to crying. Lung deposition in crying infants is reduced compared to calm infants.
▶ Since suckling calms infants, they should more readily accept aerosol treatments while sucking on a pacifier.
▶ Many parents report that they use pacifiers when administering aerosol treatments by means of a mask. However, this practice has not previously been studied.
What this study adds
▶ Lung aerosol deposition during wet nebulizer treatment while suckling on a pacifier-equipped mask is similar to that in infants breathing quietly using a conventional mask.
▶ Using a pacifier may greatly enhance compliance to aerosol treatments in infants.
Labelling the aerosol particles with a γ emitting isotope marker and quantifying its deposition scintigraphically by means of a γ camera is a simple, safe and commonly used method to assess aerosol deposition throughout the respiratory tract.
The aim of the present pilot study was to determine if treatment administered to infants who are pacifier users, using a unique mask, which incorporates their own pacifier into its anterior wall (SootherMask), results in decreased lung aerosol deposition compared with treatment administered through a conventional mask.
Subjects and methods
This pilot was part of a larger study designed to determine the mechanism by which the reported reduction in sudden infant death syndrome mortality occurs, which appears to be associated with the use of pacifiers10 (NIH NCT01120938).
Parents of inpatient and outpatient infants (n=12) aged 1–12 months on regular aerosol therapy provided signed informed consent. The study was approved by the local institutional review board and the Ministry of Health. Inclusion criteria were: hospitalised wheezy infants, who required frequent inhaled aerosol treatments, as determined by the attending physician,11 and who were regular users of pacifiers. Outpatients were infants who also used pacifiers and were on regular, at least twice daily, inhaled therapy at home. Exclusion criteria included patients who reported histories, signs or symptoms of airway abnormalities such as previous airway surgery, tracheotomy, obstructive sleep apnoea, snoring, anatomical anomalies of mouth palate nose, pharynx and trachea. Patients with chronic cardiopulmonary disease such as bronchopulmonary dysplasia, congenital heart disease, immune deficiency or cystic fibrosis were also excluded.
Methods
This was a randomised, non-blinded cross over study. Using computer-generated randomisation, infants were assigned to receive the first radiolabelled aerosol treatment either by the SootherMask into which the infant's own pacifier was inserted (figure 1) or by a conventional Hudson bottom-loaded face mask (Hudson RCI Corporation, Research Triangle Park, North Carolina, USA) without a pacifier. The alternate treatment was given at least 6 h later (for inpatients) or within 12–24 h for outpatients (depending on their regular treatment schedule). We consider this interval optimal in order to minimise pathophysiological changes in airway calibre over time and reduce interference from residual radioactivity in the respiratory tract following the first treatment.12

Use of pacifier and mask during nebuliser treatment.
For each of the study treatments, 0.5 ml of 0.5% salbutamol respiratory solution in 2 ml normal saline (final loading volume of 2.5 ml) was administered by means of the mask. The parent was instructed to hold the mask as s/he usually did at home (or on the ward). No additional pressure was applied to ensure a tight seal of the mask to the face.
The normal saline solution was labelled with technetium-99mDTPA (99m Tc). The dose of 99m Tc to be given to each patient determined before the inhalation procedure was found to be 15 uci/kg.13 As inhalation exposure is 0.05 RAD/mci,8 or 0.00075 RAD/kg, the maximum exposure for a 20 kg child was 0.015 RAD. Addition of 99m Tc has no physical effect on aerosol characteristics.14 Aerosol was generated with the same jet nebuliser (Hospitak Opti-Mist clear, Unomedical, McAllen, Texas, USA) using a constant air flow of 8 l/min for 5 min.
Patients received the treatments in a special room in the nuclear medicine department, used only for this purpose. No person other than the patient's parent and physician were allowed in the room. Radioactivity protection monitoring was carried out regularly before and after each study to ensure that no excess radioactivity was present in the room following treatment. To avoid contamination of the skin of the infant's chest during treatment, which would interfere with quantifying lung scintigraphy, the infant's body was enclosed in a disposable nylon wrap (similar to that in which the care giver was gowned) which was removed prior to scintigraphy.
The radiation dose of 99m Tc aerosol used in this study was calculated according to the Medical Internal Radiation Dose Committee.12 It is equivalent to the radiation received during 3 weeks of normal cosmic ray exposure while outside or a 12 h airplane flight and is much lower than the dose used in most diagnostic imaging procedures. 99m Tc is a pure γ emitter and has a short (6 h) physical half life.12
The initial amount of 99m Tc and the amount which remained in the nebuliser immediately after completion of nebulisation were counted using a dose calibrator (Capintec Ramsey New Jersey, USA).
Anterior and posterior scintigraphic scans of 120 s duration were obtained after each treatment using a double plate scanner (Symbia, Siemens GMBH, Munich, Germany) and γ camera counts were quantified as previously reported.4
Briefly, counts were measured in the tubing and in three body regions of interest (ROI) – lung, stomach and URT. The right lung was chosen in order to minimise interference from the oesophagus and stomach. This deposition evaluation technique has been in use clinically worldwide for several decades and has been used in previous studies.2 4 It has regularly received ethics committee approval in the past.
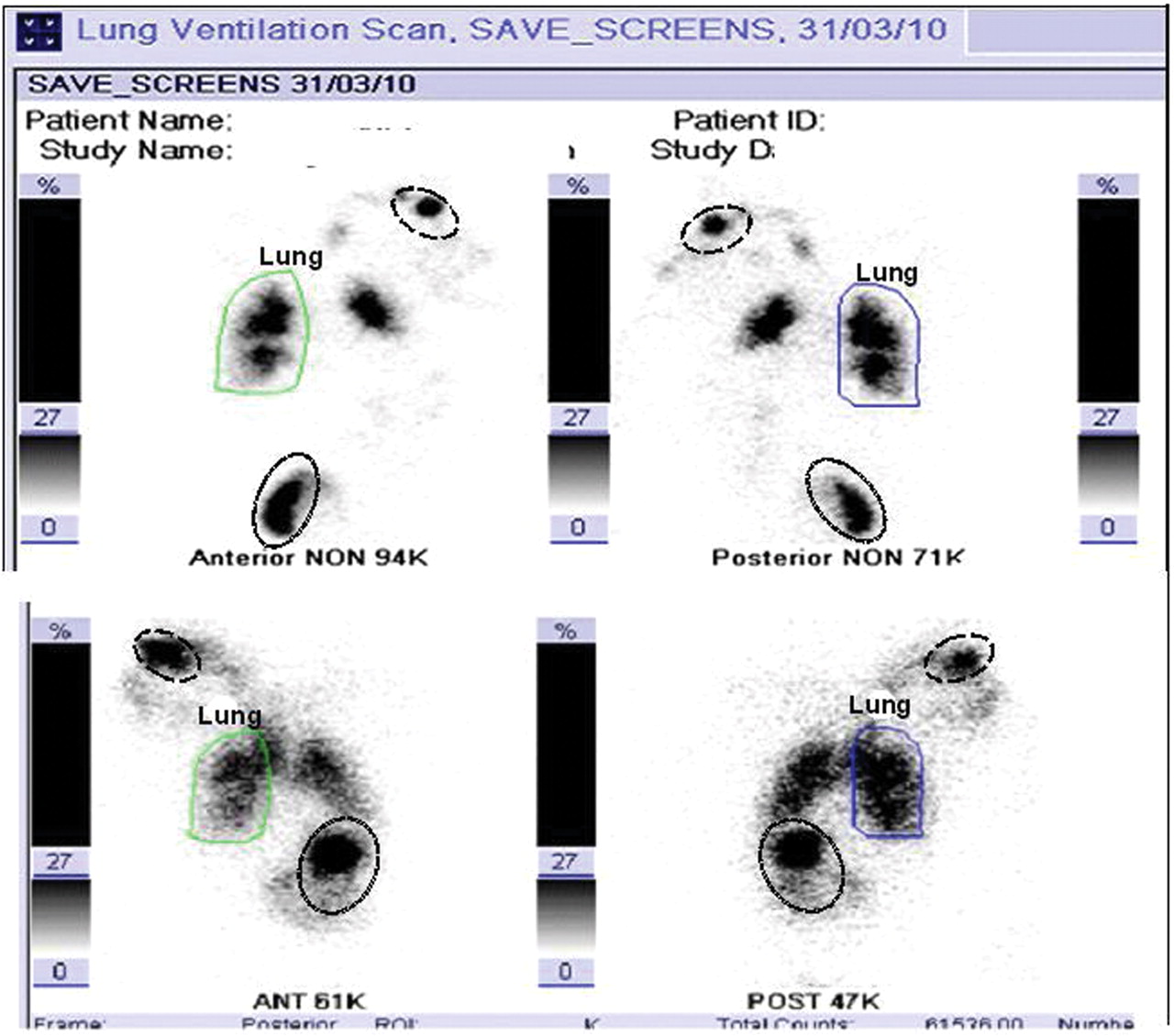
A scintigraphic representation of the regions of aerosol deposition is shown in figure 2.

Anterior (left) and posterior (right) views of the subject with (upper panel) and without (lower panel) a pacifier. The green ‘lung’ outline is the initial lung regions of interest (ROI) drawn on the right lung in the anterior view to measure the radioactivity counts (94 000 in this example). The same ROI was then copied and pasted onto each subsequent image to ensure an identical ROI. Deposition in any ROI was calculated as the percentage of radioactivity in that region relative to the amount delivered from the nebuliser during that treatment. Similarly, outlines were also drawn for the upper respiratory tract ROI (dashed line) and stomach ROI (dotted line).
Statistics
Analysis of data was carried out using SPSS V.11.0 statistical analysis software (SPSS Chicago, Illinois, USA). Statistical tests were two sided conducted at the 0.05 level. Paired t tests were used to compare deposition between the two treatments. Deposition and age indices were related by simple regression.
Sample size
The sample size was based on previous lung deposition data in infants receiving aerosol therapy.4 Based on these data, we estimated that there would be a more than 80% chance of detecting a 50% difference in deposition between the groups when sample size (n) is 12 patients in each treatment group.
Results
The infants' demographics and deposition values for the various ROIs (right lung, stomach and URT) are presented in table 1.
Demographics and deposition (%) values for the various ROIs (p>0.05)
A total of 12 infants (seven girls and five boys) were enrolled. Their mean age was 6.3 (SD=2.6) months and their mean weight was 7.3 (SD=1.7) kg. There were two inpatients (#7 and #11) diagnosed with acute bronchiolitis, whereas the rest of infants were outpatients who suffered from recurrent wheezing.
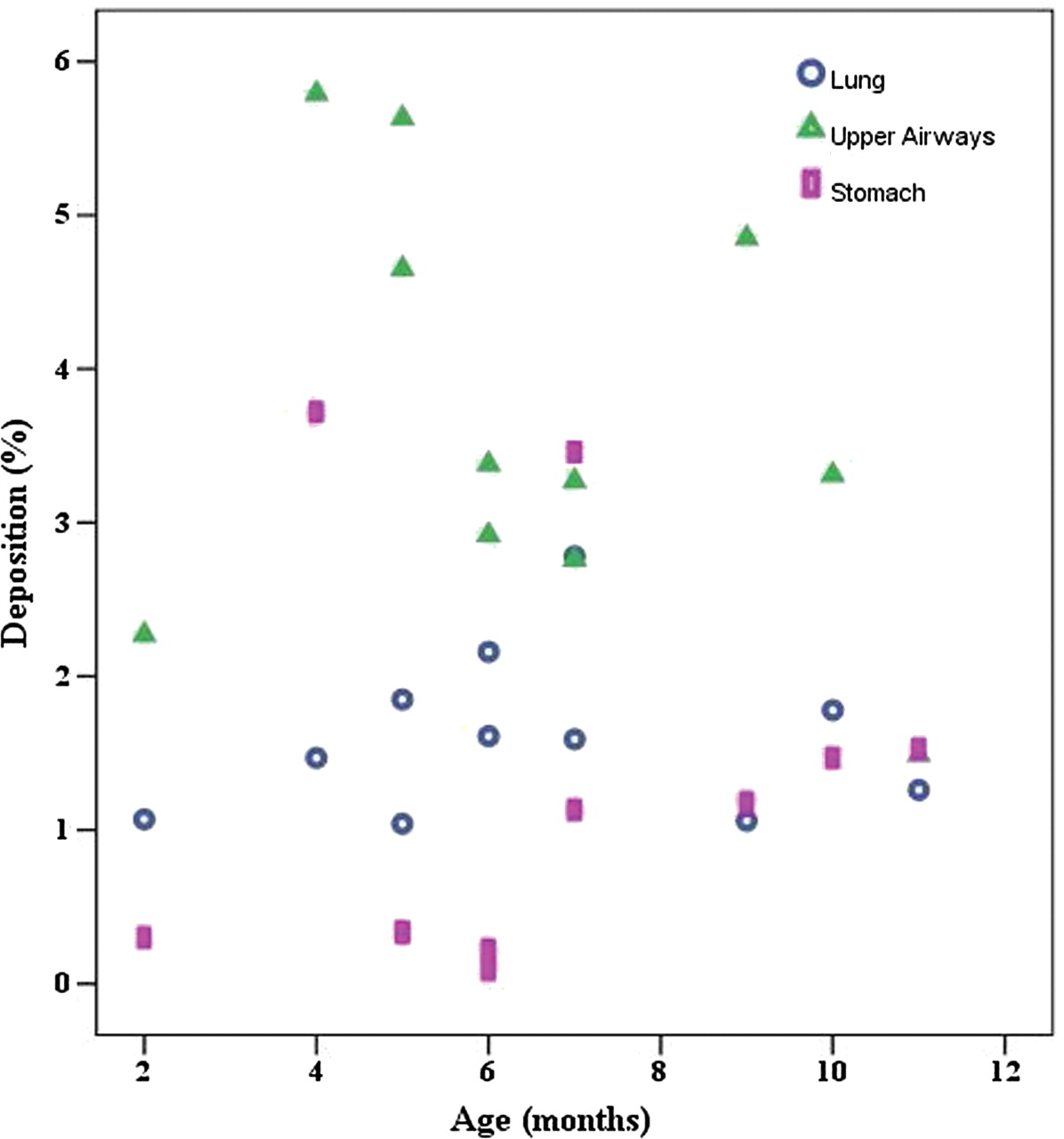
There was no significant difference in lung deposition with or without a pacifier nor were significant differences found in other ROIs or in the tubing. There were no correlations between deposition and age of the infants (figures 3 and 4).

Deposition versus age after treatments without a pacifier.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Deposition versus age after treatments with a pacifier.
In general, treatments with the pacifier were better accepted, and crying was substantially less during pacifier treatments. Three crying infants (#7, 10, 12) tended to have lower lung and greater URT deposition but the differences did not reach statistical significance.
Discussion
The present study demonstrates that the use of a pacifier incorporated into an aerosol facemask used to administer aerosol therapy does not adversely affect lung deposition of aerosol in the majority of infants who are used to using a pacifier and who have previously accepted aerosol therapy by facemask. Administration of inhaled medications to infants may be a very demanding and thankless task.15 Thus, any improvement for making aerosol administration more ‘infant-friendly’ and acceptable should improve aerosol administration in this age group. Since the pacifier is a natural infant-calming device used by many care givers for this purpose, the use of the infant's own pacifier (many infants reject an unfamiliar pacifier) incorporated into a well-designed facemask to assist aerosol administration by minimising resistance to the mask would be a logical choice. Indeed, many parents report using a pacifier during aerosol treatment in order to calm their uncooperative babies. To our knowledge, this approach to administration of aerosol therapy has not previously been studied. The present study demonstrated that inserting the pacifier into the aerosol mask and allowing the infant to suck on it during aerosol inhalation was better accepted and did not have any detrimental effect on lung deposition compared with conventional face mask application. In older children and adults it is known that compared with oral breathing, nasal inhalation reduces lung deposition of aerosolised medication. A likely explanation for the lack of an adverse effect in our study is the fact that infants are, for the most part, preferential nose breathers for the first 12–18 months of life.16 This is thought to be due to both anatomical and physiological reasons such as the proximity of the epiglottis to the soft palate in infants. It is likely that infants inhale aerosols through their nose regardless of whether there is anything in their mouth. Thus, it is unlikely that oral ‘suckling’ on a pacifier would have an adverse effect on aerosol delivery to infants. This changes markedly in older kids when oral breathing of aerosols is encouraged by the care giver and the effect of nasal aerosol particle filtration diminishes.8
Pacifier use during aerosol inhalation may be best suited to those infants who are regular or at least fairly frequent pacifier users although even those who do not regularly suck on a pacifier or whose parents may, in general, be averse to pacifier use, may be calmed by using one during aerosol therapy with a mask. In this regard, the view held by some paediatricians and thus by some parents that use of a pacifier makes infants averse to being breast fed has recently been countered by a study that showed that this was not the case.17 Additionally, as eluded to above, the regular use of pacifiers may also have a beneficial effect since it has been demonstrated that infants who use a pacifier have a lower incidence of sudden infant death syndrome.10
We acknowledge that in the present study only infants who were ‘regular’ pacifier users and who were already receiving treatments by masks were enrolled. We are currently studying infants requiring therapeutic aerosols who do not regularly use pacifiers or had not previously received treatments by mask to determine if they can nevertheless be encouraged to accept the pacifier mask (SootherMask) device.
The deposition of aerosol in the lungs using pacifiers and nasal breathing was similar to that reported previously in infants.2 4 18 It is thus reasonable to conclude that sucking on a pacifier, while inhaling aerosol nasally, does not appear to have an adverse effect on aerosol delivery to the lower respiratory tract using a small volume nebuliser for aerosol administration. It is likely that the results would be similar if aerosol therapy was administered by means of MDIs with a valved aerosol holding chamber. Confirmation of this hypothesis clearly requires further study.
In conclusion, this study has shown that infants sucking on a pacifier incorporated into a mask while inhaling aerosol from a continuously operating small volume wet nebuliser achieve similar lung deposition compared with the use of a standard mask since under both conditions aerosol inhalation is almost exclusively via the nose.
References
Footnotes
-
Competing interests Drs Amirav and Newhouse have patent rights for devices for delivering aerosols to infants and Michael Newhouse is the consulting Chief Medical Officer of InspiRx, developer of the SootherMask. All the other authors have indicated they have no financial relationships relevant to this article to disclose.
-
Ethics approval Approval provided by the local IRB and Ministry of Health.
-
Provenance and peer review Not commissioned; externally peer reviewed.