Article Text

Abstract
Background The incidence of vitamin D deficiency is unclear in the context of continuing demographic changes and the introduction of new public health measures.
Methods All cases in which vitamin D deficiency was suspected as the primary cause of the clinical presentation were studied.
Results Between 2002 and 2008, 160 cases of symptomatic vitamin D deficiency were identified with twice as many cases in 2008 (n, 42) as in the previous years. The median age of the cohort was 24 months (range 2 weeks-14 years).Three cases were recorded in children of European background, whereas the rest were in children of South Asian, Middle Eastern or sub-Saharan ethnic background. Presenting features included bowed legs in 64 (40%) and a fit in 19 (12%). In one infant, concerns were raised following a presentation with cardiac failure and hypocalcaemia.
Summary Symptomatic vitamin D deficiency remains prevalent in the West of Scotland. There is a need for effective public health education, action and surveillance.
Statistics from Altmetric.com
In many industrial towns in the UK, nutritional rickets associated with vitamin D deficiency was identified in children of South Asian origin in the 1970s,1 and the condition was dramatically reduced with targeted vitamin D supplementation.2 Although guidelines for vitamin D supplementation were issued by the UK government in 1994, a survey performed in 2001 reported the continued presence of vitamin D deficiency.3 Concerns about the ineffectiveness of a number of aspects of the Welfare Food Scheme4 led to the implementation of the Healthy Start Scheme across the UK in November 2006. One of the elements of this scheme, which was first piloted in the southwest of England, is the provision of free vitamins for socioeconomically disadvantaged young children and pregnant and lactating women. Qualification for the scheme is judged on receipt of certain benefits, and a specific application must be made. Furthermore, asylum seekers are not entitled to Healthy Start benefits. There are a number of characteristics of a city such as Glasgow (climate, latitude and population mix) that place its inhabitants at a high risk of vitamin D deficiency. The aim of the study was to analyse the cases that had presented to the Royal Hospital for Sick Children and in whom vitamin D deficiency was considered the primary problem. We anticipate that collection and reporting of these data will facilitate the development of a monitoring system for this condition and develop effective pathways for prevention and management of nutritional vitamin D deficiency in children.
Patients and methods
Children who presented with symptomatic vitamin D deficiency at the Royal Hospital for Sick Children, Glasgow, between January 2002 and December 2008 were retrospectively identified by a range of methods including, (1) clinical biochemistry activity data that recorded all children who had a serum 25-hydroxy vitamin D (25-OHD) measured and was below 50 nmol/l, (2) diagnostic imaging records where the term “rickets” or “vitamin D deficiency” was included in the request or the report of the X-ray and, finally, (3) clinical activity data for the metabolic bone service. Those children who were already attending the hospital with a chronic disease such as renal disease, liver disease, gastrointestinal disorders, inherited metabolic disorders and skeletal disorders were excluded. Ethnic background was broadly categorised by knowledge of names and country of origin as Europe, North Africa and the Middle East, South Asia, Sub-Saharan Africa and others. Over the period of study, out of the 168 children who were identified, eight children were excluded as records showed that, although they presented with suspicion of vitamin D deficiency, they did not have any clinical symptoms or signs of symptomatic vitamin D deficiency, no biochemical abnormalities consistent with vitamin D deficiency (low vitamin D, hypocalcaemia or raised parathyroid hormone (PTH)) or radiological features of vitamin D deficiency (stippling, irregularity and cupping of the epiphyses or splaying or sclerosis of the metaphyses). Any child with an isolated finding of a circulating 25-OHD concentration below 50 nmol/l and no supporting X-ray or clinical features of vitamin D deficiency was not included. Two different methods for biochemical assessment of vitamin D status were used over the period of study. From 2002 to February 2006, the Nichols chemiluminescent 25-OHD immunoassay was used on the Nichols Advantage automated immunoassay platform (Nichols Institute Diagnostics, California, USA). As from February 2006, the method was switched to an enzyme-linked immunoassay (IDS 25-hydroxyvitamin D EIA, Immunodiagnostic Systems, Tyne & Wear, UK). For both systems, the between-batch precision (coefficient of variation percent) was less than <15%. As well as measuring 25-OHD3, both assays claimed to measure 25-OHD2, but the proportion of 25-OHD2 measured has been the subject of considerable debate.5
Results
Demography
Among the 160 cases of symptomatic vitamin D deficiency, the annual incidence was 23 cases per year. However, the absolute annual incidence increased over the study period, reaching a peak of 42 cases in 2008, with the greatest increase in patients with an ethnic background of the Sub-Saharan region of Africa, North Africa or the Middle East (figure 1). Three cases were noted in children of a European ethnic background. Sixty-two (38%) children were referred directly by primary care practitioners, 29 (18%) were referred from other out-patient departments, 25 (15%) were referred by A&E, 25 (15%) by the orthopaedic department, one case was referred by the Intensive Therapy Unit (ITU), and in five (3%) cases, the source of referral was unclear. A further 13 cases had been admitted to the hospital with a vitamin D deficiency-related problem. Out of the 160 cases, 100 presented between March and August and the remainder presented between September and February.

Number of cases presenting each year between 2002 and 2008. Each year's cases have been categorised according to four broad ethnic backgrounds to illustrate temporal changes in the relative proportion of cases from these ethnic groups.
Clinical features
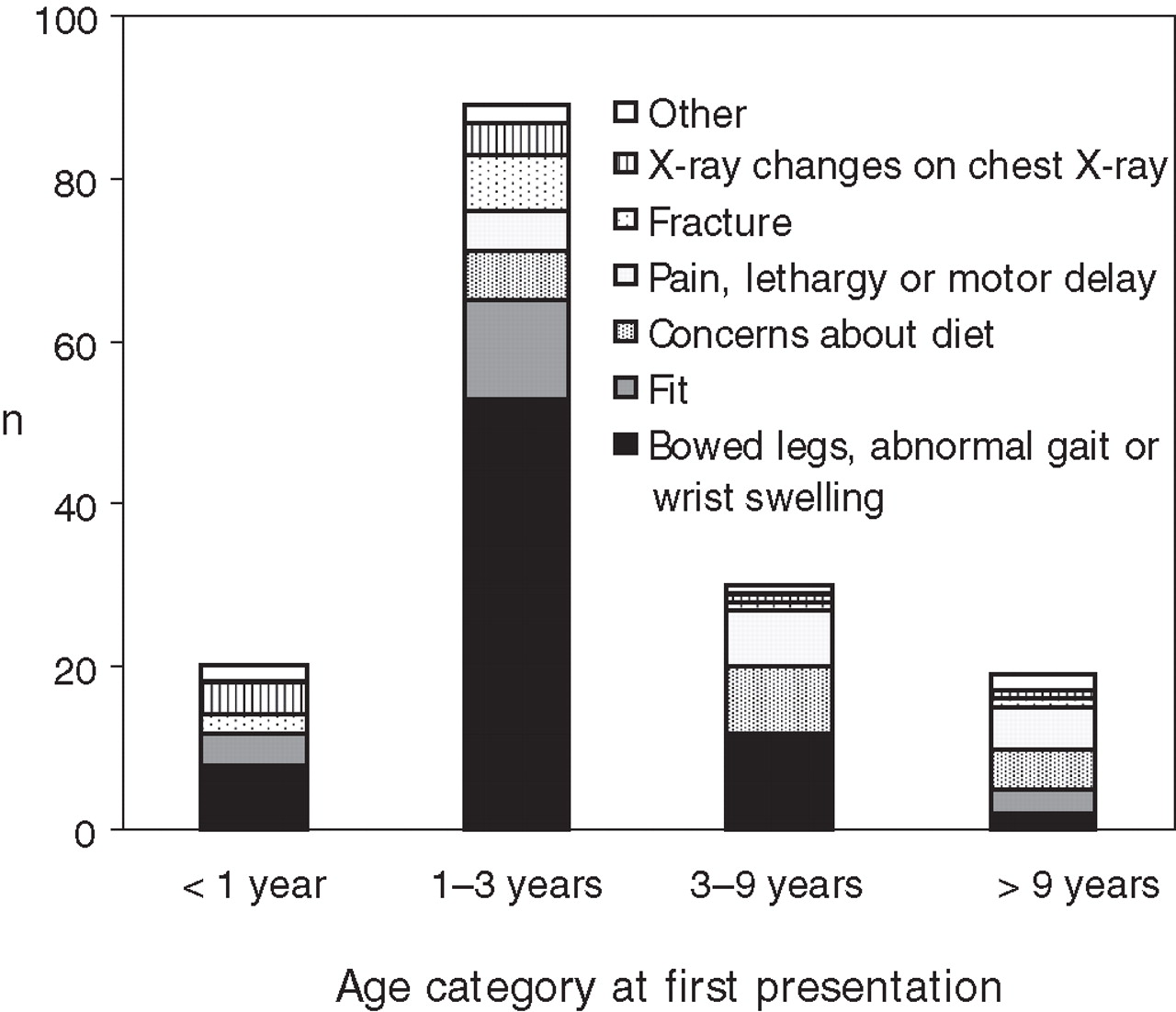
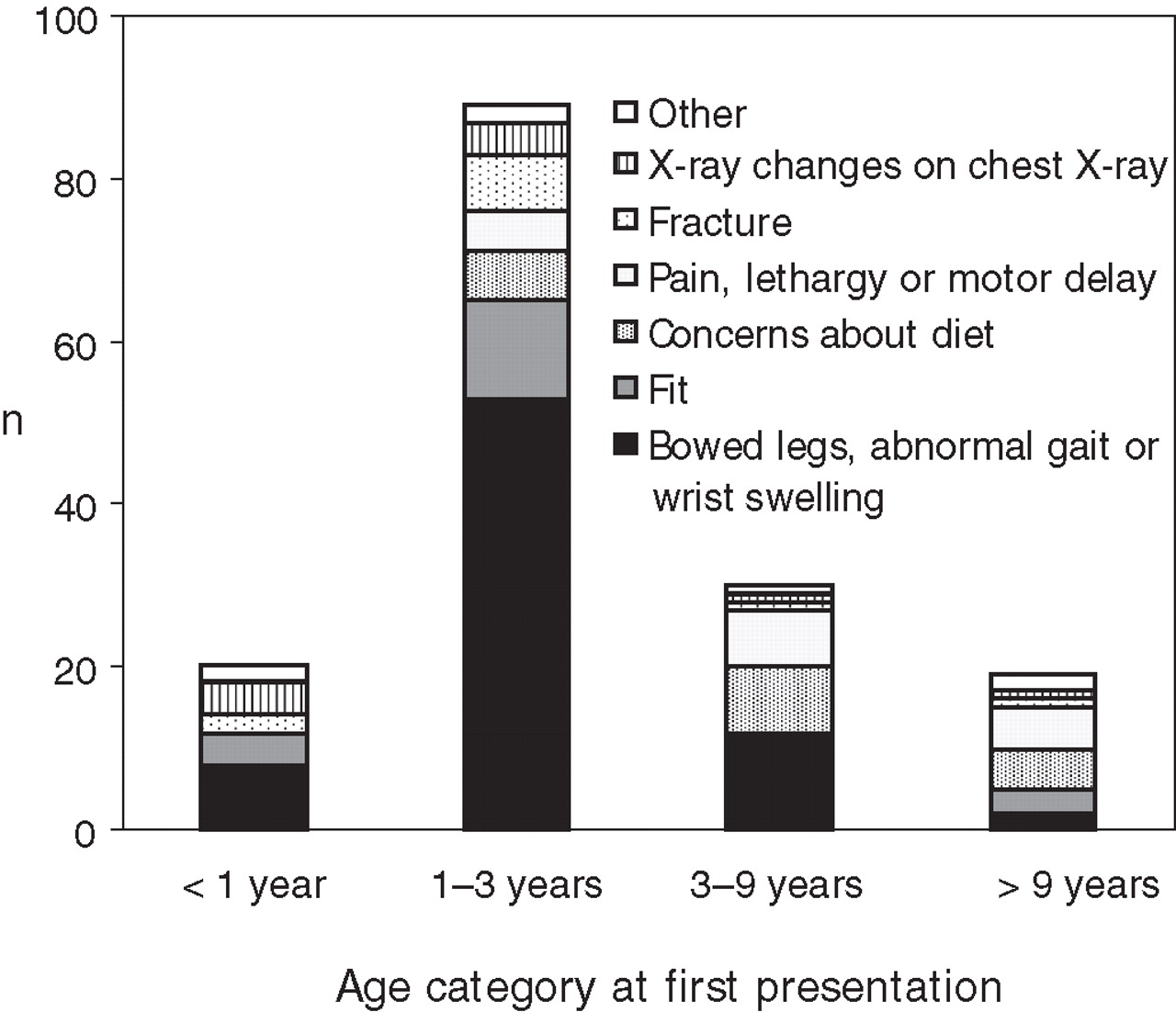
The median age of the cohort was 24 months (range 2 weeks to 14 years). Out of the 160 cases, 77 were girls and 83 were boys. Presenting features included bowed legs in 64 (40%), a fit in 19 (12%) and suspicion after X-rays in children with fractures in 11 (7%) (figure 2). One of these children had suffered from both a fracture and a fit. In another 13 (8%) cases, vitamin D deficiency was suspected after X-rays were performed for limb pain. In 13 (8%) and in 10 (6%) cases, vitamin D status was investigated because of dietary concerns or following a chest X-ray which highlighted rickets, respectively. In four (3%) cases, the complaint was of swollen wrists, in three (2%), suspicions were raised after presentation with developmental delay, three (2%) had a positive family history and two (1%) had symptoms of general lethargy. One child had asymptomatic hypocalcaemia, one child had an incidental finding of a raised alkaline phosphatase (ALP) concentration. One infant had presented with a fracture and signs of a respiratory tract infection and there was one infant where concerns about vitamin D deficiency were raised following a presentation to ITU with cardiac failure and hypocalcaemia and which resolved following treatment with calcium and vitamin D. In four cases, insufficient evidence was available.
{kind=link}
{kind=link}
Reason for referral for investigation and management of 160 children with suspected vitamin D deficiency according to age categories at presentation.
X-ray features
Among the 132 cases, 42 (32%) did not have any sign of rickets, 70 (53%) had clear signs of rickets and 20 (15%) had equivocal signs of rickets. The median age of children with clear signs of rickets was 20 months (5th, 95th, 4.9, 29) compared to 28 months (8.4, 64) for those children without any signs of rickets (p=0.03, Wilcoxon-signed rank).
Biochemistry
Out of the 160 cases, data on serum calcium, phosphate, 25-OHD, PTH and ALP were available in 152 cases. Details of the biochemistry results are presented in table 1. In general, children presenting with hypocalcaemia had a lower serum phosphate and 25-OHD and a higher PTH and ALP (table 1). Radiological rickets was evident in 30/44 (68%) hypocalcaemic cases and 61/82 (74%) normocalcaemic cases. Hypocalcaemia and hypophosphataemia were more commonly encountered in the infants and in children older than 9 years old. The infants were, in fact, more likely to have more profound vitamin D deficiency and show a raised ALP and PTH. Thirteen (8%) children had 25-OHD concentrations greater than 60 nmol/l, and this was attributed to a recent history of vitamin D2 supplementation. Out of these 13 children, seven had signs of rickets on X-ray and others had presented with clinical features of vitamin D deficiency including bowed legs, fits and lethargy. Among the 19 children who presented with a seizure, all were hypocalcaemic at presentation and seven (37%) were still hypocalcaemic when their circulating 25-OHD concentration was checked. The median serum calcium in the children who had a fit was 1.72 mmol/l (range 1.45–2.16).
Differences in the age, extent of biochemical features and radiological evidence of rickets in children with hypocalcaemia and those without hypocalcaemia at presentation
Discussion
This report comprises the largest series of symptomatic vitamin D deficiency that has ever been reported in the UK or in any other developed country, and it shows that the number of cases of profound vitamin D deficiency is currently increasing. As vitamin D deficiency has a variety of different presentations, it is highly likely that this report is an underestimate of the true incidence of this condition. It is unlikely that the increasing incidence is due to increased awareness, as in the majority of cases the presenting feature (such as bowed legs, hypocalcaemic seizure, rickets on an X-ray) would raise a suspicion of vitamin D deficiency.
Our observations of the increasing incidence clearly suggests that current public health measures have not yet had a beneficial effect on prevention of vitamin D deficiency in Glasgow. The change in the relative proportion of cases from different ethnic origins of this community reflects the changing patterns of immigration and birth patterns in the West of Scotland. In addition, although the families of a number of cases were in receipt of state benefits, it was also noted that a number were professionals in paid occupation and a number of families were asylum seekers. Our experience of vitamin D deficiency in three cases of a European background strengthens our suspicion that vitamin D deficiency is present across the community.
Our survey clearly shows that a sizeable proportion of affected children, particularly infants, do not simply have bowing deformities of their legs but also have seizures and fractures. Our data would suggest that overt cardiomyopathy is a rare but, nevertheless, very serious complication of vitamin D deficiency. Analysis of the clinical features, including biochemistry, by age categories clearly shows that the spectrum of clinical features varied by age and is similar to that described previously.6 7 Serum phosphate was lower in those who were hypocalcaemic, and this may simply be a response to the raised PTH and/or may reflect low phosphate intake. We note that our findings may be contrary to those of Robinson et al, who have previously reported raised phosphate in vitamin D deficient children with hypocalcaemia.6
Symptomatic vitamin D deficiency is a preventable cause of short-term but serious morbidity, which was successfully eradicated in the late 1970s through a public health programme that was targeted towards the South Asian population of Glasgow and which led to an increased uptake of vitamin D supplements by ethnic minority families.2 However, as our data show, this initiative seems to have floundered. The reasons for the re-emergence of symptomatic vitamin D deficiency require further exploration but may include a lack of sustained support for the public health programme through all the many changes in structure and management of community child health services during the years in question, as well as changes in patterns of immigration.
The economic costs of vitamin D deficiency not only include the burden on acute healthcare services but also the possibility of adverse long-term outcome in the deficient child. Recent estimations from observational studies and randomised controlled trials suggest that there may be real health economic benefit in raising the vitamin D level in all adults in western Europe.8 Although there may be a case for vitamin D supplementation of all children in Scotland, we believe that it is imperative that the first priority remains the eradication of profound, symptomatic vitamin D deficiency, and this will solve the acute problem. This requires improved education of the section of the population who are at highest risk and the healthcare staff who deliver care to this population. There is also a need for a robust system of monitoring profound vitamin D deficiency so that further information can be gathered about its epidemiology and the effectiveness of public health measures.
Acknowledgments
The authors would like to thank all the clinicians at Royal Hospital for Sick Children, Yorkhill, who considered the diagnosis of vitamin D deficiency in these children.
Footnotes
-
Competing interests None.
Provenance and peer review Not commissioned; externally peer reviewed.