Article Text

Abstract
Antibiotics represent the most widely prescribed therapeutic agents. The prevalence of drug prescription differs across age, with preschool children being most exposed to antibiotic drugs, especially in the community setting. A review with the aim to compare the profile of antibiotic drug prescription at the multinational, national and regional levels was performed. This overview of drug-utilisation studies found quantitative and qualitative differences in the antibiotic prescription profile between and within countries. Moreover, differences exist also at the local level and between prescribers. In general, second-choice antibiotic drugs (eg, cephalosporins) were more commonly prescribed in settings characterised by a high prevalence of antibiotic prescription. Geographical differences should be taken into account when monitoring antimicrobial drug resistance and when planning educational interventions for health professionals and parents with the aim to improve the rational use of antibiotic drugs.
Statistics from Altmetric.com
Introduction
Antibiotics represent the most widely prescribed therapeutic agents.1 The prevalence of antibiotic prescriptions differs across age, with preschool children being most exposed to antibiotic drugs.2 3 This is especially true in the community setting, where preschool children account for up to 33% of drug prescriptions.4
It is well established that antibacterial drugs prescribed to children are for the treatment of common paediatric conditions (colds, upper-respiratory-tract infections and bronchitis) that do not benefit from antibiotic therapy.5 6
It has been estimated that nearly 50% of antibiotic prescriptions for children given by primary care physicians are unnecessary.7
In view of this evidence of overuse/misuse of antibiotics, there is an increasing need to understand prescribing patterns in order to improve the appropriateness of prescribing, especially in primary care, where prescription rate and cost of antibiotics are important and essential variables of national care. In this context, drug-utilisation studies in children may be used to identify the major therapeutic problems in this population.
Several studies have monitored the antibiotic consumption in the general population. Most of these were performed by the European Surveillance of Antimicrobial Consumption (ESAC), a network of national surveillance systems that collects comparable and reliable data on antibiotic use.8
On the contrary, surveillance of antimicrobial consumption in the paediatric population is poor and not systematic.9
The aim of this overview is, therefore, to compare the profile of antibiotic drug prescription at the multinational, national and regional levels. A review of drug-utilisation studies concerning antibiotic prescriptions in the paediatric outpatient population published in the last 10 years was therefore performed.
Availability of antibiotic drugs
Antibiotics are defined as all substances belonging to the J01 main therapeutic group of the Anatomical Therapeutic Chemical (ATC) classification system.10
A total of 227 different antibiotic drugs (active substances) were listed in the WHO ATC/Defined Daily Dose (DDD) Index,10 60 of which (26%) were reported in the 2010–2011 edition of the British National Formulary for Children (BNF-C).
Only 31 antibiotics were included in the WHO Model List of Essential Medicines for Children, 21 of which were included in the core list and 10 in the complementary list.11
In the 2000–2009 period, a total of 10 new antibiotics were licensed or authorised by the European Medicines Agency with a centralised marketing authorisation or by the Food and Drug Administration, six of which were licensed for use in children in Europe and/or the USA: besifloxacin, cefditoren, ertapenem, linezolid, rifaximin and telithromycin. Antibiotics represented 2.5% and 5% of new drugs registered in Europe and USA, respectively, while antibiotics licensed for children represented 10% of the drugs with a paediatric authorisation. Only ertapenem was licensed in both continents (for use in children >3 months). Telithromycin was originally licensed in both Europe and the USA for the treatment of pharyngo-tonsillitis in children ≥12 years old, but this drug was subsequently withdrawn in the USA, because the risk/benefit profile was unfavourable. Besifloxacin (children >1 year), cefditoren (≥12 years), linezolid (all ages) and rifaximin (≥12 years) were licensed for use in children only in the USA.
Among the new antibiotics, only linezolid was reported in the BNF-C.
Problems associated with excessive antibiotic use
Considering the potential adverse drug reactions, the elevated direct costs and the increasing bacterial resistance, antibiotic overprescribing has a relevant impact on public health. The overuse and misuse of antibiotics, in fact, represent key factors in increasing bacterial resistance, and the link between antibiotic prescribing and bacterial resistance has been documented at the population level as well as in individual patients.12,–,14
Antibacterial resistance, in fact, currently represents a major health problem worldwide, with high social costs for communities and severe consequences (failure to respond to treatment, prolonged illness, increased length of hospitalisation and greater risk of complications and mortality).15 As a result, there could be a need of switch to second-line or third-line drugs or, for serious cases, to multidrug therapies, which are usually much more expensive and sometimes more toxic.12 Furthermore, the development of new antibiotics has stalled; pharmaceutical companies, in fact, began to invest in the development of new drugs for other, potentially high-profit conditions, such as chronic disease (with higher profits due to long-term, daily treatment) instead of infectious diseases.16 Consequently, approaches that preserve the efficacy of currently used antibiotics are needed.17 Several national public campaigns were performed in the last decade with the aim to promote careful use of antibiotics focusing on prescribers, the public or both. Most of these campaigns resulted in a reduction in outpatient antibiotic prescriptions. There is also some evidence on the reduction in bacterial resistance.18
However, the phenomenon of antibacterial resistance has a limited impact on the paediatric population, with the main exception of Streptococcus pneumoniae. The percentage of Streptococcus pneumoniae isolates that are penicillin (PNSP) and/or erythromycin non-susceptible (ENSP) varies across European countries. The highest values were reported in the southern and eastern European countries, in particular in France, Italy, Hungary, Turkey and Cyprus. France, Hungary, Cyprus and Turkey were characterised by a high prevalence (>25%) of both PNSP and ENSP.19
To face the increasing problem of antibacterial resistance, the rationalisation of antibiotic therapies, in qualitative and quantitative terms, must be a public health priority, involving all countries and fields of interest.
Even if bacterial resistance has a limited impact on the paediatric population, knowledge of the antibiotic prescribing patterns of physicians in the paediatric population is important, since children represent a major target for antibiotic prescription.
Monitoring antibiotic drug prescriptions: methodological considerations
Different indicators can be used to monitor drug prescriptions. Prevalence, expressed as the number of persons who received at least one prescription per 100 individuals in the population, is the indicator most commonly used to evaluate drug exposure. The DDD has been the most commonly used unit of measurement to quantify drug consumption, permitting a comparison of drug use between different settings. The DDD is the assumed average maintenance dose per day for a drug in its main indication for adults. In this regard, DDD cannot be used to measure drug consumption in children, since the dose recommendations for use in children vary according to age and body weight.10
For this reason, different indicators of drug consumption have been used, in particular the number of prescriptions, expressed as rate for the population or the treated patient.
Another measure is represented by the treatment course. One treatment course corresponds to all the prescriptions given to a single child within a predefined time period.20 However, this latter indicator is infrequently used owing to difficulties in application to large populations.
The type of indicator that can be used also depends on the data source. For example, it is possible to estimate the drug prescription prevalence in the population when evaluating prescription databases, but not when analysing data collected by primary care physicians, since the information collected concerns only children seen by the physicians. Also, in the analysis of wholesale data (as done in the ESAC studies) it is not possible to estimate the antibiotic prescription prevalence. On the contrary, analyses of prescription databases may underestimate the actual use because drugs that are not reimbursed, that is, by the national health service, are not included.4
Differences between countries
An overview of the literature that took into account 20 drug-utilisation studies published between 2000 and 2005 found a wide, quantitative and qualitative intercountry variability of antibiotic prescriptions, with the identification of regional clusters in antibiotic consumption, especially for European countries.21
For the scope of this review, the above overview was updated, and papers published between 2006 and June 2010 were searched for in the MEDLINE and EMBASE databases, using the same strategy (drug utilisation/prescriptions/pharmacoepidemiology; child/infant/adolescent; antibacterial agents/antibiotic agents). Studies that only evaluated the prescribing of antibiotics in the outpatient paediatric population were included, while studies that focused only on one antibiotic class and/or one disease were excluded. In order to analyse a homogeneous sample, studies evaluating data collected before 2000 were also excluded.
In all, 15 pertinent papers including comparable data (prevalence and/or prescription rate) were identified,20 22,–,35 two of which concerned the preschool population only.30 35
A total of eight countries were involved in the studies: Italy (five studies), Canada (three), the USA and The Netherlands (two studies each), Denmark, the UK, Sweden and Croatia (one study).
Table 1 reports the results of the most comparable studies, on the basis of the observation period (the most recent study for each country was selected), age groups and data source.
Characteristics of published studies evaluating antibiotic-drug prescribing
Italy and Canada were countries with the highest paediatric antibiotic prescription rates, and in contrast, northern EU countries (The Netherlands and UK) had significantly lower rates. The prevalence in Italy is nearly fourfold higher than in the UK (52% vs 14%, respectively), and the prescription rate is fourfold higher than in Denmark and The Netherlands (1.3 vs 0.3 prescriptions/person/year).
Qualitative differences also exist, suggesting different prescribing attitudes between countries. Data concerning the distribution of prescriptions by antibiotic class were reported for Italy, The Netherlands, Canada and Denmark (figure 1). Penicillins were the most prescribed antibiotics and represented varying rates of antibiotic prescriptions, from 39% in Italy to 89% in Denmark. Cephalosporins were the second class in Italy (39% of prescriptions) and the third in Canada (15%), while they were hardly prescribed in The Netherlands and in Denmark. Macrolides covered different rates of antibiotic prescriptions, from 11% in Denmark to 25% in Canada.
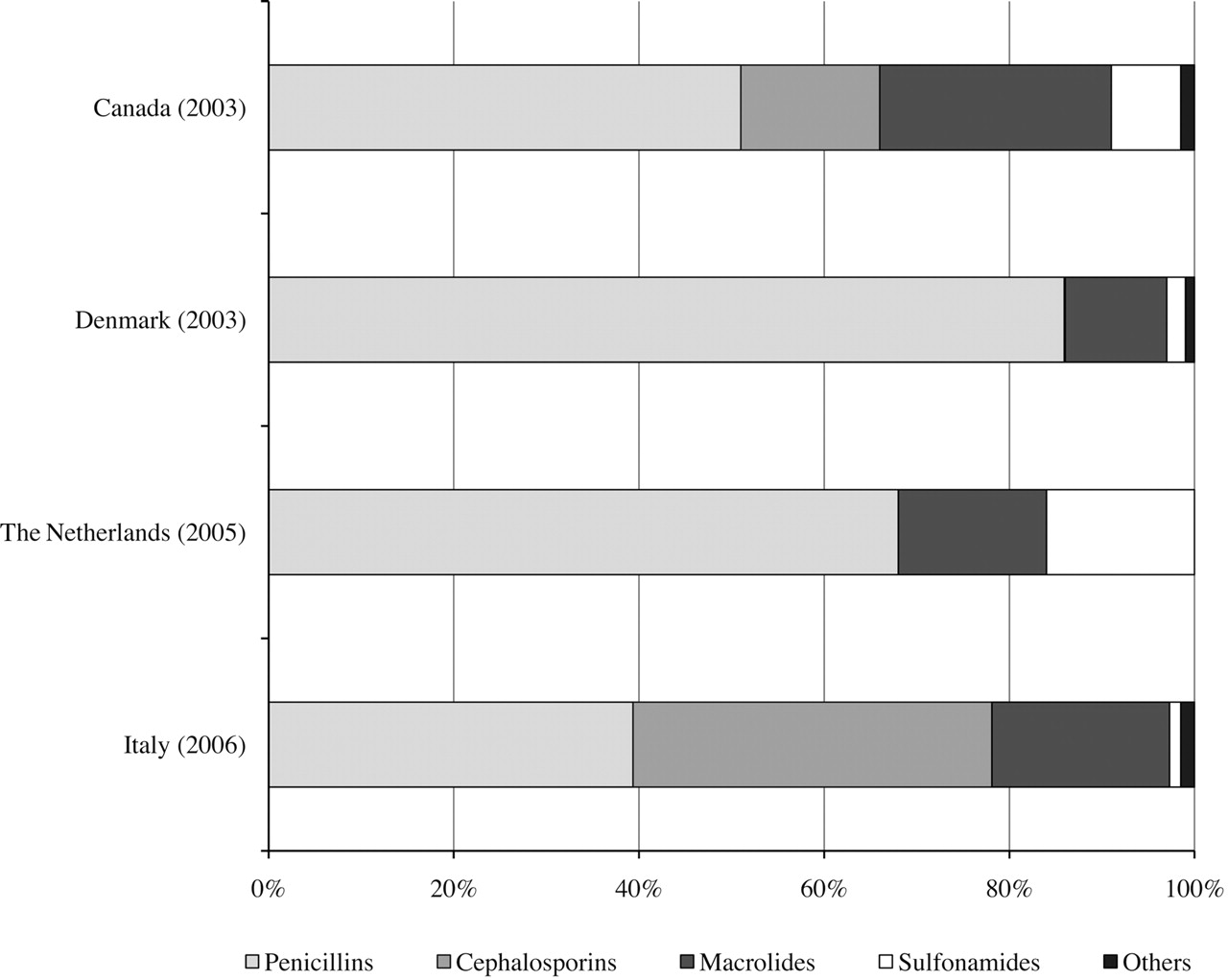
Percentage distribution (percentage of total prescriptions) of the most prescribed antibiotic classes.
Only a few studies reported the most frequently prescribed antibiotics, with data from Italy, The Netherlands and Canada. Four drugs (amoxicillin+clavulanic acid, amoxicillin, clarithromycin and azithromycin) were among the 10 leading drugs in all three countries. A total of 14 drugs covered the 10 most used antibiotics in the countries considered, representing 94% of total antibiotic prescriptions in Italy and The Netherlands. Amoxicillin was the leading drug in The Netherlands and Canada, while amoxicillin plus clavulanate was the most prescribed in Italy. On the other hand, the combination of amoxicillin and clavulanate was infrequently used in Canada. Clarithromycin and azithromycin were both widely used everywhere, but in variable amounts in each country analysed (table 2). Finally, the use of some antibiotics is limited to a single country: cefaclor is widely prescribed in Italy and Canada, while it is rarely prescribed in The Netherlands. Pheneticillin, an oral, narrow-spectrum penicillin, is frequently prescribed in The Netherlands, ceftriaxone in Italy, and gentamycin and cephalexin in Canada.
Ten most prescribed antibiotic drugs in Canada, The Netherlands and Italy
The different national policies concerning antibiotic-drug prescribing, along with other factors (eg, sociocultural and economic determinants, prescribing attitudes) may in part explain these quantitative and qualitative differences.36
Within-country differences: the case of Italy
Italian healthcare is provided free or at a nominal charge through a network of 148 local health units (LHUs) covering an average of 290 000 citizens. A national formulary is available in which drugs are categorised into two classes: class A includes essential drugs that patients do not have to pay for, and class C contains drugs not covered by the National Health Service. Nearly all antibiotics are free of charge; while parenteral antibiotics are reimbursed for severe infections only.
A total of 72 antibiotics (active substances) were prescribed to Italian outpatient children (78% of the antibiotics marketed in Italy), 22 of which were cephalosporins, 13 penicillins and 12 macrolides. Only 38 drugs (53%) were reported in the BNF-C.
Taking into account data collected in the 2005–2007 period in four Italian regions (Lombardy and Veneto, in northern Italy, and Lazio and Umbria, in central Italy), the prevalence of antibiotics at the regional level ranged from 41% in Lazio to 54% in Umbria, while at the LHU level it ranged between 32% and 60%.22 28 37 38
In a multiregional study, the prevalence of antibiotics at the LHU level ranged between 39.5% and 61.1%,22 while in the Lombardy region the prevalence of antibiotic drug prescriptions ranged from 32.8% in Milan to 49.3% in Brescia. The place of residence was identified as a key determinant of receiving an antibiotic prescription, independent of gender and age.28
Variability was also identified at the healthcare district level. In the 108 health districts of the Lombardy region, the prevalence of antibiotics ranged between 28.8% and 55.3%.
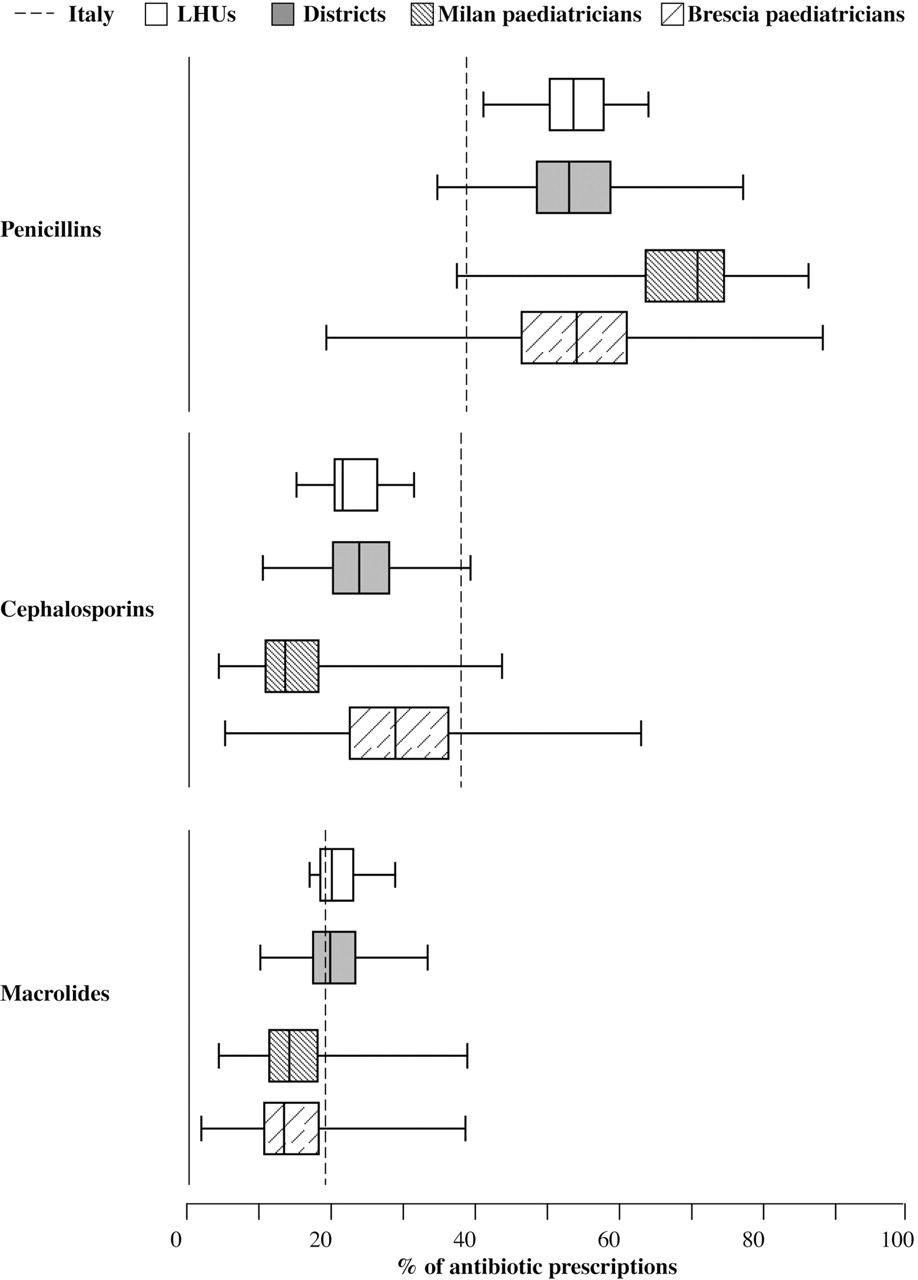
Qualitative intraregional differences also exist in the Lombardy region. Penicillins were the most prescribed antibiotics and represented 41–64% of antibiotic prescriptions. The proportion of antibiotic prescriptions covered by cephalosporins ranged between 15% and 32%, and that of macrolides ranged between 17% and 29%. Even wider differences were found at the district level (figure 2).
{kind=link}
{kind=link}
From country to prescriber: percentage distribution of prescriptions by antibiotic class at different levels (Italy, Lombardy local health unit (LHUs), Lombardy health districts, Milan and Brescia paediatricians). Data are reported using a box-whisker plot (minimum; 25th percentile; median; 75th percentile; maximum).
Taking into account the two Lombardy LHUs with the lowest and highest antibiotic prescription prevalence (Milan and Brescia), it should be noted that in Milan, penicillins covered 64% of antibiotic prescriptions, cephalosporins 15% and macrolides 18%. On the contrary, in Brescia, penicillins covered 50% of antibiotic prescriptions, cephalosporins 28% and macrolides 18%.
The ratio of children receiving one or more prescriptions for penicillins (first- choice antibiotics for the most common childhood infections) to children receiving one or more prescriptions for cephalosporins (second-choice antibiotics) was 3.5 in Milan and 1.6 in Brescia. These findings seem consistent with the results of international studies, with low-prescription settings more commonly using narrower-spectrum antibiotics compared with high-prescribing settings.1 9
At the regional and local levels, the prescription rate of antibiotics was independent of the health status of the population. In this regard, it is interesting to note that the paediatric hospitalisation rates in Milan and Brescia were very similar (8.7% and 8.9%, respectively), despite the wide differences in antibiotic prescription profile.28
Role of the prescriber
A total of 66 antibiotics were prescribed to the Lombardy region's paediatric population. The median number of antibiotics prescribed by each family paediatrician was 16 (range 9–32; IQR 15–18); in particular, each paediatrician prescribed a median number of seven different cephalosporins.
However, only 15 antibiotics (23%) were prescribed by at least 50% of the paediatricians. A total of eight antibiotics were prescribed by 90% or more paediatricians: amoxicillin+clavulanic acid, amoxicillin, clarithromycin, cefaclor, azithromycin, cefixime, ceftibuten and cefpodoxime. In all, 95% of the paediatricians prescribed all four of the most prescribed cephalosporins.39
Only four (amoxicillin, amoxicillin+clavulanic acid, azithromycin and ceftriaxone) out of the 15 antibiotics prescribed by at least 50% of the paediatricians were included in the WHO Model List of Essential Medicines for Children. These data suggest that a plethora of antibiotics that are structurally very similar, with only minor pharmacological differences between them, were prescribed in Italy.
The differences observed in antibiotic prescriptions at the LHU level can be observed also between prescribers. Paediatricians in Milan prescribed penicillins more frequently than their colleagues in Brescia (median 71% vs 55% of the overall antibiotic prescriptions, respectively). On the contrary, in Brescia, cephalosporins were more commonly prescribed (29% vs 14%) (figure 2).
The average ratio of children treated with penicillins/children treated with cephalosporins by paediatricians in the Milan LHU was 4.7 (median 4.1, IQR 3.0–5.8), while the average ratio penicillin/cephalosporin treated children in Brescia was 1.9 (median 1.7, IQR 1.2–2.2).
These findings support the hypothesis that the different prescribing attitudes between physicians may play a major role in determining differences in antibiotic prescribing.
In some countries, children can be cared for by family paediatricians or primary care physicians.
In Italy, children are assigned to a paediatrician until they are 6 years old; afterwards, the parents can choose to remain with that paediatrician until the child is 14 years old or to register the child with a general practitioner. All adolescents over 14 years of age are assigned to a general practitioner.
According to some international studies, drug prescriptions are influenced by the type of prescriber physician. In fact, a more common inappropriate use of antibiotics was observed among primary care physicians than family paediatricians in three international studies.40,–,42
In the Lombardy region, no differences were observed in the prevalence of antibiotic prescribing in children cared for by family paediatricians compared with children cared for by primary care physicians. However, differences were observed in the antibiotic classes prescribed. The prevalence of penicillins was higher in children cared for by family paediatricians (64.5% vs 54.2%), while the prevalence of macrolides and cephalosporins was higher in children cared for by primary care physicians (32.9% vs 28.3%, and 32.2% vs 26.6%, respectively).43
Conclusions
Quantitative and qualitative differences exist in the antibiotic-drug prescriptions to children at the multinational, national, regional and local levels.
Geographical differences in antibiotic use depend on several factors: the existing healthcare systems, which influence drug regulation and the national pharmaceutical market's structure, physicians' attitudes (ie, diagnostic uncertainty, especially for the youngest, or differences in diagnostic labelling, time or market pressure), sociocultural and economic determinants related to patients/parents (ie, patient's general condition or socioeconomic status).15 44
These differences should be taken into account when monitoring antimicrobial drug resistance and planning educational interventions for health professionals and parents with the aim to improve the rational use of antibiotic drugs. The availability of local, evidence-based therapeutic protocols shared by healthcare professionals may be useful in reducing antibiotic overprescribing.45
Finally, in order to implement programmes to control antibiotic resistance, prospective collaborative pharmacoepidemiological studies to collect valid and comparable data on antibiotic use patterns in general practice are necessary.
Acknowledgments
The authors would like to acknowledge M Sequi and F Fortinguerra for their support.
References
Footnotes
-
Competing interests None.
-
Provenance and peer review Commissioned; externally peer reviewed.