Article Text

Abstract
In order to assess the extent to which children in the UK will follow the UK-WHO head circumference standard, the authors used head circumference data from the Southampton Women's Survey (n=3159) and the Avon Longitudinal Study of Parents and Children (n=15 208) in children aged 0–36 months, converted into z-scores using both the UK-WHO and UK1990 references. Rapid head growth was defined as crossing upwards through two major centile bands (1.33 SD). The UK-WHO standard identified many more infants with heads above the 98th centile than to the UK1990 reference (UK-WHO: 6–16% of infants at various ages; UK1990: 1–4%). Rapid head growth in the first 6–9 months was also much more common using the UK-WHO standard (UK-WHO: 14.6–15.3%; UK1990: 4.8–5.1%). Practitioners should be aware of these findings to avoid unnecessary referrals.
Statistics from Altmetric.com
Background
New UK-WHO growth charts were launched in 2009. They incorporate the new WHO 2006 Growth Standards from age 2 weeks to 4 years, combined with recalculated birth data from the British 1990 growth reference.1 The charts include UK-WHO head circumference standards for 2 weeks to 2 years of age published in April 2007.2 The applicability of the WHO 2006 weight and length standard for growth monitoring in the UK has already been explored3 but not the head circumference standard, due to its later publication date. We thus set out to assess the applicability of the new UK-WHO head circumference reference to British children, using data from two UK population-based studies.
Methods
Populations
Southampton Women's Survey
The Southampton Women's Survey (SWS) followed women aged 20–34 years through pregnancy and their infants are currently being followed through childhood.4 Infants born before 37 completed weeks' gestation were excluded. Maximal occipitofrontal circumference (OFC) was measured three times and averaged. After birth blank tapes were used, marked and read off against a fixed rule. Printed cloth tapes were used for infants and children. Interobserver variation studies were conducted regularly to maintain consistency of measurements.
Avon Longitudinal Study of Parents and Children
The Avon Longitudinal Study of Parents and Children (ALSPAC) is a prospective study (http://www.alspac.bris.ac.uk) that enrolled pregnant women living in the former County of Avon. OFC measurements routinely collected by health visitors were extracted from the local child health database.
▶ UK children closely match the WHO standards for length, but the match for head circumference has not been assessed.
▶ New UK-WHO charts now include the WHO standard for head circumference.
▶ Children from two population-based UK studies have larger heads than the WHO standard and commonly cross centile spaces upwards.
▶ All head circumference references show a variable fit to UK, which could lead to children being spuriously labelled as having abnormal head growth.
Analysis
All head circumference data were converted into z-scores using both the earlier UK1990 growth references5 and the new UK-WHO reference, using the LMS growth package.6 The proportions in each cohort below the 2nd centile (equivalent to z-score <−2) and above the 98th centile (>+2) for each reference were identified. Changes in z-score in each child were calculated between birth and 6 months, and 6 to 12 months for the SWS, and between 6 weeks and 9 months, and 9 to 18 months for ALSPAC. Children crossing up or down through more than two major centile bands (equivalent to ±1.33 z-scores) were identified. In the SWS, mean head circumference was additionally compared to the WHO birth data, the Tanner and Whitehouse reference7 and the US standard (CDC)8 using the LMS growth program.
Results
Head circumference data were available in up to 1819 children in the SWS, and in up to 14 091 children in ALSPAC (table 1). For both cohorts, mean z-scores calculated compared to the UK-WHO standard were markedly higher at all ages compared to the UK1990 reference (table 2). Accordingly, compared to the UK-WHO standard, a large proportion of children had heads above the 98th centile from age 6 months onwards and very few had heads below the 2nd centile. Compared to the UK1990 reference, mean z-scores declined gradually from birth.
Mean (SD) head circumferences by sex and age in the Southampton Women's Survey (SWS) and Avon Longitudinal Study of Parents and Children (ALSPAC) birth cohorts compared to the UK-WHO or UK1990 references
Prevalence of head circumferences <2nd centile or >98th centile and prevalence of extreme centiles in the Southampton Women's Survey (SWS) and Avon Longitudinal Study of Parents and Children (ALSPAC) birth cohorts compared to the UK-WHO or UK1990 references
When the UK-WHO standard was used, as many as 15% children crossed upwards through two major centile bands between birth and 6 months, while with the UK1990 reference, up to 14.5% crossed downwards through two centile spaces between 6 weeks and 9 months (table 2). In the SWS there was little centile crossing in either direction after age 6 months, but in ALSPAC a substantial proportion showed either upward or downward centile crossing between 9 and 18 months.
In the SWS, the 3% of infants (n=60) of South Asian origin had smaller head circumferences at birth (mean, 95% CI z-score: −0.28, −0.54 to 0.02) than white children (0.48, 0.43 to 0.53) (p<0.001) and this difference persisted, for example, the mean South Asian z-score at age 12 months was 0.28 (0.02 to 0.54), while that for white children was 0.96 (0.91 to 1.0) (p<0.001).
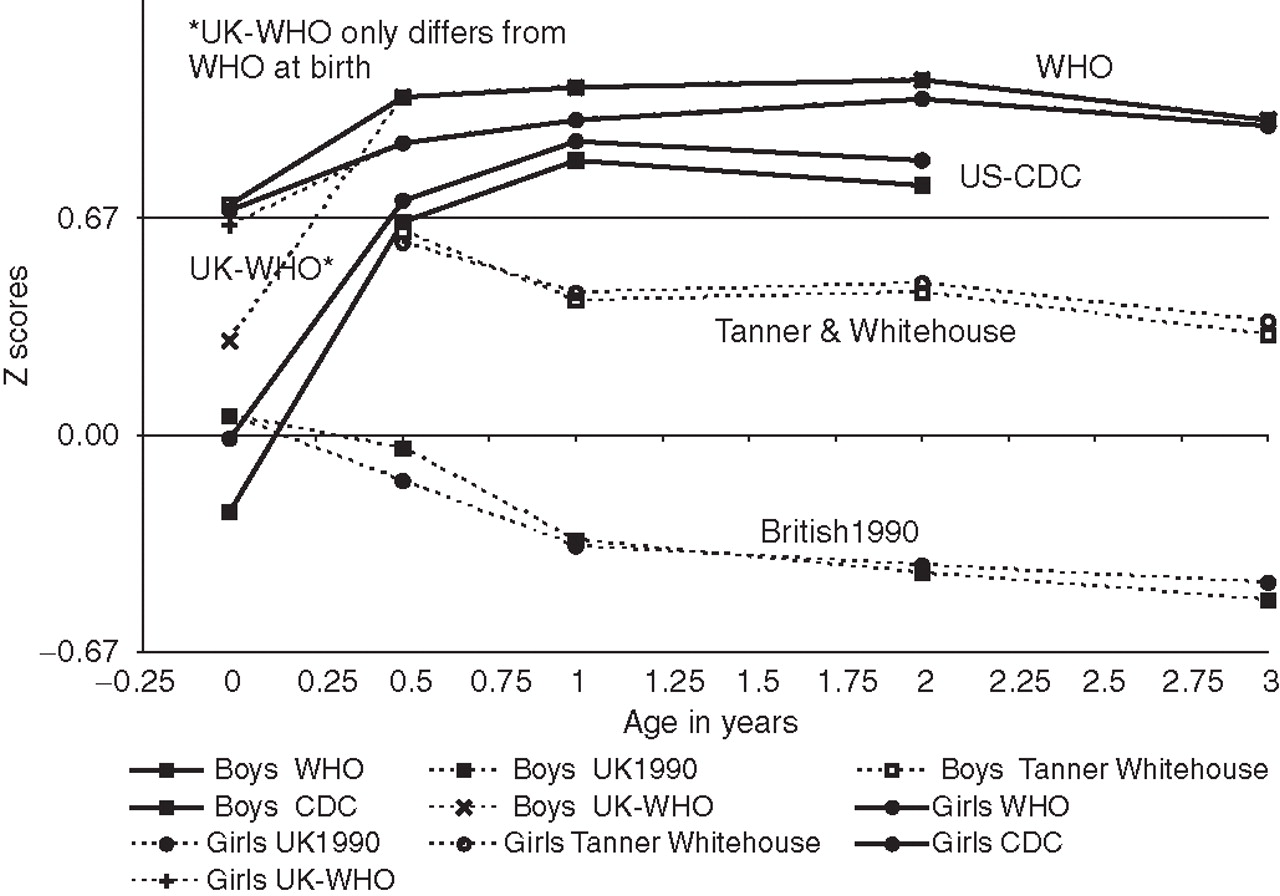
The mean SWS head circumference z-scores according to UK1990, UK-WHO, WHO 2006 (ie, using WHO 2006 birth data), Tanner and Whitehouse and CDC references all demonstrated markedly differing growth patterns over time (figure 1).

{kind=link}
Mean head circumference z-scores by age and sex, in the SWS birth cohort compared to UK1990 (British 1990), Tanner and Whitehouse, CDC (US-CDC), WHO and UK-WHO growth references.
Discussion
Our findings suggest that the head circumferences of British children will be large relative to the UK-WHO standard. On the other hand, the UK1990 reference may in the past have led to the overdiagnosis of small head size and slow head growth.
UK children show a good fit to the WHO 2006 standard for length,3 but Norwegian and Belgian children have already been described as having relatively large heads compared to the WHO standard.9 We found a substantial ethnic difference in head size, so it is feasible that, unlike length, OFC does vary with ethnicity. In contrast to standard UK practice, which is to record the largest head circumference, the WHO used a different measurement technique, where the tape was drawn tight rather than loosely applied and was anchored above the eyebrows, which is not always the fullest part of the head.10 Whether these differences in measurement techniques are sufficient to explain the difference observed, which are equivalent to more than 1 cm at age 1 year, is not clear. Whether the basis of the difference between UK and WHO growth study children is biological or methodological, recognising such differences is still important.
It is centile crossing rather than head size alone that usually signals concern, particularly about possible hydrocephalus,11 but the prevalence of centile crossing has been little studied previously. One US study found that 5–10% of infants crossed two major centile lines (roughly 1 SD) upwards or downwards up to 6 months, but rarely thereafter.12 The higher prevalence of early infancy head centile crossing could partly reflect the difficulties of obtaining a reliable measurement of head circumference around birth. In the SWS, with measurements by research staff, there was little centile crossing after the age of 6 months, as in the study above.12 In ALSPAC where data were collected by health visitors as part of routine care, a significant proportion also crossed centiles upwards or downwards after the age of 9 months. It is likely that these later infancy shifts in ALSPAC reflect higher levels of measurement error, as two imprecise measurements in opposite directions can easily produce an artefactual centile shift. The ALSPAC results indicate the actual prevalence likely to be seen in routine clinical practise. Many clinicians assessing a child's head size also compare them to the parents' head circumferences, using the latest centiles on the children's chart as an adult reference. However, the two references available for this purpose also differ markedly and it is not clear which best represents average adult head size.13
In contrast to the UK-WHO reference, the UK1990 reference identified an excess of children with small heads. This finding is in keeping with a previous report that 60% of children referred with head circumferences crossing below the 2nd UK1990 centile had no identifiable pathology.14
Conclusions
With the change from UK1990 to UK-WHO charts, it will become much more unusual to find infants with head circumferences below the 2nd centile and such infants should probably be investigated further, particularly if there is also downward centile crossing or slow neurodevelopmental progress. In contrast, head circumferences above the 98th centile and upward crossing through two centile spaces, will become substantially more common, so it will be important to look for other indicative signs or symptoms before deciding whether referral is required.
Acknowledgments
The authors are grateful to Tim Cole and David Elliman for their comments on this paper. This analysis would not have been possible without the women and children of Southampton who took part in the SWS, or all the ALSPAC families; the midwives for their help in recruiting; the SWS Study Group for their work in planning, collecting and processing the data and the entire ALSPAC team, which includes interviewers, computer and laboratory technicians, clerical workers, research scientists, volunteers, managers, receptionists and nurses.
Footnotes
-
Funding These components of the SWS were supported by the Medical Research Council, the University of Southampton, the British Heart Foundation and the Dunhill Medical Trust. Core support for ALSPAC was provided by the UK Medical Research Council, the Wellcome Trust and the University of Bristol.
-
Competing interests CW and AW are both member of the RCPCH growth chart design group and were closely involved in producing the new UK-WHO growth charts. CW also undertook a brief consultancy for WHO regarding the construction of their velocity standard. Otherwise, none of the authors have anything to declare.
-
Ethics approval This study was conducted with the approval of the Southampton and South West Hampshire Local Research Ethics Committee (SWS) and ALSPAC Law and Ethics Committee and Local Research Ethics Committees.
-
Provenance and peer review Not commissioned; externally peer reviewed.