Article Text

Abstract
Objectives Adolescent obesity is linked to metabolic and cardiovascular risk, but its associations with adolescents' experienced health and morbidity are less clear. Morbidities experienced by overweight/obese adolescents and associations between morbidities and timing of overweight/obesity were examined.
Methods Data were from the Health of Young Victorians Study (HOYVS; 1997, 2000, 2005), a school-based longitudinal study. Outcomes were blood pressure, health status (Pediatric Quality of Life Inventory 4.0 (PedsQL), global health), mental health (Strengths and Difficulties Questionnaire), psychological distress (Kessler-10), physical symptoms, sleep, asthma, dieting, and healthcare needs and visits. Regression methods assessed associations with body mass index status and timing of overweight/obesity.
Results Of the 923 adolescents (20.2% overweight, 6.1% obese), 63.5% were classified as “never” overweight/obese, 8.5% as “childhood only”, 7.3% as “adolescence only” and 20.8% as “persistent”. Compared to non-overweight, current obesity was associated with lower PedsQL physical summary scores (mean −6.58, 95% CI −9.52 to −3.63) and good/fair/poor global health (OR 3.52, 95% CI 1.95 to 6.36), hypertension (systolic 8.86, 95% CI 4.70 to 16.71; diastolic 5.29, 95% CI 2.74 to 10.20) and dieting (OR 5.79, 95% CI 3.28 to 10.23), with intermediate associations for overweight. Associations with psychosocial morbidity were weaker and inconsistent and there were few associations with health symptoms and problems. Only dieting (OR 2.30, 95% CI 1.36 to 3.89) was associated with resolved childhood overweight/obesity.
Conclusions Despite poorer overall health, overweight/obese adolescents were not more likely to report specific problems that might prompt health intervention. Morbidity was mainly associated with concurrent, rather than earlier, overweight/obesity.
Statistics from Altmetric.com
Introduction
There is surprisingly little information about the health of overweight and obese adolescents as experienced by the adolescents themselves or observed by their parents. In cross-sectional clinical1 and, to a lesser extent, community2 3 samples, social, emotional and physical health is generally poorer in obese than in non-obese adolescents. However, little is known about the prevalence of more specific health issues which, if present, might drive both perceptions of poorer general health and healthcare utilisation.4 5 If specific health issues are absent, there may be little incentive to modify behaviours, so that symptom-free overweight adolescents may not act to reduce their long-term risk for adverse adult outcomes.
What is already known about this topic
Surprisingly little has been reported about the health of overweight and obese adolescents as experienced by the adolescents themselves or observed by their parents.
It is also not known whether health issues are more common in teens with long-standing overweight/obesity, or resolve when childhood obesity resolves.
What this study adds
Overweight/obese adolescents experience poorer physical health than their non-overweight peers but do not report specific health problems that might prompt intervention to reduce their body mass index.
Many adverse health and psychological effects of childhood obesity could be reversed if the obesity were treated before adolescence.
Regarding physical health, adolescent obesity is clearly associated with higher blood pressure, higher fasting insulin, adverse lipid profiles and abnormal glucose tolerance tests, which are usually all asymptomatic at this age and detected only opportunistically or via surveillance. Obesity is believed to cause a range of more overt physical problems, with a recent systematic review citing symptoms such as heat intolerance, excessive sweating, intertrigo, heat rash, tiredness, shortness of breath on exercise, joint pain and headaches.6 Asthma has been weakly related to overweight/obesity in some, but not all, good-quality epidemiological studies,7 particularly those in which asthma is self-reported or clinically treated8 rather than more objectively assessed via lung function testing.
Suspected psychosocial impacts of adolescent obesity9 include dieting and eating disorders, as well as other mental health problems. However, the current literature is biased towards clinically obese samples in which the presence of a mental health problem may be the trigger for presentation. Population studies suggest that psychological well-being may in fact be well preserved in many overweight and obese children,10 11 with major determinants being prior psychopathology12 and severe obesity.13
No community study to our knowledge has investigated associations between body mass index (BMI) status and a wide range of both mental and physical health problems simultaneously in a population-ascertained cohort of adolescents. Therefore, the first aim of this paper was to determine the morbidities experienced by overweight and obese adolescents in a population sample, compared to their non-overweight peers. We hypothesised that the frequency of these problems would rise with increasing BMI status (ie, from non-overweight through overweight to the obese category).
A further question relates to whether any experienced health problems relate to the duration of an adolescent's obesity, or which symptoms (if any) are reversible in adolescents whose earlier overweight/obesity has resolved. This is important in the context of approaching obesity-related morbidities as curable or as problems that must be chronically managed. Therefore, our second aim was to assess whether the likelihood of adolescent health problems is increased by overweight/obesity in earlier childhood, independently of current BMI status.
Method
Design and sample
This study draws on the three waves (1997, 2000 and 2005) of the Health of Young Victorians Study (HOYVS). Sampling and methods have been reported previously.14 15 Briefly, 24 elementary schools were selected from across the state of Victoria, Australia (population 4.6 million in 1997), using a stratified two-stage random sampling design based on school education sector (government, Catholic or independent) and school class level. The baseline response rate for prep (first school year) through third grade students in 1997 was 83.2% (1943 of 2336 identified children; age range 5.0–10.7 years). The achieved sample mirrored Victorian census data for age distribution, sex, ethnicity (parental county of birth) and proportion of indigenous persons.
Children were resurveyed 3 years later when in grades 3 through 6 (HOYVS 2000) (age range 8.4–13.8 years; response rate 80.8% (1569 of 1943 children in 1997)) and then after a further 5 years when most were in grades 8 through 12 (HOYVS 2005, conducted September 2005 to December 2006). For HOYVS 2005, 960 parents agreed to participate again (58% of the 1662 located, 49% of the original 1943; mean age 15.9 years; age range 13.6–19.4 years). The main reasons for non-participation in HOYVS 2005 were adolescent not located (n=281), parental refusal (n=357) and parental consent not obtained (n=345). All waves were approved by the Royal Children's Hospital Ethics in Human Research Committee and the relevant education authorities and written parental informed consent was obtained. In 2005, adolescents also provided written informed consent.
Anthropometric measures (primary exposure)
Anthropometric measures were taken by trained field workers in each wave. Weight was measured in light clothing to the nearest 100 g using digital scales (Tanita, Tokyo, Japan, model 1597 in 1997 and 2000, model THD-646 in 2005). Height was measured to the nearest 0.1 cm using a portable rigid stadiometer (Invicta, Leicester, UK, model IPO955). Height was measured once in 1997 and 2000; in 2005, two height measurements were averaged and, where the two differed by more than 0.5 cm, the median of three measurements was used in analyses.
At each wave, BMI was calculated (kg/m2) and participants were classified as non-overweight, overweight or obese according to age- and gender-specific International Obesity TaskForce cut points.16 In the third wave, adolescents 19 years of age or older were classified as non-overweight (<25 kg/m2), overweight (≥25 and <30 kg/m2) or obese (≥30 kg/m2). Participants were further categorised according to timing and persistence of overweight/obesity as “never” (non-overweight at all three waves), “childhood only” (overweight/obese in 1997 and/or 2000, but not 2005), “adolescence only” (only overweight/obese in 2005) or “persistent” (overweight/obesity in one or both of the 1997 or 2000 waves, as well as in 2005).
Potential comorbidities (outcomes)
Potential comorbidities are summarised in table 1 and comprised parent- and adolescent-reported measures as well as measured blood pressure.
Measures of potential comorbidities (“outcomes”) of adolescent overweight/obesity
Socioeconomic and demographic variables (covariates)
Socioeconomic and demographic variables were the adolescent's sex (male/female), the adolescent's age in months and the Socio-Economic Indexes for Areas (SEIFA)17 disadvantage index for the most recent (2005) postcode of residence categorised into quintiles according to the distribution of the Victorian population. SEIFA values are standardised scores by geographical area compiled from 2001 census data to numerically summarise the social and economic conditions of Australia (national mean 1000, SD 100; higher values represent greater advantage). Due to missing data and lack of clear association with adolescent BMI status (table 2), mothers' highest completed educational level (collected in 1997) was not included as an additional covariate.
Characteristics by overall sample* and by body mass index status
Statistical analysis
Regarding morbidities experienced by overweight/obese adolescents (the cross-sectional 2005 analyses) (aim 1), adolescent BMI status was the categorical primary exposure. Regarding associations between morbidities and timing of overweight/obesity (the longitudinal analyses) (aim 2), the primary exposure was the four categories summarising the timing and persistence of overweight/obesity. Multivariable analyses were adjusted for adolescents' sex, adolescents' age in months and SEIFA disadvantage index.
Linear, logistic and proportional odds ordinal logistic regression models were used to model the continuous, binary and ordinal health outcomes, respectively, with each model including a single dependent variable (outcome). Results for the cross-sectional analyses (aim 1) present the effect estimates (mean differences for linear regression analyses; OR for logistic and ordinal logistic regression analyses) and 95% CI for overweight versus non-overweight and obese versus non-overweight, BMI status. Results for the longitudinal analyses (aim 2) are presented similarly, comparing health outcomes for the overweight/obese in the “childhood only”, “adolescence only” and “persistent” overweight/obesity categories with the “never” (reference) category.
Some outcomes were modestly skewed, so CIs for linear regression parameters were re-estimated using the bootstrap method; as the results were similar, the standard estimates are presented. One outcome, the healthcare utilisation variable, was sufficiently skewed that analysis on a log scale was preferred, with comparisons reported as geometric mean ratios. Using the Brant test, proportional odds assumptions were upheld for each of the ordinal logistic regression models. A non-parametric test for trend across ordered groups was used to assess trends in prevalence for each of the 16 physical symptoms across the three weight categories based on BMI.
Analyses were carried out with Stata release 10.0 (StataCorp, College Station, Texas, USA, 2007).
Results
Of the 960 adolescents with parental consent, 923 provided anthropometric as well as self-reported and/or parent-reported data in 2005 (467 boys and 456 girls). The mean age was 16.0 years (SD 1.2); 186 (20.2 %) were classified as overweight and 56 (6.1%) as obese. On the 1997 baseline characteristics, the retained cohort was similar to those lost to follow-up in terms of gender (50.6% vs 50.9% male; p=0.91) and SEIFA (1996) disadvantage index (1027.7 vs 1021.9; p=0.05). However, those retained were slightly younger (7.5 vs 7.7 years; p=0.004), had a lower baseline mean BMI z score (0.42 vs 0.60; p=0.001), and smaller proportions were categorised as overweight or obese at baseline (14.1% and 2.8%, respectively vs 17.0% and 7.7% respectively; p<0.001). Table 2 presents adolescent and family demographics for the 2005 sample overall and by BMI status.
Table 3 quantifies the strength of the cross-sectional associations between adolescent BMI status and the range of health outcomes, adjusted for the three covariates of age, sex and disadvantage quintile; the univariate findings (available from the authors) were very similar. Regarding physical health, PedsQL (Pediatric Quality of Life Inventory 4.0; table 1) physical summary scores fell and the proportions of adolescents with poorer global health rose with increasing BMI, as reported both by adolescents and their parents. Prevalence of systolic and diastolic hypertension also rose with higher BMI status.
Summary of each comorbidity, overall and by BMI status; adjusted measures of effect for morbidities by BMI status
Psychosocial measures (table 3) showed inconsistent relationships with BMI status. Parents of the obese subgroup (but not the adolescents themselves) reported poorer PedsQL psychosocial summary scores and adolescents reported slightly poorer behaviour scores on the Strengths and Difficulties Questionnaire (table 1) with rising BMI status; however, the prevalence of severe psychological distress on the Kessler-10 (table 1) was similar across the BMI categories. Concurrent dieting behaviour was strongly associated with rising BMI status.
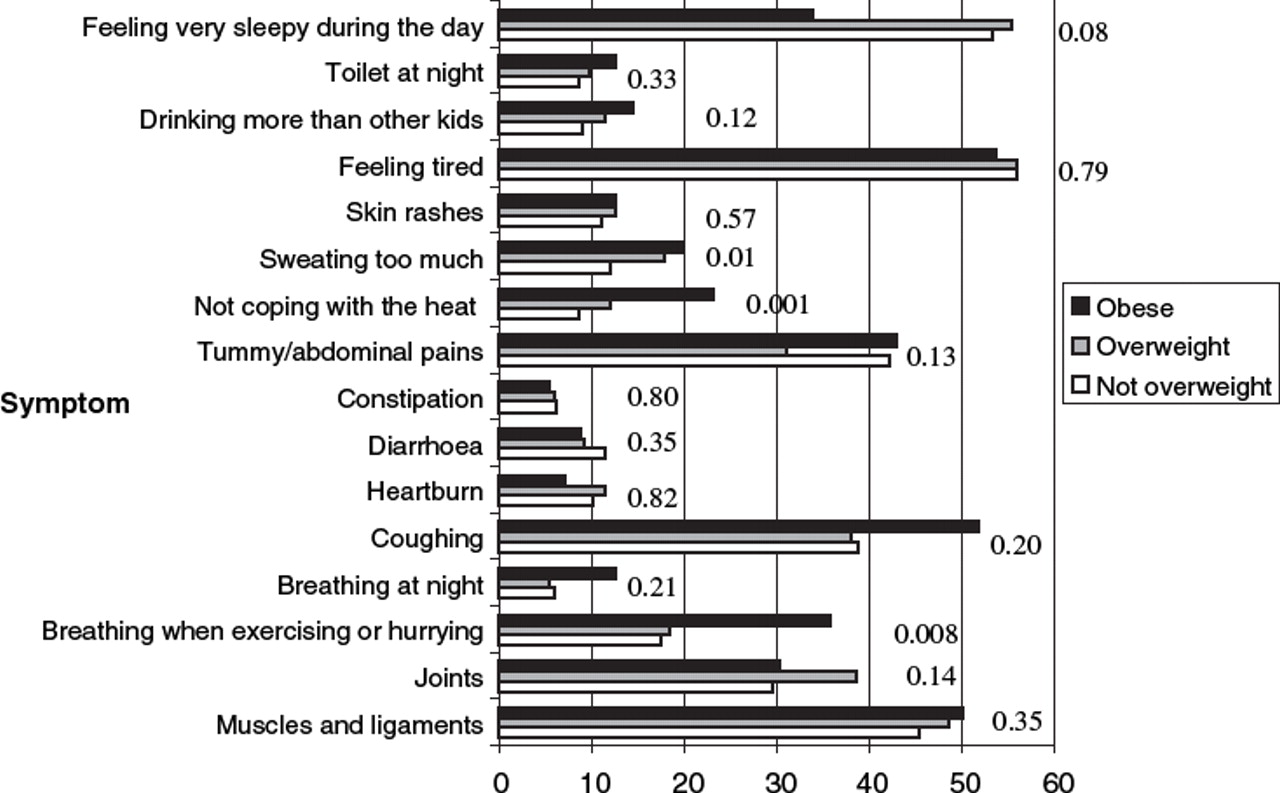
Although general physical symptoms, special healthcare needs and asthma requiring medication rose slightly with increasing BMI status, none reached statistical significance. The weak evidence (p=0.03) of an association between BMI and number of healthcare visits was mainly due to the overweight (geometric mean ratio 1.20, 95% CI 1.04 to 1.39) rather than the obese (0.90, 95% CI 0.70 to 1.15) group. Similarly, as seen in figure 1, there was little evidence of increasing prevalence of physical symptoms with increasing BMI status, except for three of the 16 symptoms (trouble breathing when exercising/hurrying, p=0.008; not coping with the heat, p=0.001; and sweating too much, p=0.01).
{kind=link}
Physical symptoms reported by adolescents according to body mass index status. p Values, obtained from a non-parametric test for trend, are shown.
Table 4 shows the associations between BMI status and health outcomes according to timing and persistence of overweight/obesity, drawing on the longitudinal data (aim 2). Overall, 516 (63.5%) children were categorised as “never” overweight/obese, 69 (8.5%) as “childhood only”, 59 (7.3%) as “adolescence only” and 169 (20.8%) as “persistent”. Where differences in adolescent health status were observed (hypertension, good/fair/poor health and lower PedsQL scores), those with “childhood only” obesity had only marginally increased risk, while those with persistent and “adolescent only” obesity were at increased risk compared to the never-obese. The only outcome that also showed clear associations with “childhood only” overweight/obesity was dieting (OR 2.30, 95% CI 1.36 to 3.89); however, the odds of dieting were even greater with concurrent adolescent overweight/obesity (“adolescence only”, OR 3.15, 95% CI 1.80 to 5.51; “persistent”, OR 4.18, 95% CI 2.86 to 6.11). No morbidity was associated solely with childhood overweight/obesity that had subsequently resolved.
Adjusted measures of effect for morbidities according to period of overweight/obesity, compared to “never overweight/obese”
Discussion
Overweight and obese adolescents were more likely than their non-overweight peers to experience poorer health, and systolic and diastolic hypertension and to engage in dieting behaviour. Poorer general physical functioning was more consistently and more markedly associated with rising BMI status than were psychosocial morbidity and distress. However, obese adolescents were not more likely to report specific health issues (eg, asthma and sleep, muscle and joint problems) that might prompt health intervention. Most morbidity was associated with current BMI; those whose childhood overweight/obesity had resolved did not report excess morbidity, with the exception of a doubling in the odds of dieting.
Strengths of the study include the population, rather than clinical, nature of the sample and its prospective design. Height and weight were directly measured on three occasions using standardised techniques and the prevalence of overweight and obesity mirrored that in other recent surveys.18 We specified a priori a wide range of common conditions, based on initial literature review and current clinical guidelines,6 for which it was reasonable to hypothesise a disproportionate excess in obese adolescents. A further strength was the inclusion of parallel adolescent self-reports and parent proxy-reports for three measures of adolescent health. Relationships with adolescent BMI status were very similar between parents and adolescents for each of these measures.
Limitations include potential bias introduced by the 50% loss to follow-up by the third wave, with a higher rate of baseline obesity in those lost. If these children subsequently experienced greater morbidity, we may have underestimated the true contribution of childhood obesity to morbidity in adolescence. Nonetheless, the prevalence of obesity in our adolescent cohort mirrored that recently reported in the Australian general population.18 As our primary aim was to describe perceived health, we did not sample blood or undertake imaging, which might have shown irreversible metabolic abnormalities in subjects whose overweight or obesity had resolved by adolescence. Although we used validated, widely used measures wherever possible, we relied on self-report of conditions such as asthma and physical health symptoms, noting, however, that self-perception of problems largely drives not only healthcare provision but also clinical guidelines.6 The number of obese adolescents at the third wave was not large, but nonetheless the findings were robust in terms of the strength and consistency of the observed associations between related measures, between parents and adolescents and (for the cross-sectional analyses, where the most literature exists) with other studies. Further, the conclusions did not alter when we repeated the analyses using Centers for Disease Control cut points, which classify more individuals as obese. Finally, healthcare utilisation was parent-reported rather than obtained from a state or national database.
We are not aware of previous population-based reports examining associations of adolescent overweight/obesity with such a wide range of health outcomes based on a published review of the literature. General physical impacts were more marked than specific physical or psychosocial problems. Australian19 and Swedish20 population studies support this finding well into early adulthood, with a clearer negative association between obesity and physical health than between obesity and mental health in obese 16–34-year olds and more marked mental health associations developing in older adults (35–64-year olds). Our study also supports others' findings that the general experience of obesity in the community2 3 is different from that of clinical populations,1 and that psychosocial morbidity in community studies particularly afflicts the most obese.20 21 Bell's recent report22 that a wide range of morbidities, including depression, increased across the BMI range in 6–13-year olds may have been influenced by nearly a third of the sample comprising treatment-seeking obese children.
The generally favourable outcome associated with childhood overweight/obesity that resolves by adolescence is a novel finding but is consistent with other recent lines of enquiry. One explanation may be that those whose overweight or obesity resolved were less overweight and healthier to begin with, but it is also now known that reversal of even morbid obesity reverses much morbidity and substantially improves health-related quality of life in adults.23 24 Second, childhood overweight/obesity in four British longitudinal cohorts was not associated with increased risk of fatal heart disease to middle age and beyond,25 26 whereas high adolescent BMI has been associated with 30–40% higher adult mortality.27 Finally, Viner and Cole recently showed that obesity in childhood that subsequently resolved on self-report was not associated with a range of self-reported physical, psychological and social outcomes in adulthood.28 Our similar findings for adolescents are strengthened by direct measures of anthropometry and blood pressure.
The finding that overweight/obesity at any age was associated with dieting is consistent with earlier studies.29 It is possible that dieting has actively contributed to the maintenance of a healthier weight in the 8% whose childhood overweight/obese resolved. Yet dieting is the major risk factor for adolescent eating disorders and it remains possible that the cost of healthier weight in this group is a continuing higher risk for anorexic and bulimic syndromes.30
Conclusions
High rates of overweight and obesity translate into generally lower adolescent physical health scores. However, overweight/obese adolescents are not more likely to report specific health complaints that might prompt them to see their doctor and neither hypertension nor dieting (the two specific problems that had striking associations with BMI status) typically present spontaneously unless extreme. Therefore, opportunistic community and/or primary care surveillance may be the only way to systematically detect important morbidities in this group. Obesity limited to childhood had little lasting impact on morbidity and the new Cochrane systematic review provides some evidence-based optimism that obesity can be treated effectively in younger children.31 This lends greater urgency to systematic attempts to manage and treat overweight in the preschool and primary school years to avert these consequences.
Acknowledgments
The authors acknowledge the contribution of all field workers who conducted the data collection across the three waves and especially Megan Mathers for managing HOYVS (2005) and assisting with the final preparation of this manuscript. The authors would like to particularly thank all the HOYVS participants and their parents.
References
Footnotes
-
Funding The third wave of the Health of Young Victorians Study was funded by Australian National Health and Medical Research Council (NHMRC) Project Grant 334303. Earlier waves were supported by the Victorian Department of Human Services, the National Heart Foundation, Murdoch Childrens Research Foundation and the Financial Markets Foundation for Children. MW is supported by an NHMRC Career Development Award, KH by an NHMRC/National Heart Foundation Postdoctoral Fellowship, GPC by an NHMRC Research Fellowship and EW by a VicHealth Public Health Research Fellowship. The researchers were independent of the funders and do not have any relevant financial interests in the manuscript. The funding organisations did not have a role in the design and conduct of the study; collection, management, analysis and interpretation of the data; or in the preparation, review, or approval of the manuscript.
-
Competing interests None.
-
Ethics approval This study was conducted with the approval of the Royal Children's Hospital Ethics in Human Research Committee.
Provenance and peer review Not commissioned; externally peer reviewed.
Patient consent Obtained.