Article Text

Abstract
Objective To determine the utility of a novel Paediatric Consultation Assessment Tool (PCAT).
Design Developed to measure clinicians' communication behaviour with children and their parents/guardian, PCAT was designed according to consensus guidelines and refined at a number of stages. Volunteer clinicians provided videotaped real consultations. Assessors were trained to score communication skills using PCAT, a novel rating scale.
Setting Eight UK paediatric units.
Participants 19 paediatricians collected video-recorded material; a second cohort of 17 clinicians rated the videos.
Main outcome measures Itemised and aggregated scores were analysed (means and 95% confidence intervals) to determine measurement characteristics and relationship to patient, consultation, clinician and assessor attributes; generalisability coefficient of aggregate score; factor analysis of items; comparison of scores between groups of patients, consultations, clinicians and assessors.
Results 188 complete consultations were analysed (median per doctor = 10). 3 videos marked by any trained assessor are needed to reliably (r>0.8) assess a doctor's triadic consultation skills using PCAT, 4 to assess communication with just children or parents. Performance maps to two factors – “clinical skills” and “communication behaviour”; clinicians score more highly on the former (mean (SD) 95% CI 0.52 (0.075)). There were significant differences in scores for the same skills applied to parent and child, especially between the ages of 2 and 10 years, and for information-sharing rather than relationshipbuilding skills (2-tailed significance <0.001).
Conclusions The PCAT appears to be reliable, valid and feasible for the assessment of triadic consultation skills by direct observation.
Statistics from Altmetric.com
Embedded in good medical practice and other models of professional activity, doctor–patient interactions are central to clinical practice.1 2 The General Medical Council's 0–18 years: guidance for all doctors emphasises the essential role of effective communication for the good care of children and young people.3
Common among the methods used to assess doctor–patient communication are patient and peer ratings. International research has shown peer ratings (multisource feedback) to be reliable, feasible and versatile for assessment of many attributes.4,–,6 Parent and adult patient rating tools have been developed for communication assessment.7 8
What is already known on this topic
Video observation is suitable for in-training assessment.
Validated tools for assessment of consultation skills have focused on two-way consultations with adult patients.
What this study adds
Reliable assessment of paediatric triadic consultation skills can be achieved by applying the Paediatric Consultation Assessment Tool to 2–3 cases.
Reliable, individual assessment of child-oriented and parent-oriented communication is also possible within 3-4 cases.
Training in paediatric communication skills should emphasise consulting with children themselves, and on information sharing rather than rapport building.
Some licensing bodies make use of direct observation, either live or via video/audio recordings, to measure doctor–patient interactions. Of these, video appears to have the greatest effect on behavioural response to feedback perhaps because one can personally review and learn from one's own behaviour. Many assessment instruments are used for evaluating dyadic consultation skills by direct observation.9,–,11 The Paediatric Consultation Assessment Tool (PCAT) has been developed to assess communication within three-way (triadic) paediatric consultations. The aim of this study was to test the validity, reliability and feasibility of PCAT in the secondary care setting.
Methods
PCAT design: assuring content validity
We designed PCAT as an itemised rating scale to simultaneously but separately rate doctor–parent and doctor–child communication. PCAT's content was configured according to consensus guidelines, a model of competencies for paediatric consultations, and the Calgary—Cambridge Referenced Observation Guide's scheme.12,–,14 We included items relating to:
Relationship building
Structuring the consultation
Initiating the consultation
Information-gathering behaviour
Information-giving behaviour and shared decision-making
Closure of the consultation
Following a nominal group exercise conducted using Royal College of Paediatrics and Child Health (RCPCH) college tutors and regional advisors in 2004, we included items assessing clinicians' clinical skills and judgement, as these were deemed “essential skills”.
PCAT's format (figs 1–4) was configured according to the best practice of developing health measurement scales, comprising:



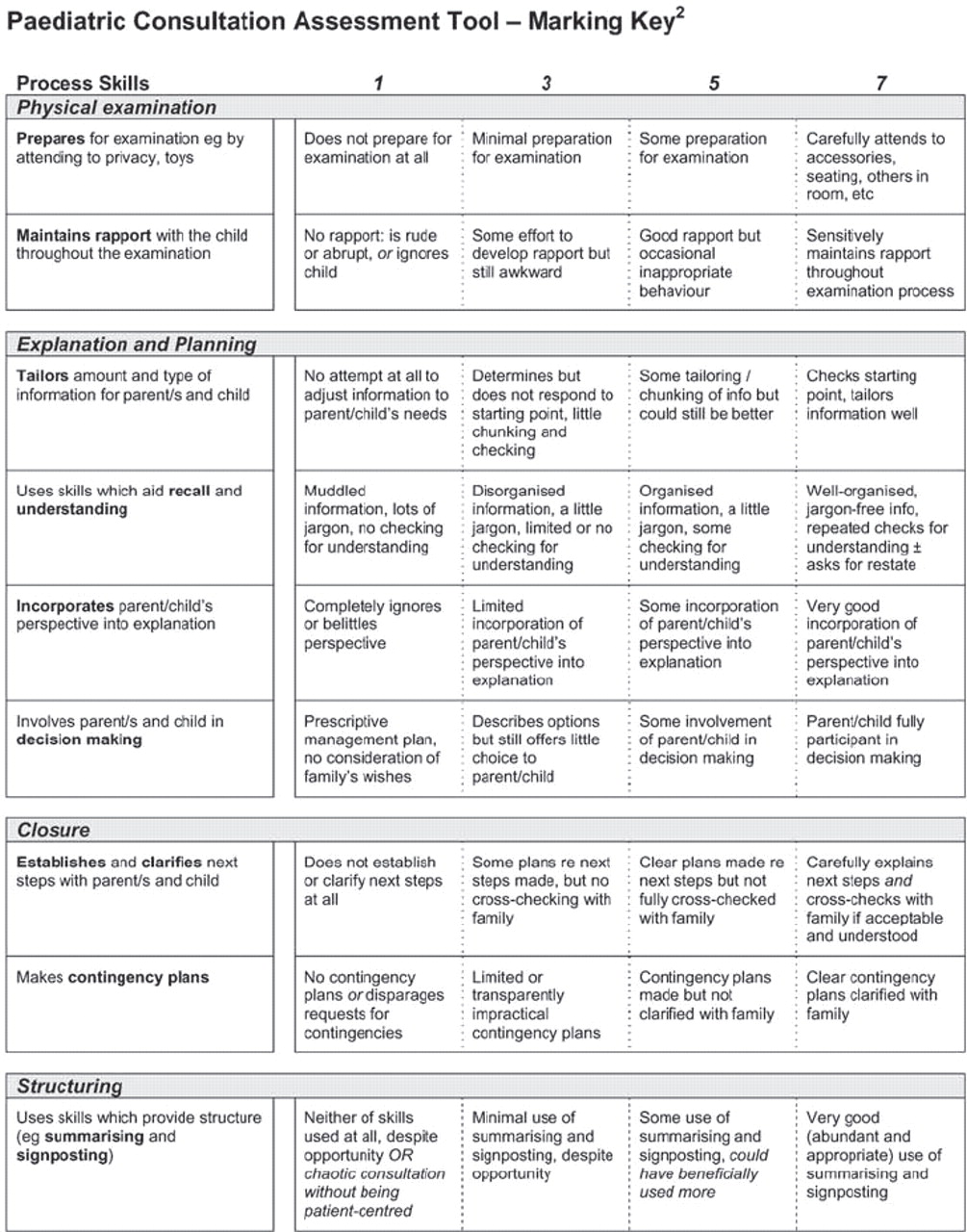
Assessment of skills (rather than consultation outcomes) and use of an itemised rating scale, for maximising educational potential through feedback.15
Sixteen scores related to themed groups of individual skills and two “global” scores.
A 7-point scale: an optimal number of response categories, feasible for use without substantial loss of information, marked using behaviourally anchored ratings.16,–,18
Space for comments/observations, for feedback.
PCAT was tested and refined through an iterative process at four time points. Four authors initially piloted the PCAT for face validity and scope using videotaped consultations. At this stage the number of items were determined. In a second exercise, RCPCH college tutors informally tested the potential for educational feedback and reliability; here, the number of response categories were optimised. At two further stages, paediatricians from centres involved in this study refined the PCAT's format into themed domains informed by discrete skills.
PCAT evaluation
To evaluate the utility of PCAT, we undertook a study to determine:
The feasibility of collecting video material
The reliability of the tool to assess paediatricians' consultation behaviour
Construct validity of the tool, by testing whether scoreswere:
Higher for items relating to clinical skills and judgement than communication skills. We hypothesised that a valid assessment tool would demonstrate such differences given that postgraduate paediatric training usually focuses on clinical rather than communication skills.
Higher for items relating to doctor–parent interaction compared with those relating to doctor–child interaction. We hypothesised that a valid assessment tool would demonstrate these differences given that none of our clinician samples had received specific child-oriented communication training.
Higher for adult-oriented items than respective child items, particularly information-sharing items. We hypothesised that a valid assessment tool might reveal such differences since observations of paediatricians' consultations suggest greater time is spent talking to children during the “affective” (relationship-building) stages of consultations, and less during information-sharing stages.19
Paediatric consultants and specialist registrars recorded videotaped consultations with patients and their families, in accordance with General Medical Council guidelines.20 With consent from parents and children, we recorded consultations from each clinician's out-patient practice, across a wide age (newborn–16 years) and case range.
A second cohort of paediatricians rated the video recordings, having been trained to use PCAT during standardised training sessions lasting 90–120 minutes. Sessions involved familiarisation with PCAT followed by benchmarking between markers using videotapes of consultations. Markers independently rated each videotape in “real time”. They were asked to judge for themselves whether to score items for communication with the child, based on the actual age of the child (supplied) and their assessment of the developmental stage of the child seen on videotape.
Multicentre ethical approval was obtained for this study.
Statistical analysis
For quantitative analysis, scores from PCAT's 16 items were combined to produce one aggregate score per consultation per assessor (AggregateO). Scores from five items (relationship building, initiating the session, gathering information, explanation/planning and closure with the adult) were combined to produce one “adult–aggregate” score (AggregateA) and six other items (relationship building, initiating the session, gathering information, physical examination, explanation/planning and closure with the child) combined to produce one “child–aggregate” score (AggregateC).
Reliability – the reliability coefficient (R) – the expression of reproducibility of “true” differences in performance between doctors given any consultation when assessed by any assessor – was determined using a generalisability (“G-study”) analysis in SPSS V.13.0. A fully nested design was used: “assessors nested within cases, nested within clinicians”. A “D-study” predicting the “number of consultations required for satisfactory reliability when assessed by any trained assessor” was determined using Microsoft Excel (2000).
Determination of construct validity by comparison of mean scores for groups of items
Principle components analysis was used to determine the relationships between item scores. Two factors accounted for 68% of variance of score: factor 1 (“communication behaviour”, 58% of variance) and factor 2 (‘‘clinical skills’’, 10% of variance). Highly correlated items which could be accounted for by either one of the two factors were aggregated.
Paired t tests were used to analyse the difference between the mean factor aggregate scores and between AggregateA and AggregateC.
Influence of covariates on score – we collected data about the following attributes:
Patient attributes
Age
Diagnoses
Co-attendants
Consultation attributes
Length
New or follow-up
Difficulty of consultation (as rated by observing assessor)
Within first or last three consultations on VHS tape We used paired and independent t tests to analyse the effect of the attributes on aggregate score, and linear regression analysis to determine the interdependency of covariates affecting score.
Results
Descriptive results
Ninety-three point eight per cent of families approached gave consent for video recording within their consultations, and of these 96.1% of recordings were of satisfactory quality (sound, image, completeness). The age range of patients was 5 weeks–15 years + 10 months. Nineteen clinicians recorded a median of 10 (range 8–14) satisfactory quality consultations onto videotape. The median number (range) of clinics needed to acquire the videos was two (1–7) per clinician.
Seventeen clinicians rated a total of 188 video recordings. One hundred and sixty-two consultations were rated in triplicate, 26 twice.
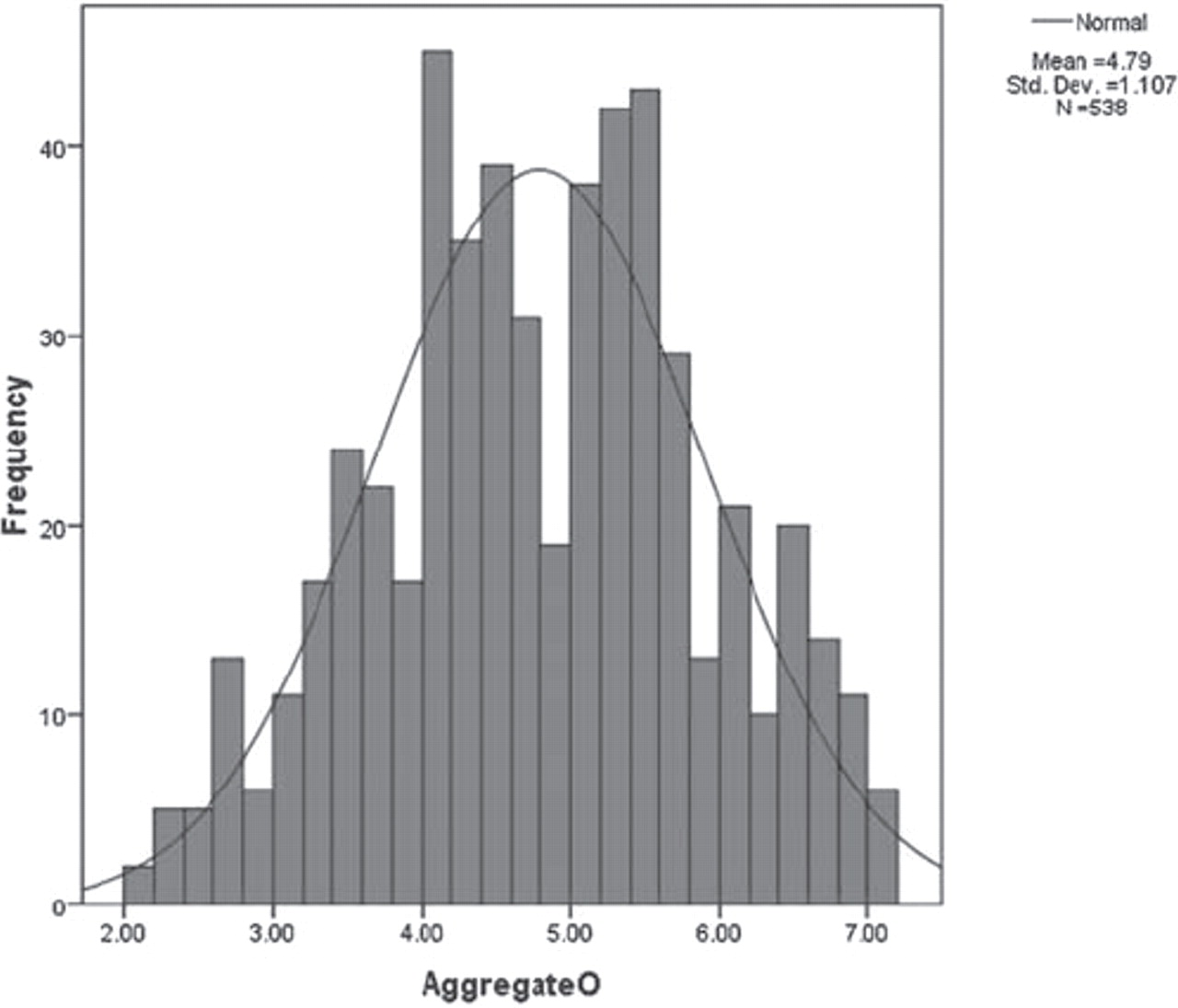
Figure 5 shows the distribution of 538 overall aggregate scores (‘‘AggregateO’’), which approximate to a normal distribution. The slight skew towards higher scores was not significantly greater than would be expected by chance. Mean (SE) overall aggregate score was 4.78 (0.05). Individual clinician's mean (SE) overall aggregate scores ranged from 3.01 (0.12) to 6.65 (0.05).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Distribution of overall aggregate scores (“AggregateO”).
Reliability analysis
Table 1 illustrates how many cases are needed for a reliable assessment of any clinician, when marked by any one trained assessor. For R>0.7, two cases are needed. For R>0.8, three cases are needed.
D study
Analysis of ‘‘adult’’-related items and ‘‘child’’-related items separately gave reliability coefficients of 0.70 and 0.66, respectively. The numbers of cases needed to reliably (R>0.7 or R>0.8, respectively) assess doctors' behaviour with children and parents separately are three or four, respectively, in each instance.
Tests of construct validity
Clinical and communication skills
The mean (SD) aggregate score (95% CI) for ‘‘clinical skills’’ was 0.520 (0.445 to 0.595) higher than that for ‘‘communication behaviour’’ (p<0.001). There was high correlation between pairs of scores (coefficient 0.73, p<0.001).
Comparison of communication with parents and children
Communication with parents scored more highly than that with children, although the two correlated highly (coefficient 0.76, p<0.001). The mean (SD; 95% CI) difference between AggregateA and AggregateC scores was 0.64 (0.08), p<0.001. When segregated by age, the difference between AggregateA and AggregateC scores was only significant when the patient was aged between 2 and 10 years (post hoc analysis of variance, p<0.001).
Scores were higher for all five specifically adult-oriented items (relationship building, initiating the session, gathering information, explanation and planning, closure) compared with the same child-oriented items. Differences between parent-oriented and child-oriented scores were significantly greater for three information-sharing items (gathering information, explanation and planning, closure), p<0.001 in all cases.
Influence of covariates on score
Patient and consultation attributes
Consultations judged to be of “average” or “difficult” complexity yielded higher aggregate scores (mean (SD; 95% CI) 0.25 (0.19)) than consultations considered to be “easy” (p<0.05). This association was accounted for by consultations attended by a non-parent (eg, grandparent, social worker) as well as a parent or guardian (p<0.001). Length of consultation and new/ follow-up status did not significantly influence score. Scores were no higher for the first or last three consultations recorded.
Discussion
Reliability
The PCAT offers the opportunity to assess doctors' consultation skills in the triadic setting by direct observation. Despite the complexity of triadic interactions, the tool appears highly reliable, requiring a very small number of cases for summative assessment of a doctor's consultation skills. This is true not only for assessment of overall communication performance (where three cases are needed for summative assessment), but also for that of communication with the child or parent alone (where four cases are needed). As the PCAT has been able to discriminate between performances of volunteer clinicians, it is likely to be able to do so among a random sample of doctors, to identify those who communicate poorly.
Feasibility
The high degree of reliability makes the assessment tool more feasible to administer than originally anticipated. Assuming a mean length of consultation of 15 minutes, assessors would need to observe 30–45 minutes of video-recorded material per trainee, or slightly more where focused evaluation of communication with just parent or child was required. Given high levels of consent and satisfactory recordings, as with our experience, it should be feasible to acquire sufficient video material from one or two outpatient clinics. Training time of 90–120 minutes adds to the practicability of implementing PCAT using clinicians as assessors. The use of web-based video streaming and online forms accessible to assessors would also improve feasibility and is already being utilised in other video-based assessments.
Validity
PCAT's content validity has been assured by its design using evidence-based communication theory. The tool has also demonstrated construct validity, scores being higher for clinical than communication skills, which is not surprising given that only two clinicians had received specific training in doctor-patient communication and no training in paediatric communication. The finding that scores were highest for communication with “parents” rather than children themselves, particularly for information-sharing items, also adds to construct validity. Observational research has shown children's involvement during information sharing within consultations to be very limited.19 21 22 That communication scores were only significantly higher for parents of children aged 2–10 years might reflect the fact that raters tended not to mark communication items for children under this age (other than ‘‘relationship building’’) and that doctors' communication with older children was genuinely better.
Limitations of this study
The sample of clinicians is small and is unlikely to represent the population of paediatricians as only volunteer clinicians submitted video-recorded material. Implementation of PCAT should be accompanied by re-evaluation of reliability in a random, non-voluntary population. A larger sample would enable further meaningful analysis of communication with respect to age and other patient/consultation attributes.
Due to practical constraints of coordinating assessors, this study did not employ a crossed-assessor design. Further estimation of reliability should be undertaken using a crossed-assessor design, to delineate the individual effects of case and assessor upon score.
Further evaluation
PCAT's design, with space for free-text comments and documentation of what has been seen and heard, makes it ideal for formative assessment where feedback can be used to guide future training and learning. We have not explored the educational impact of PCAT in this study, but this should be carried out when the assessment tool is incorporated into a wider assessment programme for paediatric trainees such as that organised by the RCPCH. PCAT's value within such a programme is likely to be one of exploration of specific communication difficulties, where these have been suspected by other methods such as multisource feedback.
Implications for assessment
What sort of cases should be recorded?
To assess the breadth of a clinician's performance, assessment should include recordings which capture children of a range of ages including those able to contribute to “medical” information-sharing parts of the encounter, and extended family members/carers.
Should clinicians themselves be allowed to select which videotaped consultations are assessed?
Our data suggest that performance does not vary hugely between individual consultations. Similarly, multisource feedback scores appear to be unaffected by case/respondent selection by the assessee.4,–,6 Thus clinicians should be allowed to choose their own consultations to submit for assessment.
Does it matter whether the first videotaped consultations are assessed relative to a later sample?
Corroborating with other researchers' findings that doctors' performance is not affected by the presence of video cameras for more than two or three consultations,23 this study found no significant difference between scores for the first and last three consultations recorded. Therefore assessees should be allowed to record consultations that represent cases from their usual practice, and be allowed to submit any of these, including the first 2–3 recorded, for evaluation.
Implications for training
It is not surprising, given other observational research, that this research shows clinicians' behaviour with children to be different from that with their parents.19 21 22 Children resent being left out of discussion about their illness but respond well to information which is specifically tailored to them.24 25 Therefore, although training in paediatric consultation skills should encompass rapport building with children and communication with their parents, more emphasis should be given to information sharing with children themselves. Training needs to be focused on interacting with pre-adolescent children, as well as teenagers.
Acknowledgments
Grateful thanks to families involved in the study and clinicians who were involved in collecting and assessing video material.
References
Footnotes
RH wrote the manuscript with assistance from the other authors.
-
Funding RH was supported by a grant donated to the Royal College of Paediatrics and Child Health by WellChild, and by the Department of Paediatrics, University of Cambridge. RH sought multicentre ethical approval, collected video material, trained assessors and undertook data analysis. HD, JS and JA supported development of the PCAT and study methodology. AM recruited clinicians/assessors.
-
Competing interests None.
-
Ethics approval Multicentre ethical approval was obtained for this study.
-
Patient consent Obtained.
-
Provenance and peer review Not commissioned; externally peer reviewed.