Article Text

Abstract
Objective: The purpose of this work was to investigate the incidence rate for admission and mortality of children receiving paediatric intensive care in relation to socioeconomic status and ethnicity in England and Wales.
Design: National cohort of sequential hospital admissions.
Setting: Twenty nine paediatric intensive care units in England and Wales.
Participants: All children aged under 16 years admitted to paediatric intensive care in the 4 years 2004–2007.
Main outcome measures: Incidence rates for admission and odds ratios (OR) for risk-adjusted mortality by an area based measure of deprivation (Townsend score) and ethnic group (south Asian vs non-south Asian determined using two-name analysis algorithms).
Results: The incidence for south Asian children was higher than that of non-south Asian children (138 vs 95/100 000, incidence rate ratio 1.36, 95% CI 1.32 to 1.40). The age-sex standardised incidence for children admitted to paediatric intensive care ranged from 69/100 000 in the least deprived fifth of the population to 124/100 000 in the most deprived fifth. The risk-adjusted OR for mortality for south Asian children was 1.36 (95% CI 1.18 to 1.57) overall, rising to 2.40 (95% CI 1.40 to 4.10) in the least deprived fifth of the population when a statistical interaction term for deprivation was included.
Conclusions: In England and Wales, the admission rate to paediatric intensive care is higher for children from more deprived areas and 36% higher for children from the south Asian population. Risk-adjusted mortality increases in south Asian children as deprivation decreases.
Statistics from Altmetric.com
Child health and survival are global priorities.1 In England and Wales, infant mortality and epidemiological evidence highlight health inequalities attributable to deprivation and ethnic group2 3 and these are the focus of targets for tackling health inequality.4 The overall infant mortality rate of 5.2 deaths per 1000 live births recorded in England and Wales increases with deprivation.5 The factors associated with excess infant mortality include low birth weight,5 ethnicity,6 poverty,7 the delivery of health care8 and consanguinity.9 In children born to mothers whose country of birth is Bangladesh, India or Pakistan, the infant mortality rate is 8.3 deaths per 1000 live births3 and this rises to 10.5 per 1000 in those born to mothers whose country of birth is Pakistan.5
What this study adds
Risk-adjusted mortality in children admitted to paediatric intensive care units (PICUs) is not higher in those from more deprived backgrounds.
Risk-adjusted mortality in south Asian children is higher than in the rest of the population admitted to PICUs and higher in those from the least deprived backgrounds.
The first population-based data on the epidemiology of children admitted to paediatric intensive care in England and Wales were reported by the Paediatric Intensive Care Audit Network (PICANet) in 2006.10 Equivalent data for comparison are sparse as other databases, such as those in the USA, do not estimate incidence rates for admission using national population data,11 although these data are now available from Australia.12 At a local level, Naclerio and colleagues in Washington, DC estimated the annual incidence of emergency admissions to a paediatric intensive care unit (PICU) at 166/100 000 for children under 14 years of age.13 They also identified higher levels of admissions in children from low income families. In children who receive paediatric intensive care, risk-adjusted outcomes using algorithms based on physiological status at admission, are routinely employed to help assess the relative performance of admitting PICUs.14 15 Until the establishment of PICANet, there were no data from England and Wales available on rates of admission or risk-adjusted mortality for critically ill children admitted to PICUs in relation to deprivation and ethnicity. Our objective was to generate incidence rates for admission and risk-adjusted mortality in relation to deprivation and ethnicity.
METHODS
A standardised dataset including demographic and clinical information and outcome (PICU mortality) is collected by PICU staff using bespoke software provided by PICANet on all admissions to PICUs in the UK. Training on data definitions and data collection has been provided by PICANet to ensure consistent data quality between units, together with local and central validation checks.10
Collection of personally identifiable data has been approved by the Patient Information Advisory Group (http://www.advisorybodies.doh.gov.uk/PIAG/Index.htm) and ethical approval granted by the Trent Medical Research Ethics Committee (ref 05/MRE04/17).
Study population
The population studied was all children (aged under 16 years) admitted to a PICU in England and Wales between 1st January 2004 and 31st December 2007, using data relating to the first admission of each child. Two South Asian names analysis programs were used to classify individual children as south Asian (Pakistani, Indian, Bangladeshi): Nam Pehchan16 and the South Asian Names and Group Recognition Algorithm (SANGRA).17 Results from these programs were then scrutinised for known misclassification errors which were corrected manually (for example, the surname Gill is classified as south Asian by SANGRA although the majority of children with this surname were not south Asian; similarly, Nam Pehchan matches on the forenames Ella, Amber, Maya and Paris, names that are common outside the south Asian community). The output from SANGRA provides an indicator as to whether a child is south Asian or not, but Nam Pehchan provides five matching levels: 0: no match on any name element; 1: stem match on one name element, no match on others; 2: full match on one name element, no match on others; 3: full match on one name, stem match on others; 4: full match on all names; 5: definitive match on at least one element. In view of the lack of sensitivity of Nam Pehchan (the sensitivity was 96% and the positive predictive value was 67.4% using the original population, but only 88.2% and 58.7%, respectively, in populations from Thames18) the classification of south Asian or not was conservatively based on a matching level of 3 or more and the output from SANGRA flagging the child as south Asian.
A deprivation score (the Townsend score) was derived for each child from the characteristics of the small census area of the child’s address at admission.19 All valid admission addresses were linked by their postcode to a UK census output area using the National Statistics Postcode Directory.20
Denominator populations
Population counts from the UK 2001 census for England and Wales21 were used as the denominator population when calculating age-sex standardised incidence by deprivation category based on the Townsend score. To take account of variations in birth rates identified in different ethnic groups, experimental statistics detailing childhood populations by standard UK census ethnic groups for England (for 2004–2006) were used to provide the denominator populations.22 The following ethnic categories from Census 2001 were included: White and Asian, Indian, Pakistani, Bangladeshi and Other Asian. Population data for 2007 were not available so 2006 figures were used. As the experimental statistics had not been calculated for Wales, the year by year percentage change from the Census 2001 populations in each age-sex strata were applied to the Welsh populations. Census data required to calculate the Townsend score were extracted at census output area level. Children with a residential address identified as outside the UK, or those without a valid address, were excluded from the analyses of incidence by deprivation but included in the univariate estimate of the odds of mortality for south Asian versus non-south Asian children admitted to PICUs.
Statistical analysis
Age-specific and age-standardised incidence rates for admission to a PICU between 2004 and 2007 were calculated with Poisson exact 95% confidence intervals (95% CI) for south Asian and non-south Asian children using the experimental statistics populations described above; and for all children aged under 16 years by deprivation category using the appropriate denominator populations from the 2001 UK census. Deprivation categories were based on the Townsend score of each census output area and were divided into fifths based on equal numbers of the childhood population in each fifth. Populations and admissions by age strata were then created by Townsend category. An incidence rate ratio (IRR) was calculated using Poisson regression to estimate the difference in rates between south Asian and non-south Asian children.
A random effects logistic regression model adjusting for within-centre clustering was used to calculate risk-adjusted odds ratios (ORs) for the effect of deprivation and ethnicity (south Asian or not) on PICU mortality.23 Risk adjustment for mortality used the log odds of mortality estimated using the Paediatric Index of Mortality (PIM)14 with recalibrated coefficients calculated by the United Kingdom Paediatric Intensive Care Outcome Study.15 A Townsend score was allocated to each child based on their admission address and this was equated to one of the fifths referred to above. This same categorical variable was modelled as an interaction term to investigate the relationship between ethnicity and deprivation on mortality. ORs for the effect on mortality of south Asian status in each deprivation category were calculated by multiplying the ORs of being south Asian in the first deprivation category by the interaction terms for each subsequent deprivation category and 95% CIs derived from the variance–covariance matrix using a linear combination of the estimates and standard errors. The effect of introducing the interaction term was assessed using the likelihood ratio test. The effect on mortality of age at admission in relation to ethnicity was investigated by introducing age in days and a variable indicating age less than 90 days or not as interaction terms in the statistical models. Gender was treated in a similar way.
Sensitivity analyses in relation to mortality were carried out comparing the results obtained using the conservative allocation of south Asian status with a dataset that included the following three more relaxed definitions: (1) a Nam Pehchan match level of two or more; (2) a Nam Pehchan match level of one or more; and then (3) where the Nam Pehchan match level was one or more and when it was equal to zero but SANGRA flagged the child as south Asian.
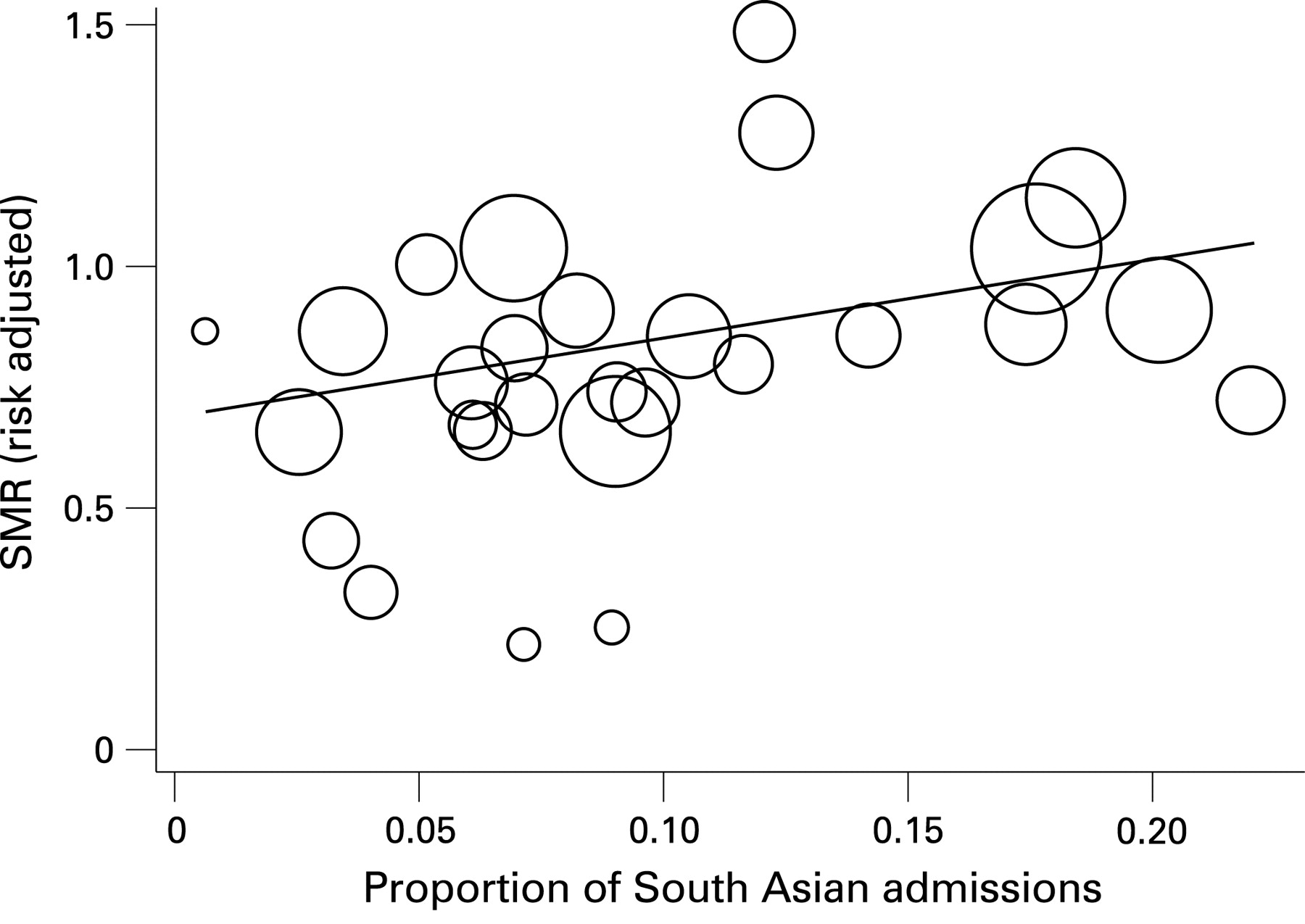
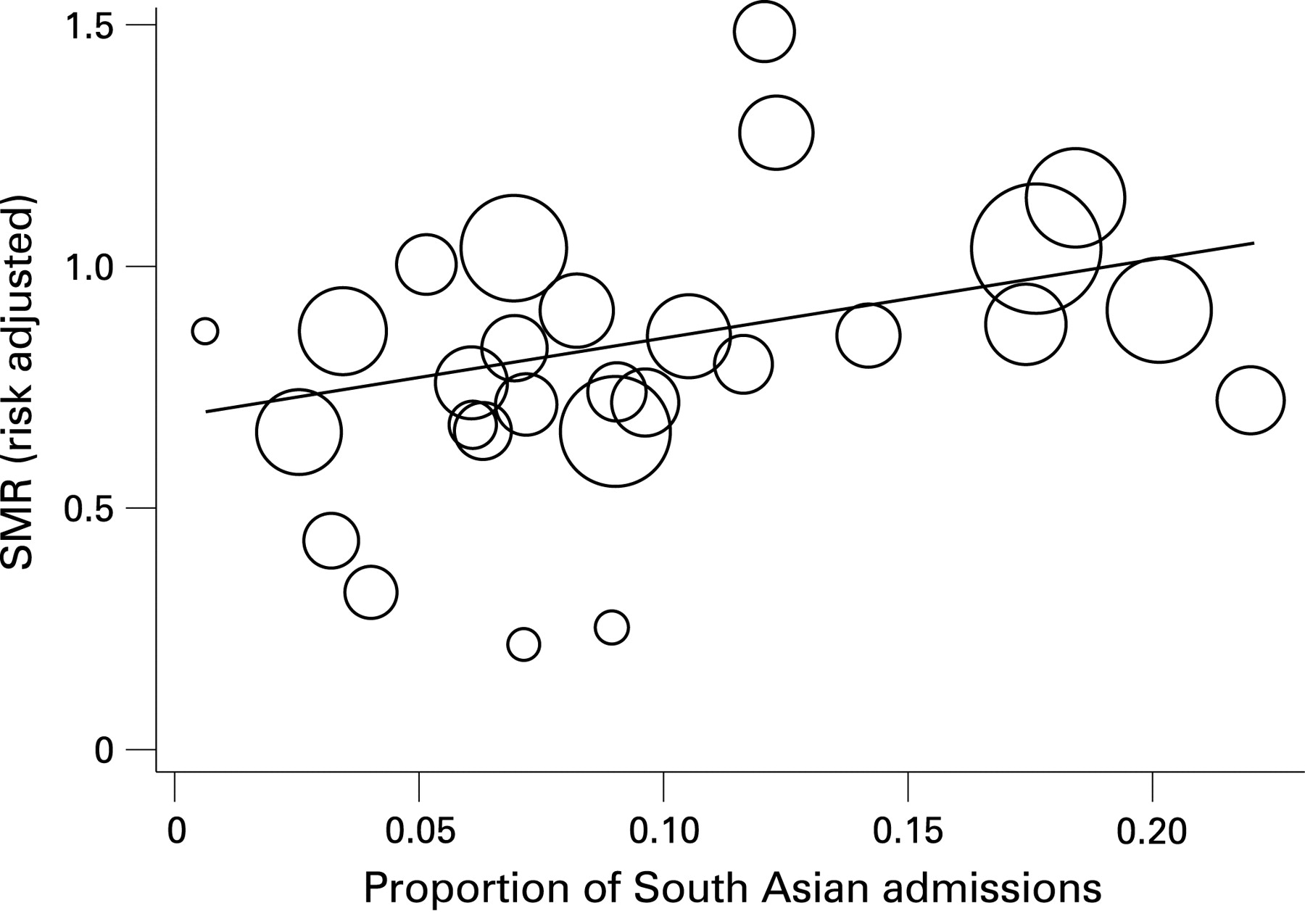
Standardised mortality ratios (SMRs) were calculated by PICU and plotted against the percentage of south Asian children admitted to each PICU. A linear regression of SMR on proportion of south Asian children admitted was performed weighted by the inverse of the variance of the number of admissions to each PICU.
Mortality was also analysed overall and by deprivation and ethnicity for children admitted for elective surgery versus those not. An interaction term for deprivation was introduced to investigate the relationship between ethnicity and deprivation on mortality in relation to elective surgical admission.
All analyses were carried out using Stata.24
RESULTS
Demographics
Nearly 11% of children were classified as south Asian compared with 7.7% of children in the general population calculated from the experimental statistics described above22 (table 1). The male to female ratio was 1.34:1 for south Asian children and 1.31:1 for non-south Asian children. Median gestational age was 38 weeks in south Asian and non-south Asian survivors and non-survivors (mean range across these groups 36.4–37.1 weeks).
Incidence
Between 2004 and 2007, a total of 40 303 children under 16 years of age were admitted to PICUs in England and Wales, giving an incidence rate of 98 per 100 000 child population per year. Of these, 4356 (10.8%) were classified as south Asian using the criteria described in the Methods section. Incidence for south Asian children was higher than for non-south Asian children (138 vs 95/100 000, incidence rate ratio 1.36, 95% CI 1.32 to 1.40) (table 2). The age-sex standardised incidence for all children admitted to paediatric intensive care in 2004–2007 ranged from 65/100 000 per year in the least deprived fifth of the population to 124/100 000 per year in the most deprived fifth.
Mortality
Crude mortality is 44% higher in south Asian children (7.11%) compared with overall mortality (4.91%) (table 3). There is a non-significant slight decrease in mortality associated with increasing deprivation (likelihood ratio test for trend χ2 = 0.31 (3 df), p = 0.96).
Table 4 presents ORs for the interaction between ethnicity (south Asian or not) and deprivation category. There is a significant elevated OR of 2.40 (95% CI 1.40 to 4.10, p = 0.001) for south Asian children in the least deprived Townsend category and significantly raised ORs in categories 2, 3 and 5, reducing with increasing deprivation. The introduction of an interaction between deprivation and ethnicity did not significantly improve the model fit (likelihood ratio test χ2 = 8.02 (4 df), p = 0.091). The overall OR for admissions for planned surgery was 0.63 (95% CI 0.54 to 0.74). There were no significantly increased or decreased ORs for planned surgery by ethnicity or deprivation when modelled in a univariable analysis (data not shown). In the interaction model, the OR for planned surgery was elevated for south Asian children in the least deprived Townsend category (OR 2.24, 95% CI 0.51 to 9.77, p = 0.283) and significantly in non-surgical admissions (OR 2.41, 95% CI 1.35 to 4.31, p = 0.003). There was no interaction between ethnicity and age in days or the indicator variable for age less than 90 days or sex and the ORs for mortality.
The sensitivity analyses were performed at three levels: (1) including Nam Pehchan match level two and above (an additional 10 children); (2) match level one and above (an additional 366 children including match level two) and (3) match level one and above where SANGRA flagged the child as south Asian but Nam Pehchan gave no match (an additional 824 children inclusive). The additional 468 children in this category included 168 children with the forename “Baby” and the majority of the other names were unambiguously not south Asian. The relaxed matching levels (1) and (2) above had very little effect on the ORs for mortality; the analysis of level (3) produced ORs for mortality for all admission types of 1.94 (95% CI 1.15 to 3.30), 1.84 (1.17 to 2.90), 1.53 (1.07 to 2.21), 1.27 (1.15 to 3.30) and 1.24 (1.01 to 1.52) for the interaction between south Asian status and least-deprived and most deprived fifths of the cohort, respectively. These are slightly lower than in the most “conservative” allocation of south Asian status for the two less deprived fifths of the cohort but the other three fifths are very similar.
For illustration, fig 1 plots risk-adjusted SMRs against the proportion of south Asian children admitted to each PICU. There is a significant increase in SMR as the proportion of south Asian children admitted increases (weighted linear regression coefficient 1.64, 95% CI 0.26 to 3.01, p = 0.022).
{kind=link}
DISCUSSION
Approximately 0.1% of the childhood population in England and Wales were admitted to paediatric intensive care between 2004 and 2007. Nearly half of these children were under 1 year of age.10 Our findings confirm that admission rates to paediatric intensive care for individuals increase with increasing material deprivation (using an area-based measure) from 65/100 000 to 124/100 000 children in the most deprived fifth of the population. Increased admission rates for more deprived children have been observed in the United States13 but have not been reported elsewhere. These data will be important for those involved in the planning of health care provision.
Deprivation has been associated with higher infant mortality in national data4 and in an urban population in the UK,7 and crude mortality in the poorest group in this series is higher than the national average for PICUs at 5.33% versus 4.91%. This however, reflects the severity of illness at presentation: risk-adjusted mortality is not elevated in more deprived categories (indeed, it shows a non-significant reduction in OR in the population as a whole). There is a raised risk-adjusted OR for mortality in south Asian children overall, which appears to be driven by an interaction with deprivation, with higher levels of deprivation associated with reduced risk of mortality. This appears to be the reverse of trends seen in national mortality data. There is also no reduced risk-adjusted mortality in admissions after elective surgery in the most affluent compared with the most deprived fifth of the population as seen in adult intensive care,25 although there is excess mortality in the least deprived and most deprived south Asian children in elective surgical admissions. Non-surgical admissions reflect the pattern of a reducing risk of mortality in south Asian children with increasing deprivation shown overall. The indication that risk-adjusted standardised mortality rates increase with the proportion of south Asian children admitted to each PICU (fig 1) is of interest, but great care should be taken when interpreting performance of PICUs measured by mortality in the context of ethnicity.
Raised infant mortality in the children of mothers born in Bangladesh, India or Pakistan in the general population3 is reflected in our findings for south Asian children admitted to paediatric intensive care. As we have calculated the log odds of mortality based on a validated mortality risk-adjustment tool, the Paediatric Index of Mortality,14 this increased risk would not appear to be attributable to south Asian children presenting with more severe physiological symptoms.
Consanguinity has been identified as a major risk factor for perinatal and infant mortality, especially in Pakistan where consanguineous marriages, especially of first degree cousins, are associated with increased mortality in children under 5 years of age.9 We have not, however, observed an interaction with age that reflects the effect of increased mortality in the under fives in our data either when considered as a continuous variable or in those under 90 days. In addition, the distribution of gestational age is not significantly different between south Asian and non-south Asian children admitted to PICUs. Although data on co-morbidity are collected by PICANet, not all PICUs have sufficient resources to collect these data. We are not, therefore, able to identify those children who have congenital conditions that may be attributable to consanguineous marriages but do not form part of our risk-adjustment model.
Despite evidence that increased mortality and morbidity in the UK Pakistani population may be attributable to autosomal recessive diseases,26 our data do not allow us to identify direct causal factors relating to the excess mortality in south Asian children. The risk-adjustment tool may not be sensitive to, or even calibrated for, ethnicity-specific pathophysiology such as variation in allostatic load,27 or response to paediatric intensive care treatment.28 We have used PIM14 rather than the later PIM 229 as PIM 2 was not published when we commenced data collection. PIM and PIM 2 both perform well in comparison with other mortality prediction tools such as the Paediatric Risk of Mortality Score III and have a much lower burden of data collection.15
We do not know whether cultural or social factors would influence outcome of paediatric intensive care treatments, and we caution against genetic and biological explanations for mortality inferred from race alone.30 In the USA, heritable diseases have frequently been noted as the underlying cause of mortality on PICUs but not identified as such in routine mortality statistics.31 These co-morbid conditions not accounted for by the risk-adjustment model may nevertheless contribute to increased probability of mortality. No comparisons between deprivation or ethnic group and later mortality or morbidity were possible as long-term outcome data were not available.
This study is based on a unique dataset and has a number of strengths: the analysis relates to information held on individual children in a national, population-based dataset that is subject to extensive validation and provides complete and accurate data on children admitted to PICUs in England and Wales.10 We used two Asian name identification programs to validate our classification of south Asian status using a conservative cross-match as we were aware that Nam Pehchan16 could possibly produce false positives.18 Repeating the analyses using different classification cross-matches based on Nam Pehchan and SANGRA made no significant difference to the overall results except for a moderate reduction in OR when the least conservative allocation of south Asian status was used. We identified a number of obvious misclassifications in this group and it is unsurprising, therefore, that the ORs were slightly attenuated. There is no available information on the reliability of the name analysis programmes in relation to mixed Asian ancestry and we acknowledge that this may be a source of classification error. Given the strength of the associations we have observed, however, it is unlikely that any small level of misclassification in our more conservative allocation of south Asian status would bias the overall outcome observed in this data.
While higher admission rates of more deprived children and children from a south Asian background to paediatric intensive care reflect previous research and UK statistics on health inequalities, we have observed excess risk-adjusted mortality in south Asian children, especially those from less deprived backgrounds. Excess mortality in infants of south Asian origin has also been observed in the neonatal intensive care population in Canada, even after adjusting for those small for gestational age and short gestation.32 Although there is some evidence that class inequalities in self-rated health seen in the white population are not apparent in Pakistani and Bangladeshi adults,33 it is not clear why there is such a strong interaction between less deprived children of south Asian origin and excess mortality. The reasons for this excess warrant further investigation.
Acknowledgments
We would like to thank all the staff in participating hospitals who have collected data for PICANet. We are grateful to the Paediatric Intensive Care Society for continued support and to the members of the PICANet Steering Group and Clinical Advisory Group listed below. Thanks also to Gill Ryder and Angie Willshaw for assisting with data collection and administration and Tom Fleming for managing the PICANet database. We are especially grateful to Dr Punam Mangtani for processing our data using the SANGRA name analysis program. Sarah Hepworth and Richard Feltbower provided additional statistical advice.
REFERENCES
Footnotes
Funding: PICANet is funded by the Healthcare Quality Improvement Partnership (HQIP), Health Commission Wales Specialised Services, NHS Lothian/National Service Division NHS Scotland, the Royal Belfast Hospital for Sick Children and the Pan Thames PICU Commissioning Consortium. The views expressed are those of the authors.
Competing interests: None.
List of participating NHS Trusts and hospitals: Addenbrooke’s NHS Trust: Addenbrooke’s Hospital; Birmingham Children’s Hospital NHS Trust: Diana, Princess of Wales Children’s Hospital; Brighton and Sussex University Hospitals NHS Trust: Royal Alexandra Hospital for Sick Children; Cardiff and Vale NHS Trust: University Hospital of Wales; Central Manchester and Manchester Children’s University Hospitals NHS Trust: Royal Manchester Children’s Hospital; Great Ormond Street Hospital for Children NHS Trust: Great Ormond Street Hospital for Sick Children; Guy’s and St. Thomas’ Hospital NHS Trust: Guy’s Hospital; Hull and East Yorkshire Hospitals NHS Trust: Hull Royal Infirmary; King’s College Hospital NHS Trust: King’s College Hospital; Leeds Teaching Hospitals NHS Trust: Leeds General Infirmary, St. James’ University Hospital; Newcastle upon Tyne Hospitals NHS Trust: Newcastle General Hospital, Freeman Hospital, Royal Victoria Infirmary; Oxford Radcliffe Hospitals NHS Trust: John Radcliffe Hospital; Queen’s Medical Centre Nottingham University NHS Trust: Queen’s Medical Centre; Royal Brompton & Harefield NHS Trust: Royal Brompton Hospital; Royal Liverpool Children’s NHS Trust: Alder Hey Hospital; Sheffield Children’s NHS Trust: Sheffield Children’s Hospital; Southampton University Hospitals NHS: Trust Southampton General Hospital; South Tees Hospitals NHS Trust: James Cook University Hospital; St. George’s Healthcare NHS Trust: St. George’s Hospital; St. Mary’s NHS Trust: St. Mary’s Hospital; The Lewisham Hospitals NHS Trust: University Hospital, Lewisham.
PICANet Steering Group members: Mrs Pamela Barnes, Professor Nick Black (Chair) (2002–2007), Mr William Booth, Ms Bev Botting Child (2002–September 2003), Dr Jean Chapple (2002–2006), Dr Bill Chaudhry (2002–September 2003), Dr Mark Darowski, Mr Noel Durkin, Dr Steve Kerr, Mr Ian Langfield (2002–September 2003), Dr Michael Marsh, Dr Jillian McFadzean, Dr Roddy McFaul (2002–September 2003), Professor Jon Nicholl, Dr Gale Pearson, Ms Tanya Ralph, Ms Laura Reekie, Dr Kathy Rowan, Mr Stuart Rowe, Ms Dominique Sammut, Dr Jenifer Smith, Dr Charles Stack, Professor Stuart Tanner, Dr Robert Tasker.
PICANet Clinical Advisory Group members: Dr Paul Baines (2002–present), Ms Corenna Bowers Sister (2002–September 2004), Dr Andrew Durward (2002–present), Ms Georgina Gymer (2005–October 2006), Dr James Fraser (2002–October 2005), Dr Hilary Klonin (2002–present), Ms Christine Mackerness (2002–present), Dr Jillian McFadzean (2005–present), Ms Victoria McLaughlin, (2002–present), Dr Roddy O’Donnell (2002–present), Ms Geralyn Oldham (2002–present), Dr Gale Pearson (Chair) (2002–present), Dr Damian Pryor (2002–September 2004), Dr Allan Wardhaugh (Sept 2004–present), Ms Debbie White (2002–present).
Contributors and sources: ESD, PAM and RCP are principle investigators for PICANet. GJP is a former principle investigator. RCT is a consultant paediatric intensivist and chair of the Paediatric Intensive Care Society Study Group. KT is a co-worker in PICANet and SJ and TC former co-workers. RCP, ESD, PAM and GJP initiated the project. RCP conducted the statistical analysis and wrote the first draft. GJP provided additional statistical advice. Thereafter RCP, PAM, RCT GJP, ESD, KT, SJ and TC critically revised the manuscript. PAM is the guarantor.