Article Text

Abstract
Objectives: To determine whether a school obesity prevention project developed in the United States can be adapted for use in England.
Methods: A pilot cluster randomised controlled trial and interviews with teachers were carried out in 19 primary schools in South West England. Participants included 679 children in year 5 (age 9–10). Baseline and follow-up assessments were completed for 323 children (screen viewing) and 472 children (body mass index). Sixteen lessons on healthy eating, physical activity and reducing TV viewing were taught over 5 months by teachers. Main outcome measures were hours of screen activities, body mass index, mode of transport to school and teachers’ views of the intervention.
Results: Children from intervention schools spent less time on screen-viewing activities after the intervention but these differences were imprecisely estimated: mean difference in minutes spent on screen viewing at the end of the intervention (intervention schools minus control schools) adjusted for baseline levels and clustering within schools was −11.6 (95% CI −42.7 to 19.4) for a week day and was −15.4 (95% CI −57.5 to 26.8) for a Saturday. There was no difference in mean body mass index or the odds of obesity.
Conclusions: It is feasible to transfer this US school-based intervention to UK schools, and it may be effective in reducing the time children spend on screen-based activities. The study has provided information for a full-scale trial, which would require 50 schools (∼1250 pupils) to detect effects on screen viewing and body mass index over 2 years of follow-up.
Statistics from Altmetric.com
Persistent obesity is established before the age of 11; therefore, obesity prevention needs to be targeted at children aged under 11.1 Many behaviours are known to be associated with childhood obesity: consumption of fizzy drinks,2 hours spent viewing television,3 4 regular consumption of fast food5 and sedentary behaviour.5 However, there is a paucity of evidence about effective interventions to prevent obesity.6–9 Three reviews10–12 of interventions to prevent obesity during childhood or adolescence noted that few studies achieved a sustained change in body mass index (BMI).
An earlier review13 recommended multi-faceted, school-based interventions, following Harvard School of Public Health’s success in changing obesity rates and risk factors for obesity in the United States through two similar health-promotion programmes for different ages (Planet Health3 and Eat Well Keep Moving14) based on social cognitive theory and behavioural choice theories of individual change. A cluster randomised controlled trial of 10 schools (five intervention; five control) examining the effect of the “Planet Health” programme of lessons found that girls in the intervention schools were less likely than those in the control schools to be obese at the end of follow-up, whereas no effect on obesity was found for boys.3
This study aimed to evaluate the feasibility of adapting the lessons from this US intervention for use in the UK and to examine the effect of the lessons on children’s time spent on screen-viewing activities, BMI and mode of transport to and from school in a short-term (5 months) pilot cluster randomised controlled trial of UK children aged 9–10 years. This study was a pilot designed primarily to inform a larger trial.
METHODS
Study design
The “Active for life year 5” project was conducted as a pilot cluster randomised controlled trial in 2006, in year 5 classes in 19 primary schools in England.
Twenty-seven schools in South Gloucestershire (n = 27) were invited to take part in the study. The schools were informed they would be randomly allocated to “intervention” or “control” groups, with the intervention schools being provided with the teacher training and teaching materials and the control schools being provided with these after the completion of the study. Nineteen schools agreed to be in the study. The timescales for recruiting the schools were short, which deterred some of the schools from taking part. Random allocation to intervention or control school was concealed and done by one of the authors (DAL).
Intervention
The project was an adapted and abbreviated form of the “Eat Well Keep Moving” programme developed in the United States.14 Sixteen lessons on healthy eating, increasing physical activity and reducing TV viewing were adapted by two primary school teachers for the English school setting. The main changes were to shorten the lesson plans, change US phrasing or references and change the pyramid structure of food groups to the balance of good health. The pilot did not include two staff meetings. Two teachers provided a training session for the 10 teachers who were teaching the lessons, and materials were provided to the schools. Materials included lesson plans for nine physical activity lessons, six nutrition lessons and one lesson about screen viewing (see table 1). In the physical activity lessons, the children played games based on the food groups using photographs of food that reinforced the theory taught in the nutrition lessons.
Outcome measures
All measurements were taken before the lessons were taught (February 2006) and five months later (July 2006).
The primary outcome was reduction in time spent doing screen-based activities (watching television, videos, DVDs or computer games). The children completed a questionnaire about the length of time spent doing screen-based activities on the previous weekday and Saturday. The questionnaire was an abbreviated and updated version of a questionnaire designed by Robinson.15 Before doing the main analyses we decided to exclude from the analyses any child with a sum of 720 minutes or greater of screen-based activities for the weekdays and any child with a sum of 1080 minutes of such activities for Saturday. This resulted in the exclusion of 52 children from both the intervention schools and control schools. The limits of 12 hours for weekdays and 18 hours for weekends were chosen as the maximum plausible hours on these activities assuming 6 hours spent at school during the week and at least 6 hours of sleep.
A questionnaire called “A Day in the Life”16 was completed by the children and provided information about their activities during the previous day. This questionnaire was used to determine the mode of transport to and from school defined as walking/cycling or being driven or going by bus to school.
School health assistants, who were blinded to the allocation of schools, took height and weight measurements. Height (without shoes) was measured to the nearest 0.1 cm with minimeter height scales. Weight (without heavy clothing) was measured to the nearest 0.1 kg on portable bathroom scales. Obesity was defined using the BMI (weight (kg)/(height (m)2)) above the 95th centile of the reference curve for the age and gender of each child. This cut-off is derived from the UK National BMI classification, which uses the 1990 reference population.17
Six of the 10 teachers took part in an interview with one of the authors (RK) in which they were asked about the training day, measurements and lessons.
The US study was evaluated over a two-year period. However, it was not possible for us to undertake a long-term trial before completing initial feasibility work. The programme was implemented over two terms with teacher training taking place in January 2006, the intervention taking place between February–June 2006 and the final outcome assessment in July 2006. We evaluated the effect of the programme over a 5-month period from February to July.
Statistical methods
Since this was a pilot study, we aimed to recruit as many schools and their pupils as possible and use the results, including the intraclass correlation coefficients (required for an appropriate sample size calculation of a clustered randomised controlled trial) to calculate the necessary sample size for a full-scale study.
All analyses were undertaken using an intention to treat protocol, regardless of the number of lessons taught in intervention schools. However, we only included in the analyses those children with complete data at baseline and outcome. Multivariable regression (linear or logistic) was used to determine the mean difference or odds ratio comparing intervention to control schools at follow-up. In these analyses, adjustment was made for age, gender and the baseline level of the outcome of interest to maximise precision. We used robust standard errors to take account of clustering (non-independence between pupils from the same school) in the computation of 95% confidence intervals and p values. We also present results without this clustering being taken into account as a demonstration of how this affects the precision of the estimate and the p values. All analyses were undertaken, in Stata version 9.2, by DAL who was blinded to which were the intervention and which the control group of schools.
Ethics
Ethical approval was sought from the National Health Service but the chairman of the local research committee said that since this was research that did not involve patients or NHS staff ethical approval was not required. Parents were asked to give written consent for each of the outcome measures.
RESULTS
Comparison of outcomes
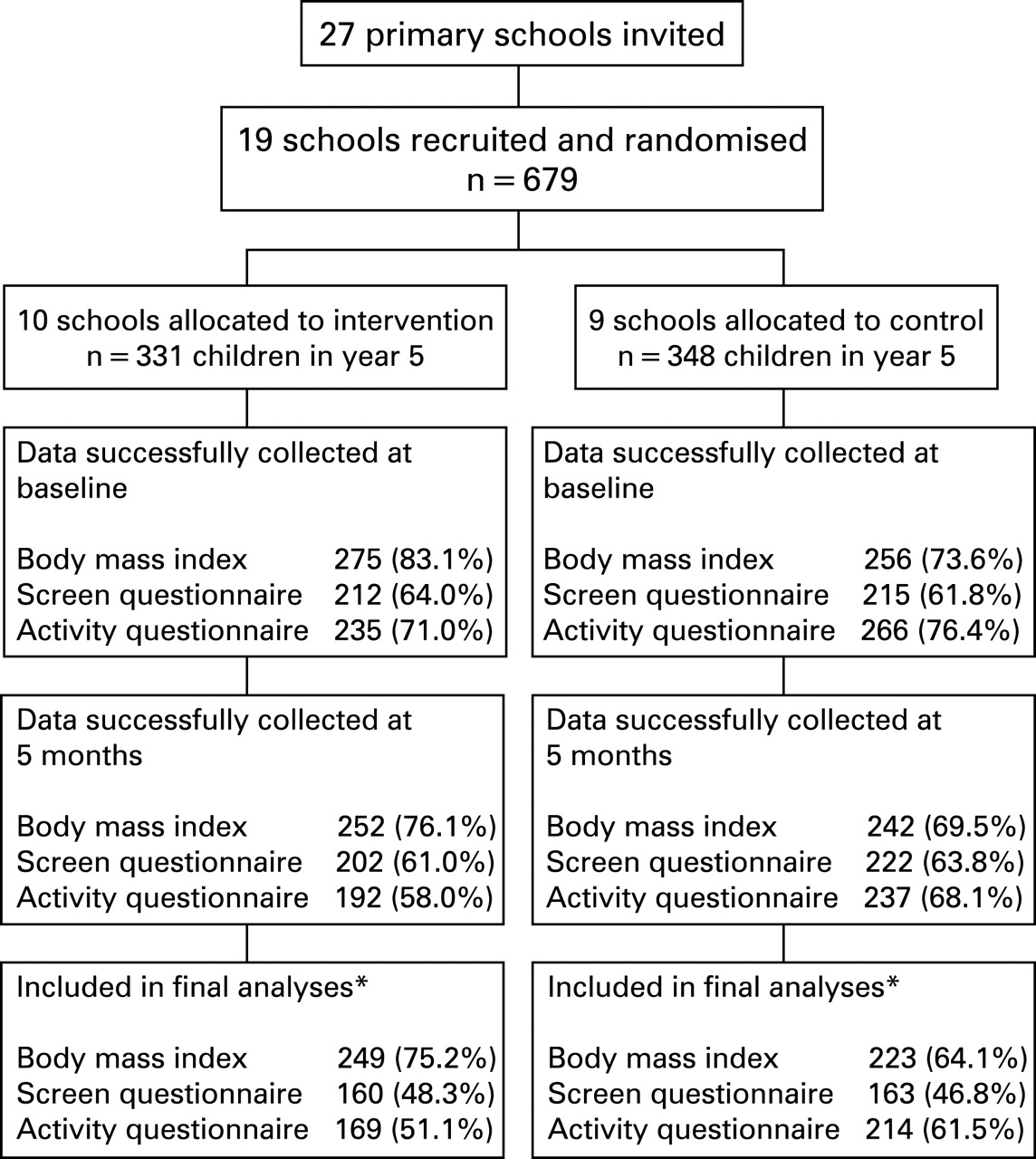
Figure 1 shows the flow of pupils through the study. The greater extent of missing data for screen viewing and mode of transport to school occurred because of a number of questionnaires being returned without the child’s name and because of excluding some participants with implausible levels of screen viewing (see above). Baseline characteristics for those pupils included in the analysis were similar for those from the intervention and control schools, with the exception of the proportion walking or cycling to school (table 2). Despite concealed random allocation, pupils from those schools allocated to the control group were more likely at baseline to walk/cycle to school than those allocated to the intervention schools.

{kind=link}
Table 3 compares the outcomes at follow-up between children in the intervention schools and those in the control schools. Children from intervention schools spent less time on screen viewing activities at the end of the intervention compared with children from control schools, but these differences did not reach statistical significance. Mean difference in minutes spent on screen viewing at the end of the intervention (intervention schools minus control schools) adjusted for baseline levels and clustering within schools: −11.6 minutes (95% CI: −42.7 to 19.4) for weekday and −15.4 minutes (−57.5 to 26.8) for Saturday. There was no difference in mean BMI or the odds of obesity between pupils allocated to intervention schools and those allocated to control schools. At the end of follow-up, pupils who were allocated to control schools tended to have an increased odds of walking or cycling to school despite adjustment for the baseline difference in this outcome. As anticipated, the 95% confidence intervals were narrower and the p values were smaller for all outcomes when clustering within schools was (inappropriately) not taken into account in our analyses.
Examination of the point estimates suggested no difference by gender for any of the outcomes except the odds of being obese at follow-up. Among males the odds ratio comparing those in intervention schools to control schools (with adjustment for baseline obesity and clustering) was 0.28 (95% CI: 0.06 to 1.33) and in females it was 1.52 (95% CI: 0.37 to 6.25) in females, p value for gender* intervention interaction = 0.09.
When we included all children, irrespective of their reported viewing times, and in a separate analyses that excluded a greater number of children by using the lower threshold for believable values (8 hours for week days and 14 hours for weekend days), the results did not differ substantively from those presented here.
The intraclass correlation coefficient for screen viewing from this pilot study was 0.01 (95% CI: 0.00 to 0.03) and that for BMI was 0.02 (95% CI: 0.01 to 0.03). In our sample-size calculation for a full-scale randomised controlled trial, we have used the upper limit of the 95% confidence interval for these intraclass correlation coefficients (ie, 0.03 for both screen viewing and BMI).
Interviews with teachers
The majority of teachers were positive about the training they received and content of the lessons. Several teachers regarded the lessons as suitable to use in the Qualifications and Curriculum Authority’s “keeping healthy” topic. The majority of teachers found it difficult to fit the lessons into the timetable and only two teachers taught all the lessons. All the teachers who were interviewed taught at least half the lessons. They gave positive comments about the response of the children to the lessons. The teachers thought the programme had increased children’s knowledge about healthy eating and physical activity, but varied in their views about the impact it had made on behaviour.
DISCUSSION
Our pilot study suggests that a school-based intervention that has been shown in the United States to be effective in reducing screen-based activities can be successfully adapted and transferred for use by schools in the United Kingdom. Teachers responded positively to the training day for delivering these lessons and to the content of the lessons.
Study strengths and limitations
The investigator who did the random allocation had no prior knowledge of characteristics of any of the schools; therefore allocation was concealed. An intention to treat analysis was undertaken, and the analyst for the quantitative comparisons was blind to which group was the intervention or control. However, there were several limitations to the study. The questionnaires were self-administered, which reduced the number of children included in the analysis because of incomplete completion of personal identifiers. It is possible that the questionnaires were not sufficiently valid and sensitive for changes to be detected over the short period. However, for our main outcome measure (time spent screen viewing) we used a questionnaire that had been tested for use in US school children of the same age.15 The questionnaire was found to have excellent test–retest reliability (r = 0.94),18 but poor levels of agreement with parental reports of screen viewing (r = 0.17–0.49).15 We were unable to collect information on parental report of children's screen viewing. However one cannot assume that the parental report would be more accurate than the child’s since children of this age are known to engage in these activities in their bedrooms. In the US study the magnitude of the effect of the intervention was similar for either child’s own or parental report of screen viewing.15 In our study, we found similar results using no exclusions on the basis of implausible values in the child’s report of screen viewing activities and when we used two different thresholds for excluding those with possible implausible values. The similarity of these findings suggests that if there is measurement error in the child’s report it is similarly distributed across the two randomisation arms.
The cluster randomisation design incurs a risk that there can be different responses within a school; however, we aimed to minimise differences between schools by selecting schools in similar geographical areas with similar demographic profiles.
This was a pilot and feasibility study and therefore we did not undertake a formal cost-effectiveness analysis, but would do so in a full-scale trial. The cost of training teachers to use the adapted material and providing sets of journals to schools is relatively cheap: approximately £110 per teacher and £2 per pupil.
Main implications of the study findings
Our findings suggest that similar to the US studies,3 14 the intervention was associated with a reduction in the amount of time children spent on screen-based activities. However, our study had insufficient power to provide precise estimates of this effect and had a shorter follow-up period than the US studies. Unlike the US studies we did not note a stronger effect in females compared with males.
On the basis of the results from this study and the previous US studies, we estimate that a full-scale trial would require 50 schools each with an average of 25 pupils in year 5 to be randomly allocated to detect a 15-minute difference in screen-based activities during the weekdays and a 20-minute reduction on weekend days (114 minutes less per week) sustained over 2 years of follow-up. This calculation assumes an alpha level of 0.05 and power of 90% and provides the same level of power to detect a mean difference of 0.5 SD of mean BMI and adequate power for important secondary outcomes (levels of obesity, waist circumference, energy expenditure measured by accelerometer).
In a full-scale trial we would recommend using trained researchers to administer the questionnaires. We tried to use pedometers in this study but found that they were unreliable. Because of this, and findings from studies in adults,19 we would recommend that movement sensors (accelerometers)20 21 are used to measure activity.
To conclude, our study suggests that a US school-based programme can be adapted for use in UK children and may reduce time spent on screen viewing in these children. This study has provided us with the necessary information for undertaking a full-scale trial of this promising intervention.
What is already known on this topic
There is not a strong evidence base for the effectiveness of interventions to prevent obesity through school-based programmes.
The Planet Health programme in the United States reduced levels of obesity but it had not been adapted for use in England.
What this study adds
A pilot study of a multi-faceted school-based obesity prevention programme developed in the United States has been successfully adapted and transferred for year 5 classes in the United Kingdom.
A full-scale trial would require 50 schools, each with approximately 25 pupils, to be adequately powered to precisely estimate potentially important effects and should include parental involvement, a formal cost-effectiveness analysis and an objective measure of physical activity using movement sensors (accelerometers).
Acknowledgments
We thank Harvard School of Public Health for their permission and support in adapting the “Eat Well Keep Moving” project for the UK, particularly Lilian Cheung, Steve Gortmaker and Hank Dart. We thank Sara Cooper at Human Kinetics Publishers for giving us permission to adapt the lessons. We thank the staff and pupils of the following schools for their participation and support: Our Lady of Lourdes Catholic Primary School, Barley Close Community Primary School, Barrs Court Primary School, Filton Hill Primary School, Stoke Lodge Primary School, Patchway CE Primary School, Shield Road Primary School, Mangotsfield Primary School, Emerson’s Green Primary School, The Tynings Primary School, Beacon Rise Primary School, Charborough Road Primary School, Cadbury Heath Primary School, St Barnabus Primary School, St Michael’s Primary Stoke Gifford, Holy Family Primary School, Deer’s Wood School, Staple Hill Primary School, Courtney Primary School. We thank the steering group for their advice: Maggie Sims, Lindsey Thomas, Nicola Ravenscroft, Sue Odgers, Jeanette Quinn, Kim Hazeldine. We thank Jean Powell and Ruth Treneer for their work in adapting the lessons. We thank the school health assistants at North Bristol Teaching NHS Trust for doing the height and weight measurements. We thank Tom Robinson for permission to adapt the TV questionnaire and Laurel Edmonds and Sue Ziebland for permission to use the “A day in the life” questionnaire. We thank Tom Steuart-Feilding, University of Bristol, for entering the data.
The South West Public Health Group runs the South West Public Health Training Scheme. RK is employed by the training scheme, DAL is an academic trainer for the training scheme and CP is a service trainer for the training scheme.
REFERENCES
Footnotes
Funding: Funding was received from the Department of Health via the South West Public Health Group, South Gloucestershire Council, and DAL is funded by a Department of Health Career Scientist Award, which also funded data entry.
Competing interests: None.