Article Text

Abstract
Children in primary school can be very disabled by chronic fatigue syndrome or ME (CFS/ME). The clinical presentation in this age group (under 12 years old) is almost identical to that in older children.
Aim: To describe children who presented to the Bath paediatric CFS/ME service under the age of 12 years.
Method: Inventories measuring fatigue, pain, functional disability, anxiety, family history and symptoms were collected prospectively for all children presenting to the Bath CFS/ME service between September 2004 and April 2007. Data from children who presented to the service under the age of 12 are described and compared to those who presented at age 12 or older.
Results: 178 children (under the age of 18) were diagnosed as having CFS/ME using the RCPCH criteria out of 216 children assessed. The mean age at assessment for children with CFS/ME was 14.5 years old (SD 2.9). Thirty-two (16%) children were under 12 years at the time of assessment, four children were under 5 years and the youngest child was 2 years old. Children under 12 were very disabled with mean school attendance of just over 40% (average 2 days a week), Chalder fatigue score of 8.29 (CI 7.14 to 9.43 maximum possible score = 11) and pain visual analogue score of 39.7 (possible range 0–100). Comparison with children aged 12 or older showed that both groups were remarkably similar at assessment. Twenty-four out of the 26 children with complete symptom lists would have been diagnosed as having CFS/ME using the stricter adult Centers of Disease Control and prevention (CDC) criteria.
Conclusion: Disability in the under-12 age group was high, with low levels of school attendance, high levels of fatigue, anxiety, functional disability and pain. The clinical pattern seen is almost identical to that seen in older children, and the majority of children would also be diagnosed as having CFS/ME using the stricter adult definition.
Statistics from Altmetric.com
Chronic fatigue syndrome/ME is defined in the Royal College of Paediatrics and Child Health Evidence Based Guideline for the Management of CFS/ME as “generalised fatigue persisting after routine tests and investigations have failed to identify an obvious underlying cause”.1
Although some papers make reference to CFS/ME starting at a young age (eg, some studies suggest a mean age of onset of 8.7–11.6 years2–5), other reports have excluded children under the age of 12.6 To date there are no studies describing how these young children present to clinicians.
In this paper we describe a cohort of 32 children who presented with CFS/ME while at primary school. We then compare them to children presenting in the same time frame but aged 12 years or over in terms of symptoms at presentation, fatigue, anxiety, disability, pain and school attendance.
METHODS
The Bath paediatric CFS/ME service provides assessment and treatment for over 150 children and young people each year. The service covers Bath, Bristol, West Wiltshire, Somerset and Gloucestershire. This region has over 400 000 children aged 5 to 19 years according to the 2001 census.
Before assessment, the following inventories were collected: 11-item Chalder fatigue scale, SF36 (physical function subscale) for functional disability, Spence children’s anxiety scale (SCAS) on children 14 years old and younger, pain visual analogue scale and school attendance rates. The 11-item Chalder fatigue scale was scored using the bimodal method for scoring each item (0 for “less than usual” and “no more than usual” and 1 for “more than usual” and “much more than usual”). Children score 1 for “yes limited a lot” and 3 for “no not limited at all”. Children with the most disability therefore score 10, whereas those with the least disability score 30. The SCAS measures the frequency with which a child experiences symptoms relating to anxiety. There are four possible answers for each question: never (score 0), sometimes (score 1), often (score 2) and always (score 3). School attendance is measured with a single-item question on how much they attend school as a percentage of possible school attendance.
At assessment children are asked about the presence or absence of symptoms using a symptom list derived from the CDC criteria7 and the RCPCH guidelines.1 Time to assessment is calculated as the time from the first onset of symptoms to the assessment date. Screening investigations are carried out on all children as recommended in the RCPCH guidelines.1
Data were analysed for children (under the age of 18) who were assessed by the CFS/ME service between April 2005 and April 2007 and had a diagnosis of CFS/ME made at assessment. The notes were reviewed to check whether an alternative diagnosis had been made at follow-up.
Inventories were excluded entirely for analysis if there was more than one missing item. Items were counted as missing if there were two answers given. For the symptom checklist, data were included even if the symptom list was incomplete. For the children under 12, if the parent and/or child were uncertain whether a symptom was a problem, the data were left as missing and the remaining symptoms were included in the analysis.
The data were analysed using STATA 9.2 for Windows. Children under 12 were compared to children aged 12 and over using the Fisher’s exact test (percentage with each symptom, male to female ratio) or the unpaired t test (fatigue score, pain, SF36, number of symptoms present and time at school).
RESULTS
Two hundred and sixteen children were under 18 years old at the time of assessment, and 40 of these were 11 years old or younger. Overall, 82% of children assessed had CFS/ME confirmed at assessment.
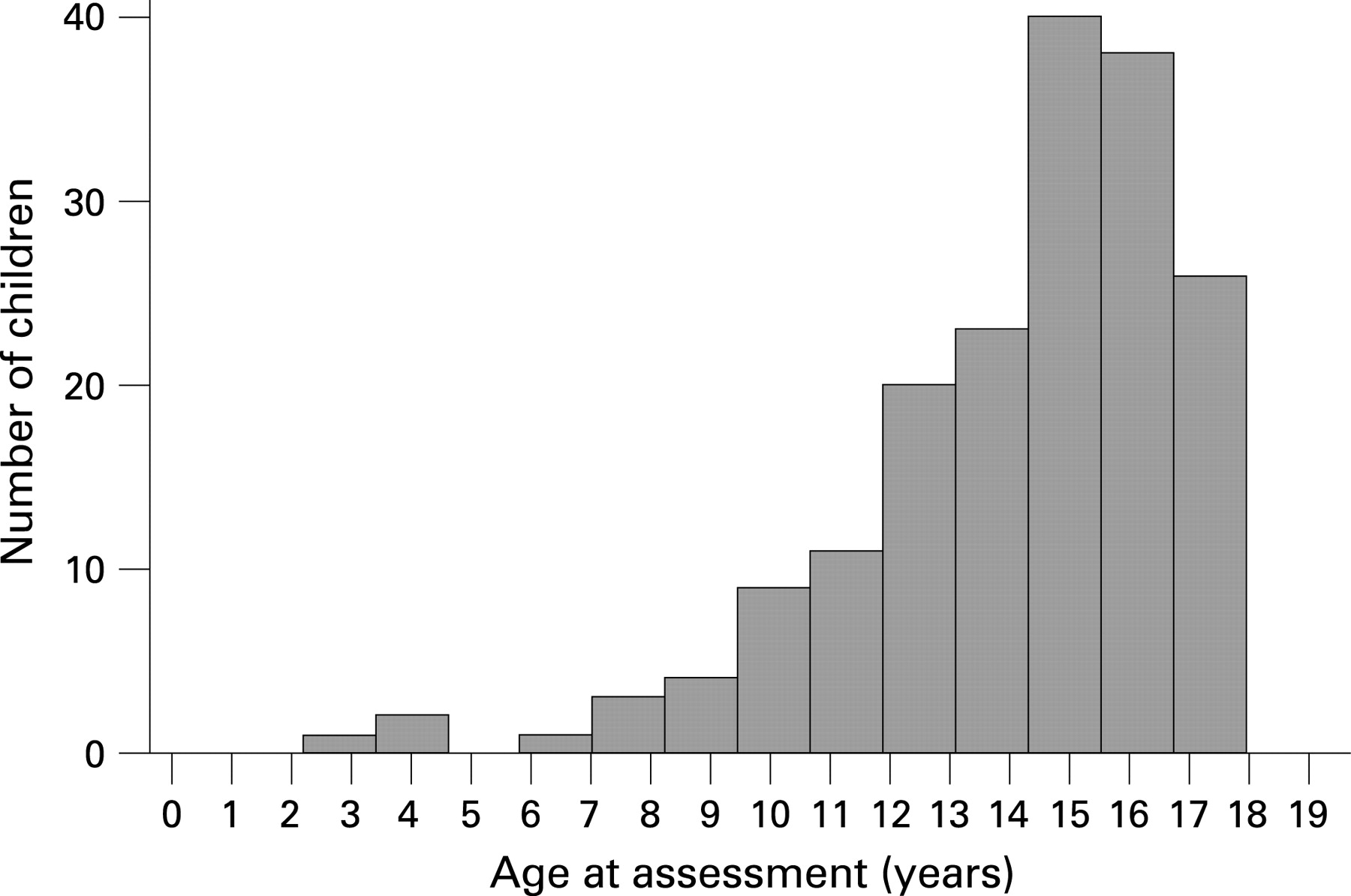
The mean age (SD) at assessment for children with CFS/ME was 14.5 (2.9) years old (SD 2.9). The age distribution for all children attending for assessment is shown in figure 1.
{kind=link}
Of the 40 children assessed who were under 12, 32 (80%) had CFS/ME. Three of these were under 5 years old and the youngest child was 2 years old. Twenty-two (68%) children were female and 30 (93%) children described themselves as White Caucasian. Median time from symptom onset to assessment was 12 months (range 3 to 60 months).
Of the eight children who did not have CFS/ME, five children no longer had fatigue by the time they were seen in the clinic or were not disabled by it; one was given a diagnosis of anxiety; one a diagnosis of chronic pain syndrome and one was undergoing further investigations for alternative causes for fatigue at the time of assessment.
Missing data
The three children who were under 5 were unable to complete the inventories. These children are therefore not included in the analysis of fatigue, pain, anxiety or functional disability. Of the 29 remaining children, three children did not complete any inventories. One additional child did not complete the SF36 scale, one the SCAS, and two did not complete the pain VAS. The poorest inventory for completion was the SCAS. One child missed out nine items and one 17 items, and both these children were excluded from analysis.
Out of 32 children, three did not have a symptom checklist completed, one child had 10 symptoms missing and two children had 13 symptoms missing.
In the children aged 12 and over there were 37 children out of 146 with a diagnosis of CFS/ME who did not return any inventories. Of the remainder who completed some of the inventories, 13 did not complete the Chalder fatigue scale, and in five, there were two or more missing items and so they were excluded. Eleven did not complete the SF36 and four were incomplete (and therefore excluded). The HADS was only sent to children aged 14 and over. In this age group, 43 out of 136 did not complete the HADS. The SCAS was initially used only for children up to 14 years of age up to 2007 but was so useful it was extended to all children seen in clinic in 2007. In children over 12, there were 34 who did not complete the SCAS at all and seven who were excluded because the inventory was incomplete, leaving 68 for analysis.
Those who did not complete any inventories were compared to those who completed some or all of them. There were no differences in age or gender between the two groups.
Analysis of the inventories (table 1) showed that children under 12 were severely affected, with a mean school attendance of just over 40% (average 2 days a week) and a mean Chalder fatigue score of 8.3 (CI 7.14 to 9.4 maximum possible score = 11). They also experienced a significant amount of pain, with a mean visual analogue score for pain of 39.7 (possible range 0–100). The most common symptom experienced was post-exertional malaise (100%), followed by unrefreshing sleep (96%) and subjective memory impairment (80%). (See table 2 for full symptom list.)
Comparison of fatigue, anxiety, pain, functional disability, number of symptoms, time at school and time to assessment between the two groups of children demonstrated that they were remarkably similar in all areas. The younger children appeared to be more anxious and yet attending slightly more school but these results were not statistically significant between the two groups.
Comparison of the frequency of symptoms between the two groups of children demonstrated that the two groups were very similar (table 2). There were no significant differences between either group for any symptom frequency.
Twenty-six children under 12 had completed symptom lists taken at assessment and of these, 24 would have been given a diagnosis of CFS/ME using the stricter criteria for adults from the CDC. The two that would not have been given a diagnosis had not had CFS/ME for 6 months at the time of assessment (3 months and 5 months respectively).
Discussion
This is the first detailed study describing a cohort of primary-school-aged children with CFS/ME. All 32 children fulfilled the RCPCH definition of CFS/ME defined as “generalised fatigue persisting after routine tests and investigations have failed to identify an obvious underlying cause”.1 Twenty-four of the 26 children who had complete symptom lists taken at assessment would also have been diagnosed as having CFS/ME using the stricter CDC definition, which requires you to have 6 months of fatigue and four additional symptoms (see table 3).
Eighteen percent of children with CFS/ME diagnosed using the RCPCH criteria seen during the time period studied were under 12 at the time of assessment. This is consistent with other studies that have reported that CFS/ME is less common in younger children compared with older children.4 8 9
Children under 12 were very similar to those who were 12 and over in symptom presentation but also in fatigue, pain, anxiety, school attendance and functional disability scores.
The youngest child was 2 years old at the time of assessment and a total of four children were under 5 years of age at assessment. Diagnosis of CFS/ME in children under 5 years of age is very difficult as subjective description of symptoms is less reliable. Diagnosis was made on what appeared to be disabling fatigue according to parental report using the RCPCH criteria. In each case, the clinical diagnosis of CFS/ME was made by two paediatricians (referring paediatrician and one of the authors) who were experienced in the assessment and management of CFS/ME. For children under 5, a symptom list was not recorded. In all of the children, the parents had not previously heard of CFS/ME, and all routine screening tests were negative. All four children had extensive investigation to exclude other causes of fatigue and all tests were negative. All four children made a good recovery when they were treated using a family-based graded activity programme.
Limitations of this study
The main limitation of this study is the missing data. This is more of a problem in the older children then in the younger children. However, there were no differences in age or gender between those who completed some or all of the inventories when compared to those who completed none.
CONCLUSION
CFS/ME exists in children under 12 and in children as young as 2 years old. There appears to be no difference in clinical symptoms between children under 12 and older children. The majority of children with CFS/ME in primary school would have had a diagnosis of CFS/ME using the stricter adult CDC criteria.
Acknowledgments
Thanks to Professor Alan Emond and Dr Linda Hunt for help in writing this paper. Thanks to all the families who participated.
Footnotes
Funding: This research was funded by The Linbury Trust.
Competing interests: Dr Crawley is a medical advisor for the Association of Young people with ME (AYME).