Article Text

Abstract
A survey of aetiological investigations arranged on children with severe/profound bilateral sensorineural hearing impairment by ENT consultants and community paediatricians working in audiology is described. Greater routine use of ECG, urine analysis, and ophthalmological assessment is needed, with a more selective approach to other investigations as recommended by the British Association of Audiological Physicians (BAAP) and the British Association of Community Doctors in Audiology (BACDA).
- aetiological investigation
- aetiology
- survey
- hearing impairment
Statistics from Altmetric.com
One in 1000 children are born with a permanent hearing impairment and 50–90% more acquire a hearing impairment in early childhood.1 Investigation aims to identify associated conditions, aid genetic counselling and habilitation, and provide prognostic information and also epidemiological data necessary for surveillance and hearing impairment prevention programmes.
Difficulties, however, arise in arranging appropriate investigations, particularly as the yield of investigations is often low, and also in the timing of the investigations, which are often delayed until parents have accepted their child’s hearing impairment.
Recommendations have been produced to facilitate aetiological investigation.2,3 The British Association of Audiological Physicians (BAAP) and British Association of Community Doctors in Audiology (BACDA) issued guidelines for the aetiological investigation of severe to profound bilateral sensorineural hearing impairment in children in 2002.4 These guidelines indicate investigations, which should be performed on all children (level one; box 1⇓), with further investigations undertaken when indicated from history and clinical findings (level two; box 2⇓).
Level one investigations; to be performed on all cases
Paediatric history
Family history of deafness
Clinical examination
Developmental examination
Family audiograms—1st degree relatives
ECG
Referral to ophthalmologist
Urine for microscopic haematuria
Connexin 26 mutation testing
Cochlea/internal auditory meati imaging
Level two investigations; indicated from history and clinical findings
Serology for congenital infection
Haematology and biochemistry
Thyroid function tests
Immunology tests
Metabolic screen
Renal ultrasound
Clinical photography
Chromosomal studies
Referral to geneticist*
Vestibular investigations*
This study aims to examine current practice of aetiological investigation of severe-profound bilateral sensorineural hearing impairment in Wales.
METHODS
A postal questionnaire enquiring about the use of aetiological investigations in children with bilateral severe-profound sensorineural hearing impairment was sent to all ENT consultants (n = 34) and community paediatricians in audiology (n = 15) working in Wales. The only consultant audiological physician in Wales was one of the investigators and excluded from the survey. A second mailing was sent to non-respondents three months later. The questionnaire is shown in the appendix (see ADC website).
RESULTS
Twenty seven replies were received from the 34 (79%) ENT consultants and from 14 of the 15 (93%) community paediatricians.
Nineteen of the 27 (70%) ENT consultants arranged aetiological investigations. The remaining eight referred children to multidisciplinary clinics or another specialty for aetiological investigation.
Nine of the 14 (64%) community paediatricians arranged aetiological investigations. The remaining five (36%) referred the children to another specialty.
Analysis of the results was based on the 19 ENT consultants and nine community paediatricians who arranged such investigations.
Figure 1⇓ indicates the frequency with which level one investigations (recommended to be performed on all children by BAAP/BACDA) are requested routinely. Community paediatricians reported a high use of visual and developmental assessments, but fewer routinely used cochlea imaging and ECG. ENT consultants were less likely to routinely request level one investigations, particularly ECG and urine analysis. The BAAP/BACDA guidelines4 recommend connexin 26 testing as a level one investigation. However, in this survey we combined genetic testing and referral.

The reported routine use of level one investigations (to be performed on all children) by ENT consultants and community paediatricians.
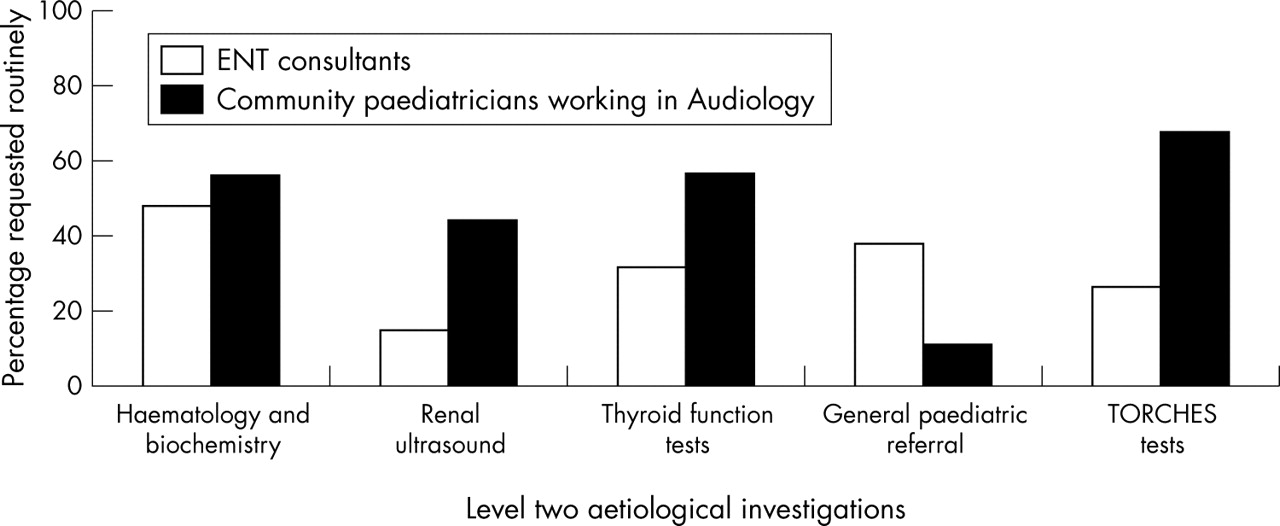
Community paediatricians reported that they routinely request level two investigations more frequently than the ENT consultants, as shown in fig 2⇓.

{kind=link}
{kind=link}
The percentage of level two investigations (undertaken when indicated from history and clinical findings) routinely requested. (The TORCHES acronym of prenatal infections refers to toxoplasmosis, rubella, cytomegalovirus (CMV), herpes simplex, and syphilis.)
ENT consultants showed a preference for referral to paediatricians and audiological medicine, with community paediatricians referring to genetics, ENT, and audiological medicine equally.
DISCUSSION
Aetiological investigation of permanent hearing impairment is, in children, an ongoing process as symptoms emerge and the clinical conditions evolve over time. The causes of childhood hearing impairment have also changed with improvements in neonatal intensive care, advances in genetics, and the introduction of universal immunisation programmes.
Our results show a general awareness of appropriate aetiological investigation of the hearing impaired child. All respondents either arranged such investigations or referred children to colleagues. Cross referral appears to be common practice as is the presence of multidisciplinary clinics in some areas.
When arranging aetiological investigation consideration of the yield, cost benefit and invasiveness of the investigation is required. The need for ECG and urine analysis in all children is particularly important; both these non-invasive tests can be the first indicators of serious underlying pathology, for example, Alport syndrome and Jervell-Lange-Nielsen syndrome.
Approximately 50% of children with a severe to profound hearing impairment have ocular anomalies, the majority being refractive errors.5 Correction of such errors is crucially important to hearing impaired children; visual information is an essential channel of information. Visual examination also provides valuable diagnostic information.
Almost 50% of clinicians reported that they would routinely arrange imaging of cochlea/internal auditory meati (IAM). Imaging is one of the most useful investigations to be performed to establish aetiology.6
Audiological assessment of family members is useful in identifying other affected family members and also in the detection of carriers of genetic hearing impairment.7
The importance of the geneticists in the management of the hearing impaired child is reflected in our results, with 53% of ENT and 89% of community paediatricians in our study reporting that they routinely refer, or perform genetic tests themselves. Advances in genetics have resulted in the identification of several genes implicated in hearing impairment, particularly connexin 26.2
Figure 2⇑ shows that community paediatricians report that they perform more level two investigations routinely than indicated by the BAAP/BACDA guidelines. An extensive review by Bamiou and colleagues6 concluded that haematological and biochemical tests are useful only in the presence of a relevant history (for example, leukaemia, autoimmune disease). Likewise, thyroid function tests only provide useful information in cases with a relevant history. The majority of cases of Pendred syndrome have normal thyroid function tests, with goitre development usually after 10 years of age.8
Vestibular assessment in the hearing impaired child may provide diagnostic information, for example, Usher syndrome, and also allow identification and counselling of children with vestibular failure, particularly with regard to swimming.9
Difficulties have arisen in the usefulness of serological testing; blood samples provide reliable information only when taken in the first six months of life. A recent report using cytomegalovirus (CMV) DNA obtained from Guthrie cards found congenital CMV to be responsible for a significant number of cases of sensorineural hearing impairment with a previous unknown cause.10 With the widespread introduction of universal neonatal screening in the United Kingdom, investigation for congenital infection should provide more useful information and become a prominent part of aetiological investigation.
This report highlights the need for greater use of ECG, urine analysis, and ophthalmological examination in children with severe/profound hearing impairment, as well as a cost effective, evidence based approach as recommended by the BAAP/BACDA guidelines.
Supplementary materials
Web-only Appendix
The appendix is available as a downloadable PDF (printer friendly file).
If you do not have Adobe Reader installed on your computer,
you can download this free-of-charge, please Click hereFiles in this Data Supplement:
Footnotes
Competing interests: none declared