Article Text

Abstract
Background: Better language outcomes are reported for preschool children with hearing impairment (HI) diagnosed very early, irrespective of severity. However, population studies of older children are required to substantiate longer term benefits of early detection.
Aims: To study impact of age of diagnosis and severity of HI in a population cohort of 7–8 year old children.
Methods: Eighty eight 7–8 year old children born in Victoria, who were (a) fitted with hearing aids for congenital HI by 4.5 years and (b) did not have intellectual or major physical disability were studied. Main outcome measures were Clinical Evaluation of Language Fundamentals (CELF) and Peabody Picture Vocabulary Test (PPVT). Predictors were pure tone average (0.5, 1, 2 kHz) in better ear at diagnosis and age at diagnosis. Marginal (adjusted) means were estimated with general linear models.
Results: Response rate was 67% (n = 89; 53 boys). Mean age at diagnosis was 21.6 months (SD 14.4); 21% had mild, 34% moderate, 21% severe, and 24% profound HI; mean non-verbal IQ was 104.6 (SD 16.7). Mean total CELF score was 76.7 (SD 21.4) and mean PPVT score 78.1 (SD 18.1). Age of diagnosis, adjusted for severity and IQ, did not contribute to language scores. In contrast, adjusted mean CELF and PPVT language scores fell sequentially with increasing severity of HI.
Conclusions: More severe HI, but not later diagnosis, was strongly related to poorer language outcomes at 7–8 years. Further systematic study is needed to understand why children with hearing impairment have good or poor outcomes.
- CELF, Clinical Evaluation of Language Fundamentals
- CHIVOS, Children with Hearing Impairment in Victoria Outcome Study
- GLM, general linear models
- HI, hearing impairment
- HL, hearing loss
- POI, Perceptual Organisation Index
- PPVT, Peabody Picture Vocabulary Test
- RPT, Reading Progress Test
- WISC, Wechsler Intelligence Scale for Children
- hearing loss
- child language
- reading
- age factors
- cohort studies
Statistics from Altmetric.com
- CELF, Clinical Evaluation of Language Fundamentals
- CHIVOS, Children with Hearing Impairment in Victoria Outcome Study
- GLM, general linear models
- HI, hearing impairment
- HL, hearing loss
- POI, Perceptual Organisation Index
- PPVT, Peabody Picture Vocabulary Test
- RPT, Reading Progress Test
- WISC, Wechsler Intelligence Scale for Children
Congenital hearing impairment requiring amplification has serious and lasting effects on language development for many children. It has traditionally been diagnosed late.1 With equipment suitable for newborn screening now feasible and available, many countries and states are embracing the philosophy and practice of universal newborn hearing screening.2–,4 Two influential recent studies5,6 build on earlier studies7–,9 in suggesting that very early diagnosis and entry to services improve language outcomes, independent of severity of hearing impairment,5,6 intelligence,5,6 and socioeconomic status.5
However, the published research has important flaws. Most importantly, rigorous epidemiological approaches are needed to minimise selection bias and maximise generalisability. While recruitment within one or two early intervention services offers the opportunity to study within-group outcomes by age of entry, it adequately characterises neither the whole population of children with congenital hearing impairment, nor those who left the service prior to outcome data collection. Secondly, the most persuasive studies5,6 assessed outcomes before children completed their preschool years. Research with profoundly deaf children receiving cochlear implants has established that catch-up can occur at later ages.10 Assessment of longer term outcomes is therefore crucial.
Additional criticisms include the use of parent reported language measures which, while well respected, may be open to serious bias in unblinded studies of the impact of age of diagnosis on outcome.5 Language measures in some studies canvass only limited domains, such as receptive vocabulary6 or intelligibility.7 Not all studies have adjusted for child intelligence,11 despite known correlations of 0.70–0.75 between global cognition and general language abilities in normally hearing children.12,13 Those that included cognitive measures5 did so at an age when IQ is difficult to measure accurately and thus lacks longitudinal stability. Finally, although the foundations of language are laid down in early childhood, language development continues throughout the childhood years; thus it seems important to study outcomes for older, as well as younger, children.
The Children with Hearing Impairment in Victoria Outcome Study (CHIVOS) aimed to address many of these issues. The study targeted an entire state’s population of 7–8 year old hearing impaired children. Access to amplification and early intervention services was available to all. Accurate data on severity of hearing loss and ages of diagnosis and amplification were collected prospectively. Objective measures of cognition and a broad range of language skills were assessed by researchers blind to hearing status and age of diagnosis.
This paper reports on the relation between severity of hearing loss at diagnosis, age at diagnosis, and language outcomes for this cohort. In line with the current literature, we hypothesised that children whose hearing impairment was diagnosed early would have language outcomes superior to children who were diagnosed later, irrespective of severity of hearing impairment or intelligence.
METHODS
Design and participants
This population based cohort study targeted all children born between January 1991 and July 1993 in the state of Victoria (population 4.8 million), Australia, who were fitted with hearing aids by 4.5 years for hearing impairment believed to be congenital. Children were excluded if they had known intellectual disability, if their hearing was now classified as normal, if they had moved interstate, were more than 9.0 years by the time of contact, lived in non-English literate families, or had died.
All Australian children identified with a hearing loss that may require a hearing aid are referred to Australian Hearing, a national, government funded organisation responsible for all paediatric hearing aid fittings. From 1992, Australian Hearing provided data on children fitted with hearing aids to the state’s hearing screening programme. At this time the hearing screening programme comprised audiology referral for infants with risk factors and a universally available behavioural hearing screen at 8–10 months. No universal neonatal hearing screening programme was operating. These data included age at first appointment (used as a proxy measure of age at diagnosis), age at which hearing aids were first fitted, severity of hearing impairment at diagnosis (three frequency pure tone average across 0.5, 1, and 2 kHz in the better ear), postcode, gender, and date of birth. The screening programme’s database provided the sampling frame for this study.
Measures
Standardised assessment measures
Receptive and expressive language skills and receptive vocabulary were assessed with the Clinical Evaluation of Language Fundamentals–Third Edition (CELF)12 and the Peabody Picture Vocabulary Test–Third Edition Form B (PPVT).13 Both are widely used in research and academic settings with both hearing and hearing impaired children,6,14,15 and are supported by a strong literature indicating concurrent and predictive validity and reliability. The Perceptual Organisation Index (POI) of the Wechsler Intelligence Scale for Children–Third Edition (WISC)16 provided a measure of cognition that does not rely on speech processes, correlates highly with full scale IQ in hearing children,16 and is perhaps the most widely used test of child cognition available today, with validity data supporting use of the POI in both hearing and hearing impaired children. Standard scores were calculated for the CELF, PPVT, and WISC (mean 100 and standard deviation (SD) 15 in normative samples).
The Sounds-in-Words subtest of the Goldman-Fristoe Test of Articulation–First Edition17 measures the number of articulation errors occurring in 23 consonant sounds in up to three positions (initial, medial, final) and 12 consonant blends. Inter- and intra-rater agreement and test-retest reliability are high. The Reading Progress Test 1 (RPT1)18 is a simple test of reading comprehension which does not depend on auditory comprehension or writing skills. Though not widely used in research, the RPT1 was selected because we could not find a better test that does not rely on auditory comprehension or written answers (relevant to this population in which many were expected to be on the cusp of literacy). Reading age was divided by chronological age and multiplied by one hundred to produce a standardised score.
Parent and teacher questionnaires
Written questionnaires were completed by a parent and the child’s teacher. Teachers rated intelligibility using Markides’ seven point scale (1 = normal, 7 = no speech).7 As a proxy for parent-child interaction, current family functioning was reported by parents using the 12 item General Functioning Scale of the McMaster Family Assessment Device19 which provides a single score of general family functioning (1 = healthy, 4 = unhealthy). Parents reported on early intervention services, current school based education services, and sociodemographic details.
Hearing status
Severity of hearing impairment in the better ear at diagnosis and at outcome were analysed both as continuous and as categorical variables, using the World Health Organisation three frequency classification20 (mild 26–40 dB HL; moderate 41–60 dB HL; severe 61–80 dB HL; and profound >80 dB HL). Other classifications, which define profound losses more stringently as >90 or >95 dB HL, were not an option here because the Australian Hearing database (which comprised our baseline) did not record acuity at 4 kHz. CHIVOS therefore classified nine children with losses of 81–95 dB HL into the “profound” category, who might otherwise have been in the “severe” category using alternative classifications. However, since in almost all analyses severity was entered as a continuous rather than a categorical variable, this discrepancy would have exerted relatively little impact on our results.
Procedures
Parents provided written informed consent to take part in the study. The study was approved by the Royal Children’s Hospital Ethics in Human Research Committee. Each child took part in one individual three hour assessment with a speech pathologist and a psychologist. Children wore their usual hearing aids and/or cochlear implant; on six occasions a certified sign interpreter assisted. Researchers were blind as far as possible to the child’s hearing status and age of diagnosis during the assessments, though in practice profound losses were often self-evident.
Statistical analysis
The Statistical Package for the Social Sciences Version 10.0 was used throughout. Postcode data enabled comparison of socioeconomic status between respondents and non-respondents using the Education and Occupation Index of the Australian census based Socio-economic Indexes for Areas21 (population mean 1000, SD 100). Occupation was categorised using the Australian Standard Classification of Occupations, then converted using the ANU3_2 Occupational Prestige Scale22 to provide a measure of occupational prestige ranging from 0 to 100 (mean 34.8, SD 23.4).23
Relations between outcome variables and potential predictor/confounder variables were explored using t tests, one way ANOVA, and Pearson correlations for pairs of normally distributed variables, and Spearman correlations where one or both variables were not normally distributed. Goldman-Fristoe scores and teacher-rated intelligibility were slightly skewed. These variables were successfully transformed using a logarithmic transformation to base e. Regression models using the enter method were constructed examining scores on the CELF, PPVT, RPT, and the transformed Goldman-Fristoe and teacher rated intelligibility. Non-verbal IQ, maternal education, paternal occupational prestige, and family functioning were entered first as covariates, followed by the two independent variables of interest, age at diagnosis and severity at diagnosis. Finally, we constructed separate general linear models (GLM) to estimate marginal adjusted mean language and reading outcome scores by (1) severity at diagnosis (categorised) and (2) age at diagnosis (categorised), controlling for significant confounders in the multiple regression analyses.
RESULTS
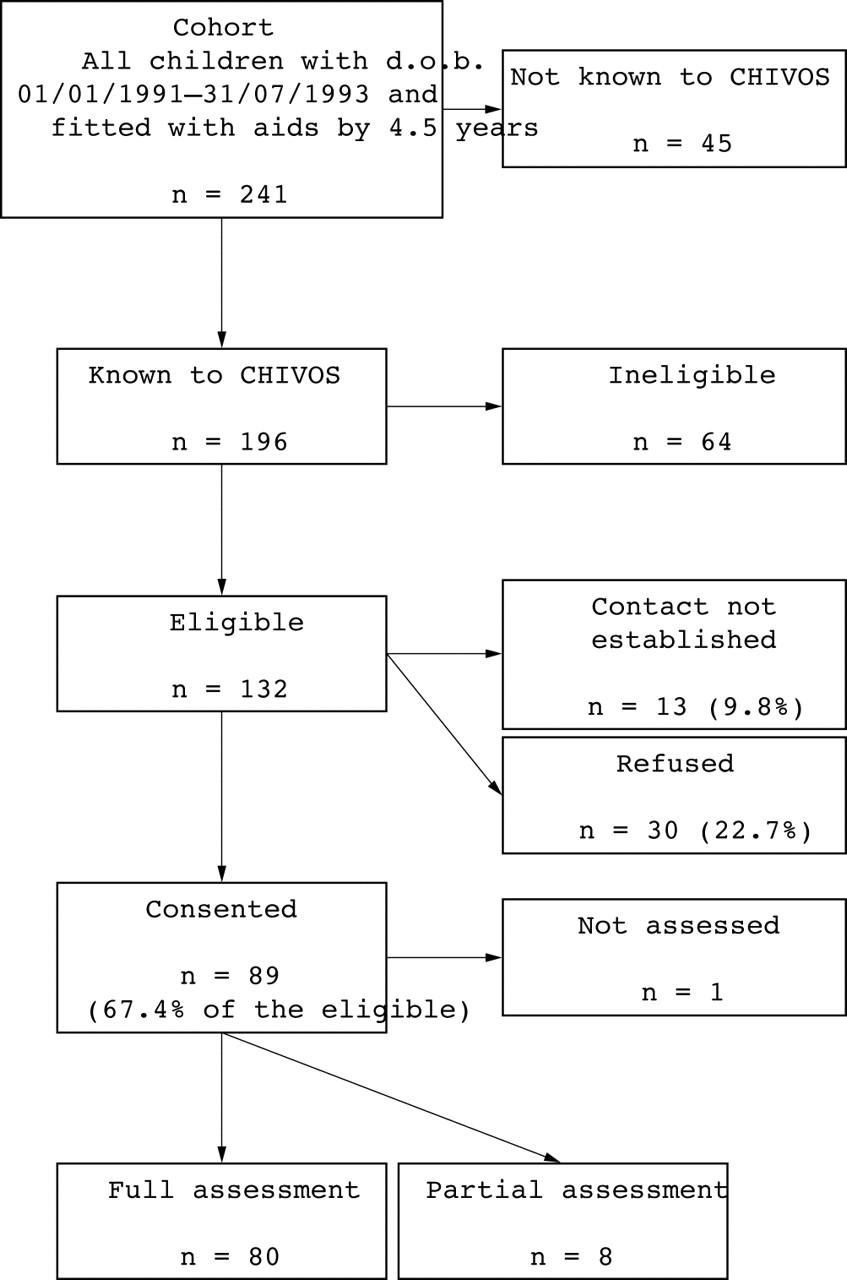
A total of 132 eligible children and families were identified (fig 1⇓). The 89 respondents did not differ from the 43 non-respondents in mean age at diagnosis, mean age at which hearing aids were first fitted, mean severity at diagnosis, gender, or mean Education and Occupation Index score.

Participant flowchart.
After completion of the study, we realised that a further 45 potentially eligible children had not been identified due to a 1997 administrative change in the way Australian Hearing provided data to the hearing screening programme. These children were similar to those approached on all available indices (age at diagnosis, age hearing aids first fitted, severity at diagnosis).
Table 1⇓ shows demographic and audiological characteristics of the sample. On average, 6.1 years had elapsed since diagnosis (SD 1.1, range 3.5–8.1). Eleven children had been diagnosed by 6 months, of whom one had mild, three moderate, four severe, and three a profound loss; 29 had been diagnosed by 12 months, of whom two had mild, eleven moderate, six severe, and nine a profound loss. Mean severity was 65 dB HL at diagnosis (SD 25, range 30–120) and 57 dB HL at outcome (SD 22, range 23–105). On average, children’s acuity remained stable from diagnosis to outcome (mean change = 0.06 dB HL, SD 14, range −27 to +50 dB HL). Fourteen children showed evidence of progression 10 dB HL or greater, with a median change of 17 dB HL (range 12–50), and a further 14 children showed an improvement in hearing levels of 10 dB HL or greater (median 15, range 12–27). Eighty eight per cent of the sample had attended an early intervention service. Forty six per cent were currently attending a school for the deaf or a school with a deaf facility; 93% of those attending a school without a deaf facility had a visiting teacher or teacher’s aide.
Demographic characteristics of the sample (n = 86*)
Diagnosis (mean age 1.8 years) was followed closely by hearing aid fitting (mean age 1.9 years; Pearson’s r = 0.99, p < 0.001), and entry to early intervention service (mean age 2.0 years; Pearson’s r = 0.76, p < 0.001). Age at diagnosis was negatively correlated with severity at diagnosis (Pearson’s r = −0.39, p < 0.001). At outcome, mean non-verbal IQ was 104.6 (SD 16.7); mean total CELF score was 76.7 (SD 21.4); and mean PPVT score was 78.1 (SD 18.1).
Table 2⇓ shows bivariate correlations between outcome measures and potential predictors/confounders. Severity at diagnosis, severity at outcome, and non-verbal IQ were significantly correlated with almost all speech and language measures, but not reading score. In contrast, there were no significant correlations between age at diagnosis or hearing aid fitting and any of the outcome measures. Family functioning did not correlate with any outcome measure. Socioeconomic indicators were only weakly related to outcome measures, the strongest correlation being with the reading score.
Correlations between language and reading measures and potential predictor/confounder measures
Seven regression equations were calculated using the enter method (table 3⇓). Age at diagnosis did not contribute significantly to variance on the language, speech, or reading measures, with the exception the PPVT which approached significance (R2 change = 0.07, p = 0.05). Severity of hearing impairment contributed significantly to the variance in scores on all the language and speech measures, but not the RPT. More severe hearing impairment very strongly predicted lower scores on all language measures, independently accounting for 12–29% of outcome variance. Interaction effects between severity of hearing impairment and age at diagnosis on outcome were sought but not found. Our cohort had a slightly higher proportion of mild losses (21%) than Moeller’s (8%) or Yoshinaga-Itano’s (13%) studies. In case these children unduly influenced our results, we re-ran the regression analyses including only the children with losses >40 dB HL. The findings were unchanged.
Summary of variance explained by regression models predicting language and reading measures at age 7–8 years
In the GLMs, estimated mean language and reading scores did not vary significantly by age of diagnosis, adjusted for severity of hearing impairment and non-verbal IQ (table 4⇓), though we note a tendency for those diagnosed by 12 months to do better than those diagnosed between 1 and 3 years. In contrast, mean scores fell sharply with increasing severity of hearing impairment, adjusted for age at diagnosis and non-verbal IQ (table 5⇓).
Estimated mean* language and reading scores by age at diagnosis, adjusted for severity at diagnosis and non-verbal IQ
Estimated mean* language and reading scores by severity at diagnosis, adjusted for age at diagnosis and non-verbal IQ
Summary of variance explained by regression models predicting language and reading measures at age 7–8 years for children with moderate, severe, and profound losses (excluding children with mild losses)
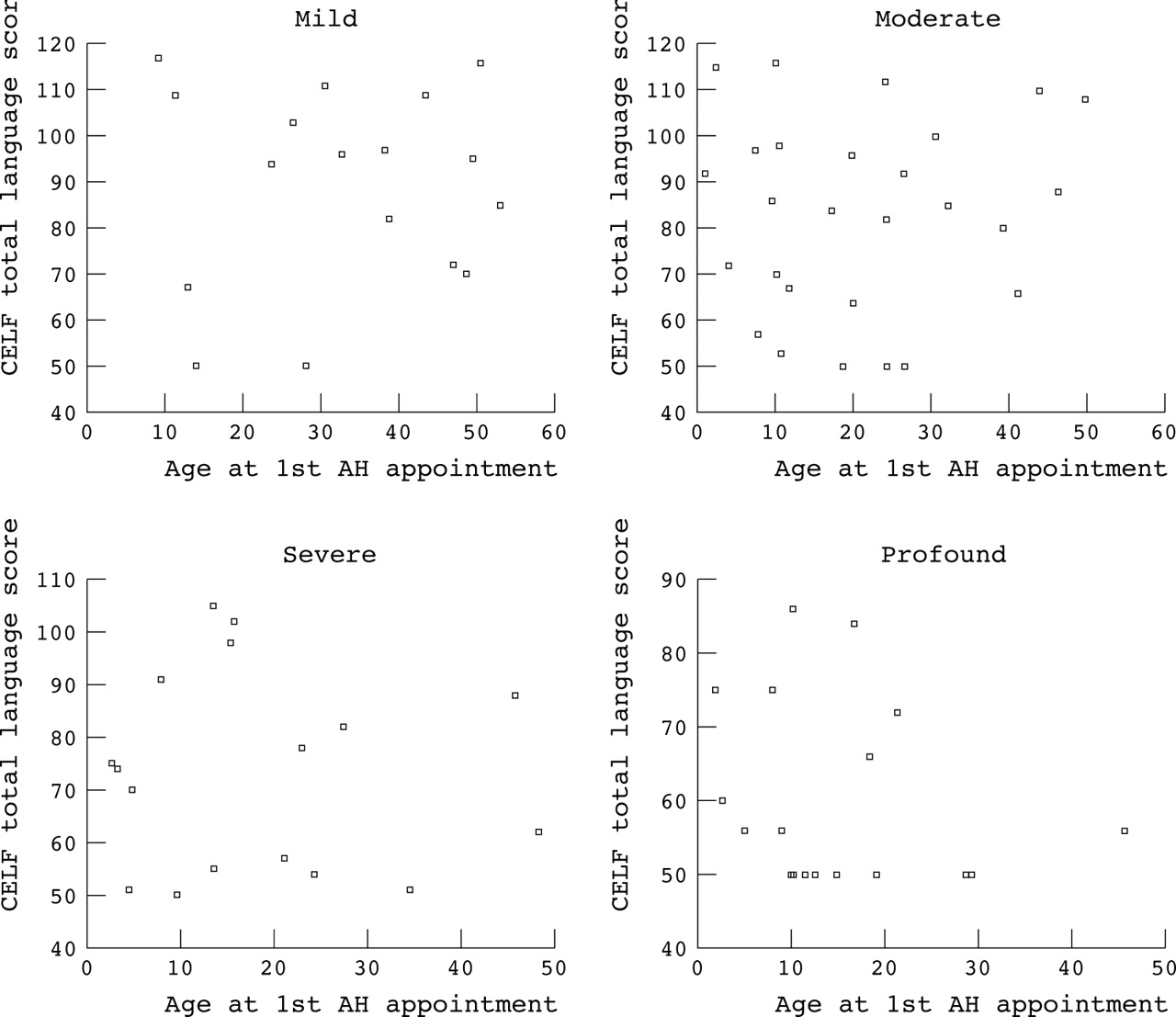
Figure 2⇓ presents scatterplots, stratified by severity, of age at diagnosis by outcome for the CELF. No discernable trends are evident in any of the severity groupings.
{kind=link}
{kind=link}
Scatterplots showing CELF score against age at diagnosis, stratified by severity of hearing impairment.
DISCUSSION
Language outcomes for this cohort of 7–8 year olds with congenital hearing impairment from Victoria were very poor—more than 25 points lower than expected from their IQ scores. In contrast to other studies, we found that these outcomes were strongly and linearly related to the severity of impairment but not to age at diagnosis. How do we interpret these findings?
We have confidence in the quality of our data. The study minimised potential bias through its size, sample selection methods (population based), measurement of predictors (objective and prospective), and measurement of outcomes (objective, standardised, and blinded with respect to the predictors of interest). Likely confounders were considered and where necessary adjustment occurred. Diagnosis was followed rapidly by amplification and early intervention, which was accessed by all but the mildest and latest diagnosed in the cohort. Non-respondents did not differ from respondents on key predictors or sociodemographic indicators.
The main differences between this and previous studies5,6 is that our subjects were older and our study sampled from a geographical, rather than a service based, population. It may be that by age 7–8 years, severity of impairment has prevailed over age at diagnosis—the longer a severe disability is present, the greater its relative impact on outcomes. A population sample may give a different picture to studies conducted entirely within one or two early intervention programmes. Although almost all our children received intervention as soon as the diagnosis was confirmed, this was variable in approach (and presumably intensity) since parents were free to choose which of the available programmes they wished to attend. This is probably similar to the scenarios in most countries, in which a variety of approaches are usually available.
It may be that there were simply too few children in this cohort diagnosed younger than 6 months of age. However, examination of the raw data did not indicate that the 11 children diagnosed before 6 months showed a trend to do better, and in fact those with the best outcomes were diagnosed after 6 months. The most direct comparison that can be made is with Moeller’s study of children with similar numbers, spreads of age at diagnosis and severity, and outcome measures.6 Using a comparable age categorisation, Moeller found a stepwise relation between language outcomes and age at diagnosis, but not IQ or severity; we found the opposite. Nonetheless, the small numbers of cases diagnosed prior to 6 months leaves wide confidence intervals around the outcome figures and therefore leaves the question of possible benefit of very early intervention (made feasible with universal neonatal screening) open.
What is already known on this topic
Better language outcomes have been reported for preschool children with hearing impairment diagnosed very early, regardless of severity of impairment
However, population studies of older children are required to substantiate long term benefits of early detection
Other limitations include lack of a parent-child interaction or family participation measure, which is difficult to assess by this age and in the setting of a non-service based research outcome study. Parents play a vital role in optimising the development of children’s language,24 regardless of hearing status. We doubt addition of a good parent-child interaction measure would have negated the findings, though they may have added to the variance explained. Our family functioning measure did not add to the explanatory power of our models, even though we might expect this to be related to both positive parent-child interaction and family participation. Because we excluded children with intellectual disability, we cannot generalise these findings to such children. While it could be possible that some children who had poorer outcomes were excluded as having “intellectual disability”, we doubt that this is the case since the mean non-verbal IQ (104.6) was equivalent to normative populations, and we found no evidence (such as downward skew) to suggest that performance IQ was altered by the hearing loss itself.
Like other studies, we could not be completely sure that all hearing impairments were congenital. However, the hearing screening programme prospectively recorded whether hearing impairments were believed to be acquired or congenital, and acquired losses were excluded from our sampling frame. Minimal overall progression was measured from diagnosis to outcome, and the prevalence of moderate or greater bilateral hearing loss in our population at age 4.5 years approximates that usually found in universal newborn hearing screening programmes.25 Thus we do not think that inadvertent inclusion of acquired or progressive losses has influenced these findings greatly.
What this study adds
This study addresses many epidemiological flaws of previous studies. In this cohort of intellectually normal children, milder hearing impairment, but not earlier diagnosis, was strongly related to better language outcomes at 7–8 years
Further systematic study is needed to understand why children with hearing impairment have good or poor outcomes, and the effectiveness of different approaches to intervention
In 2001, the US Preventive Services Task Force evidence based systematic review of newborn hearing screening noted important design weaknesses in all published studies examining age of diagnosis and language outcomes.26 In addressing many of these weaknesses, this study did not find the expected relations between earlier diagnosis and better outcomes, even when amplification and prompt intervention were readily available. The strongest evidence continues to indicate that the best outcomes follow very early diagnosis of congenital hearing loss (before 6 months of age). This study, which contained only 11 such children, should not change that conclusion but does sound a note of warning. Countries considering implementing newborn hearing screening should be aware that excellent infant, preschool, and primary school services are also essential if early diagnosis is to reap the desired dividends. They should also systematically monitor outcomes of any new programme well into the primary school years, and not assume that early diagnosis alone translates into long term benefit. Outcome data such as these should provide a baseline against which to measure our successes, an impetus to rigorously study the effectiveness of different approaches, and a mechanism to make long term decisions about the future of newborn hearing screening.
REFERENCES
Footnotes
Funding: Victorian Health Promotion Foundation (1998-0143).
Competing interests: none declared