Article Text

Abstract
Aims: To ascertain the long term outcomes in children diagnosed as having failure to thrive (FTT).
Methods: Systematic review of cohort studies. Medline, Psychinfo, Embase, Cinahl, Web of Science, Cochrane, and DARE databases were searched for potentially relevant studies. Inclusion criteria: cohort studies or randomised controlled trials in children <2 years old with failure to thrive defined as weight <10th centile or lower centile and/or weight velocity <10th centile, with growth, development, or behaviour measured at 3 years of age or older.
Results: Thirteen studies met the inclusion criteria; eight included a comparison group, of which five included children identified in community settings. Two were randomised controlled trials. Attrition rates were 10–30%. Data from population based studies with comparison groups and which reported comparable outcomes in an appropriate form were pooled in a random effects meta-analysis. Four studies report IQ scores at follow up and the pooled standardised mean difference was −0.22 (95% CI −0.41 to −0.03). Two studies reported growth data as standard deviation scores. Their pooled weighted mean difference for weight was −1.24 SDS (95% CI −2.00 to −0.48), and for height −0.87 SDS (95% CI −1.47 to −0.28). No studies corrected for parental height, but two reported that parents of index children were shorter.
Conclusions: The IQ difference (equivalent to ∼3 IQ points) is of questionable clinical significance. The height and weight differences are larger, but few children were below the 3rd centile at follow up. It is unclear to what extent observed differences reflect causal relations or confounding due to other variables. In the light of these results the aggressive approach to identification and management of failure to thrive needs reassessing.
- systematic review
- failure to thrive
- weight faltering
- prognosis
- outcome
Statistics from Altmetric.com
Most child health surveillance programmes both in the West and in poor countries include the regular weighing of infants and young children, with the aim of identifying those children who are growing inappropriately slowly. A variety of cut-off points for action are used, including weight below a particular centile (which ranges from <10th to <0.4th centile) or crossing more than a certain number of centiles. Recently it has been argued that clinicians should use the new charts which identify the slowest growing children while correcting for regression to the mean.1
A small number of children who are identified in this way will be diagnosed as having an organic illness, but over 90% will be labelled as having non-organic failure to thrive.2 A number of explanations have been advanced for this phenomenon of poor growth in early life in the absence of organic disease and in the presence of adequate supplies of food. Child abuse,3 oro-motor coordination leading to feeding difficulties,4,5 and inadequate parenting6 have all been implicated, and there is a widespread assumption that this early poor growth has significant long term effects on children’s growth and development.
A variety of approaches to treatment of failure to thrive have been developed, but there is inconsistent evidence that these improve outcome.7–,9 There is furthermore a clear potential for harm in this situation: failure to thrive is often a pejorative diagnosis, and may instil significant anxiety and feelings of lack of competence within the family.10
Given that there is currently little good evidence from randomised controlled trials that interventions are beneficial in failure to thrive, along with the lack of high quality studies on the effects of growth monitoring programmes on children’s health,11 we aimed to systematically review prognostic studies of children diagnosed as having failure to thrive. We attempted to identify all cohorts of children labelled as having failure to thrive, however diagnosed, that reported measures of growth or psychomotor development at 3 years of age or later, regardless of what interventions were used.
METHODS
Search strategy
Medline, Cinahl, Psychinfo, Web of Science, and Embase databases were searched for cohort studies using the key terms failure to thrive, weight faltering, growth faltering with appropriate synonyms, and mis-spellings, combined with methodological terms including risk factors, prognosis, cohort studies, and outcomes. Randomised controlled trials were also identified for data relating to long term follow up of children in these studies (for this purpose the Cochrane Controlled Trials Register and DARE libraries were also searched). A full search strategy is available from MCJR.
Titles and abstracts identified by electronic searches were examined on screen to select potentially relevant studies. In addition, reference lists of identified studies and review articles were examined. Experts in the field were contacted for unpublished data.
Inclusion criteria
Studies identified as potentially relevant by the searches were reviewed by the authors against the following inclusion criteria:
Population: Children identified as failing to thrive (defined as weight below the 10th or a lower centile, and/or a reduction in weight gain velocity) in the first two years of life in either hospital or community settings
Outcome: At least one outcome measured at the age of 3 years or older, relating to growth, psychomotor development, and/or behaviour
Study design: Cohort studies with or without comparison groups or randomised controlled trials.
Studies were specifically excluded if all participants were children born of low birth weight (<2.5 kg), if they were conducted in countries where malnutrition is prevalent, or if they included children identified as failing to thrive after the age of 2 years.
Data extraction
Data extracted from the studies included case definition, selection of controls, attrition rate, length of follow up, and measures of weight, height, psychomotor development, or IQ and behaviour.
In addition, we recorded whether in those studies with a control group, the outcome assessors were blind to case status, and what attempts had been made to adjust results for potential confounding variables.
Data analysis
The studies were grouped as follows:
Population based studies which attempted to ascertain all cases meeting prespecified criteria
Clinical samples where defined entry criteria were taken to identify children who were inpatients, outpatients, or community referred children.
They were further divided according to whether or not they included a comparison group of children without failure to thrive.
The study details and results were then tabulated within these groups.
Where population based studies included an appropriate comparison group and had comparable methods of outcome assessment and reported data in a usable form, we pooled the results using a random effects meta-analysis. For estimates of weight and height differences, we included only studies that reported standard deviation scores (that is, standardised for age) and their confidence intervals, and performed a pooled weighted mean difference. For measures of psychomotor development or IQ we included studies that used any standardised scale and reported the group means and standard deviation. As these scales have different population means and standard deviations we calculated a pooled standardised mean difference.
RESULTS
Forty seven studies were identified from the searches as being of potential interest,7,9,12–,56 of which 139,12–,23 met the inclusion criteria. Eight were cohort studies,12–17,19 and five were randomised controlled trials.9,18,20,22,23 Of these, eight included a comparison group.12–,19 Study characteristics are described in table 1⇓ for those with a comparison group and in table 2⇓ for those without. The main results are described in table 3⇓ for studies with, and in table 4⇓ for studies without a comparison group. All studies without a comparison group reported results suggesting that children with failure to thrive were shorter, lighter, and scored lower on measures of psychomotor development than population norms, with those recruited as clinical samples generally doing worse. Given the role of potential confounding variables, these studies were not analysed further.
Details of studies with a comparison group
Details of studies without a comparison group
Studies with a comparison group (data expressed as cases mean (SD) versus controls mean (SD))
Results of studies without a comparison group (data expressed as mean (SD))
Quality of studies (tables 1⇑ and 3⇑)
The definition of failure to thrive varied widely across studies with criteria ranging from weights <5th centile to <3rd centile, a fall down 2 centile lines, <80% normal weight and a low thrive index. Attrition rates were 10–30%.
In studies including a comparison group, most selected comparison groups at inception, and were matched for a variety of sociodemographic factors. Blinding was reported for developmental testing in all studies but none reported blinding of assessment of growth.
Growth
Growth data were presented in a variety of forms including standard deviation scores, mean centile position, % normal weight/height, and weight for height, limiting the number of studies that could contribute to the pooled estimates. The data as presented also did not allow for analysis of differing severities of failure to thrive. All studies reported that children who had failure to thrive were lighter and shorter than comparison children at follow up.12–14,16,19 The majority of index children were however above the 3rd centile for both weight and height. Three studies reported that parental height was on average shorter for the cases.14,16,19
Two studies reported weight and height standard deviation scores (SDS)13,16 and were pooled in a random effects meta-analysis. The pooled difference in weight was −1.2 SDS (95% CI −2.0 to −0.5), and in height −0.9 SDS (95% CI −1.5 to−0.3)(fig 1⇓).

(A) Meta-analysis of weight SD scores in children who had experienced failure to thrive in infancy as compared with controls. (B) Meta-analysis of height SD scores in children who had experienced failure to thrive in infancy compared with controls.
Psychomotor development
A variety of measures of psychomotor development and IQ were reported including the Wechsler Intelligence Scale for Children (WISC), McCarthy, Stanford Binet scales, or the Battelle Developmental Inventory. Measures were low overall, but no single study reported a statistically significant difference in IQ between cases and comparisons,12–17,19 although one clinic based study with a comparison group reported that 18% of the sample had learning difficulties as compared with only 3% of controls.19 One study commented that when they adjusted for maternal IQ they found a reduction in differences between the groups,14 and three studies reported a relation between parental education and child’s IQ.17,19,22
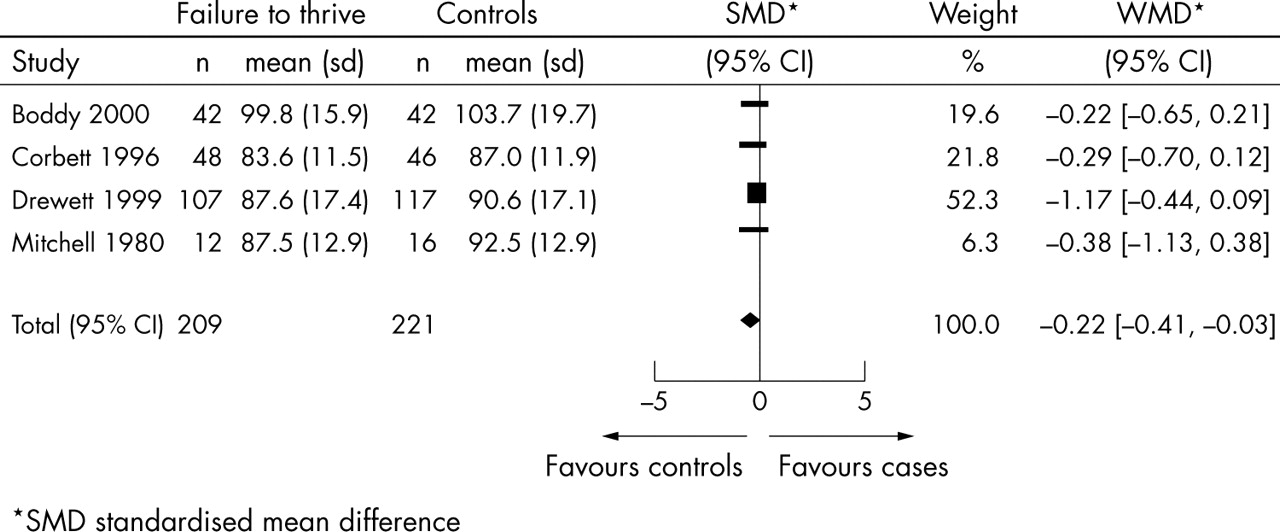
Four studies reported differences between group means and their standard deviations and were included in the meta-analysis.12–14,16 The pooled standardised mean difference in developmental quotient/intelligence quotient was −0.2 (95% CI 0.4 to 0.0)(fig 2⇓). This difference equates to a mean difference of approximately 3 IQ points on the Wechsler Intelligence Scale for children.
{kind=link}
{kind=link}
Meta-analysis of intellectual scores in children who had experienced failure to thrive in infancy compared with controls.
Behaviour
Five studies with a comparison group reported assessments of behaviour.12,13,15,18,19 All used informal questionnaires to teachers or parents. Only one reported an increase in school problems. Three studies13,15,18 reported results on the Child Behaviour Checklist,57 of which only one18 found a difference between the groups.
DISCUSSION
Where convincing evidence of the benefit of intervention is lacking, justification of efforts to identify and treat those with the “condition” must depend on the demonstration of deleterious effects on later outcome. The main finding of this review was the paucity of high quality follow up studies. The population studies which included comparison groups were small, none adjusted adequately for potential confounders (although a number matched on some important variables), and few reported data in a form which allowed inclusion in the meta-analyses. This relative lack of usable data reduces the precision of our estimates of the magnitude of the association between a diagnosis of failure to thrive and long term growth and cognitive development, and means that we cannot entirely exclude quite substantial effects. The heterogeneity of case definition further complicated interpretation, and the data were presented in a way that did not allow for analysis of differing levels of severity. Given this background, the pooled results need to be treated with caution.
What is already known on this topic
Identification of failure to thrive by weight monitoring is a time honoured practice underpinned by the assumption that there are damaging consequences for growth and intellectual development
Considerable stress and anxiety are often precipitated by health professionals when a child is found to be failing to thrive
The aim of systematic reviews is to provide an unbiased estimate of an association by including all studies meeting the inclusion criteria, whether or not they have been published. It is generally believed that location bias is likely to be a particular problem when dealing with observational studies. Although we used an exhaustive search strategy, including asking authors working in the field, we did not find unpublished studies and cannot be entirely certain that we have identified all relevant data.
Results of the included studies suggest that, on average, children identified as having failure to thrive in infancy will be shorter, lighter, and score less well on measures of psychomotor development than their peers. However, the clinical significance of these differences needs to be questioned for a number of reasons, both methodological and clinical.
Although a few of the studies attempted to control for potential confounding variables in their analyses, there is the strong likelihood that residual confounding remains. Some studies commented that “failure to thrive” parents were shorter14,16,19 and one study that parental education was of shorter duration,17 giving some credence to this suggestion.
On clinical grounds, the results also need to be interpreted with caution. Firstly, the pooled difference in IQ scores was relatively small and so of doubtful clinical significance. As regards growth, although the cases were on average smaller than the controls, few children were below the third centile on follow up. As no studies adjusted for parental height, and children were studied during the early primary school years, conclusions regarding final height would be premature. Lastly, some of the children may have had underlying genetic or pathophysiological reasons for poor growth which could affect growth both early in life and later, but should not lead one to conclude that the poor infant growth caused reduced growth in childhood.
Although severe and prolonged malnutrition clearly has profound long term effects on growth and psychomotor development,58 this review provides little good evidence that the growth pattern experienced by children included in the population based studies has serious deleterious effects on subsequent growth or psychomotor development although such an effect cannot be excluded. In most of the included studies, children from both FTT and control groups had relatively low scores on standardised tests of cognitive function at follow up compared to population norms. This suggests that these samples may have been largely drawn from relatively disadvantaged sections of the community.
What this study adds
Failure to thrive is associated with little reduction in IQ, but some reduction in childhood weight and height, although even this may be exaggerated as studies did not adjust for confounding factors such as parental height and IQ
There is little evidence that identifying failure to thrive is predictive of damaging consequences for growth and intellectual development
This conclusion however does not mean that there is no benefit in identifying children who are growing poorly, particularly when there are associated developmental problems or clinical signs and symptoms. Clinical experience suggests that for a small number of children this is a route to the diagnosis of important, remediable organic conditions.2 A further small proportion of poorly growing children may do so as a result of neglect or the deliberate withholding of food, where poor growth can be an important marker for the need for intervention. Finally, this may be a route by which parents who are having difficulties in the management of feeding, or whose children have more general developmental problems, may access care.10
The challenge facing clinicians is how best to identify those children among the slowest growing who would benefit from investigation or intervention, without generating damaging anxiety in those that do not. Bearing in mind that there is currently little robust evidence from randomised controlled trials that intervention is associated with clear long term benefit,7–,9 it is arguable whether screening can be justified, although it remains important that clinicians should respond appropriately to parental anxieties. Yet again, this illustrates the need for randomised controlled trials of interventions that pay careful attention to entry criteria and have adequate long term follow up.
REFERENCES
Footnotes
Competing interests: none
Published Online First 12 May 2005
Linked Articles
- Atoms