Article Text

Summary
The needs of children and adolescents severely affected by chronic fatigue syndrome, myalgic encephalomyelitis (CFS/ME) are currently inadequately addressed in the UK. Sadly, there are few specialists addressing the needs of these patients who are primarily bed-bound, wheelchair users or who can only leave home on an infrequent basis. Uncertainty about what to offer as well of a lack of funding may play a part. Action for Young people with ME (AYME) suggests that at least 350 severely affected children/adolescents are receiving little or inadequate care to help them overcome this debilitating illness. This case report illustrates how recovery can occur with pragmatic rehabilitation combined with a committed compassionate family based approach.
Statistics from Altmetric.com
Background
Chronic fatigue syndrome/myalgic encephalomyelitis (CFS/ME) like any other chronic illness poses a real challenge to healthcare professionals. Although the prognosis of CFS/ME in adolescents is relatively good, a substantial minority of individuals remain disabled for long periods of time.1 It causes significant morbidity at a crucial time in a young person’s growth and development, and causes more time to be lost from school than any other childhood condition. Social, emotional and educational development is significantly impacted upon at a crucial stage of the young person’s life. The consequences of being left untreated are potentially profound with some individuals becoming chronically disabled leading to significant cost for themselves, the family and society. Family life is often disrupted particularly when the young person is too ill to attend school or college. One parent, usually the mother, may give up work to care for their child; this may lead to financial difficulties and feelings of isolation.
There is considerable controversy as to how CFS/ME in children and in adults is best understood and managed. There are those who recommend high levels of rest while others recommend the more conservative approach of ‘pacing’. Two controlled studies have shown CBT to be effective in reducing fatigue and disability in adolescents who are able to attend a hospital setting for out patient appointments.2 3 However, no research to date has focused on the management of severely affected adolescents with CFS/ME. We now describe the treatment of an adolescent boy with CFS/ME who was virtually housebound and who could only mobilise with the aid of a wheelchair.
Case presentation
George, a previously healthy 11-year-old boy who played tennis at a national level, was referred to the Chronic Fatigue Syndrome Research and Treatment Unit at the Academic Health Sciences Centre at King’s College Hospital, following an 18-month illness. George became unwell following a stomach bug that he developed abroad on holiday. Over the next 2 months, he experienced abdominal pain and was referred to a paediatrician; stool tests were normal. An abdominal x-ray showed moderate faecal loading; lactulose relieved his constipation but pain continued. He gradually became mentally and physically fatigued with profound muscle weakness. Investigations to exclude other diagnoses were carried out, including the following: FBC, ESR, U&E’s, LFT, calcium, albumin, creatinine kinase, thyroid function tests (TSH and free T4) local celiac screen (eg, IgA endomysial autoantibodies), random blood glucose and urine analysis for blood, sugar and protein.
During the next few months, he became less mobile and unable to walk and developed severe and frequent headaches along with fatigue. A diagnosis of CFS/ME was made and shared with the family by a consultant paediatrician 1 year before referral to the CFS unit. The diagnosis of pervasive refusal syndrome was suggested by a clinical psychologist. Previous treatments that had not been effective included homeopathy, anti-depressant medication, cranial osteopathy, a 2-week inpatient stay to try to resolve his difficulty with feeding, some sessions with a clinical psychologist and a dietician. Physiotherapy sessions were of some help, but he had a worsening of symptoms following an increase in the time he was standing for. This resulted in him avoiding standing for fear of causing a further deterioration. The severity of his symptoms and level of disability inhibited him from attending the out-patient department and so a home-based assessment and treatment package was arranged with the primary care team.
Treatment
At assessment, George spent most of the time lying down and was only able to sit up or tolerate conversation for a few minutes. Most of the information gathered therefore was taken from his parents. He was unable to walk; he used a wheel chair around his home and rarely left the house. His father had taken early retirement in order to help provide good consistent care with his mother and they had both reduced their social activities. A cognitive-behavioural model of understanding George’s problems was discussed with his parents and a self-help treatment manual was given. Diaries were given to his mother to complete on his behalf to get a detailed picture of his sleep routine and the type and amount of activity and rest he was taking during the day. Self-report measures relating to fatigue4 and social adjustment5 were given before treatment, at discharge from treatment and at 6, 12 and 36 months post treatment.
George had 25 home-based sessions, each lasting between 1½ and 2 h over 18 months. He had follow-up appointments at 3, 6 and 12 months after discharge. Sessions consisted of encouraging him to establish a consistent pattern of activity and rest, then gradually increasing activity and establishing a sleep routine. Fearful thoughts about engaging in activity, for example, standing and walking, were addressed by agreeing specific behavioural experiments to test out the validity of them. Later sessions addressed management of setbacks and preparing for the future. Homework was planned and reviewed in each session. During early sessions, most of the time was spent with George’s parents, but as his symptoms reduced, he became more involved in the decision-making process.
A number of issues related to living with someone with a debilitating illness were addressed; these included parental concerns about contributing in some way to the onset and maintenance of his illness, the effects of the illness on the family and how best to address individual needs and how to work together collaboratively to aid George’s recovery. In addition, as George made progress, issues about encouraging his independence, re-integrating him back into school and gradually resuming previous social activities that had been reduced as a result of looking after George were discussed. A key factor in treatment was engaging George and his parents in the treatment process. This began before the assessment appointment in the form of a telephone call to discuss how George and his parents would like the session to be conducted in view of his severe symptoms. It was important to convey a good understanding of the illness to allay possible fears of being pushed too hard and to develop trust in the approach. Each session involved time to discuss things other than treatment issues, such as hobbies, interests and events that had taken place between appointments or that were forthcoming; this created an environment in which a positive therapeutic alliance developed. As rapport and trust in the therapist built up, George and his parents felt able to discuss their concerns openly; this facilitated a resolution of problems as they arose.
During the first few months of home-based sessions, a community physiotherapist was involved in George’s care. She helped him to develop stamina by encouraging stretching and strengthening exercises and provided aids, for example, a wheelchair. He also did aqua-aerobics weekly. We liaised regularly to ensure a consistent approach was being adopted. A home tutor helped George with school work and helped with his transition to school.
Outcome and follow-up
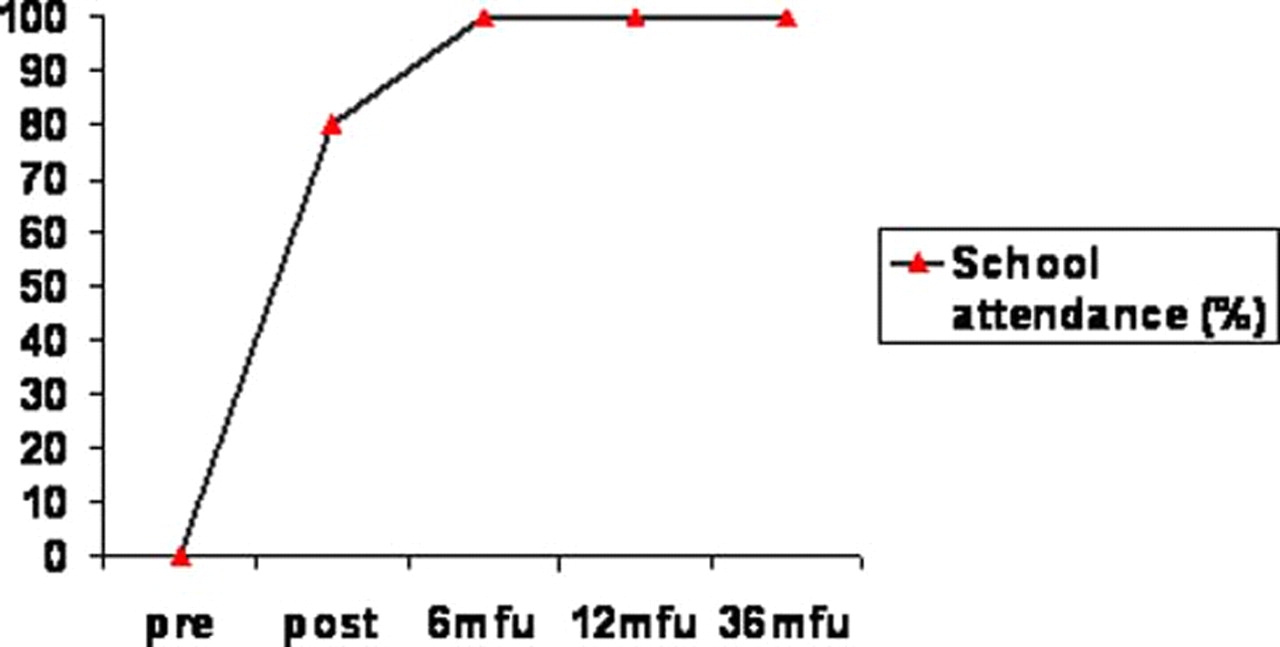
At discharge, after 23 home-based sessions over 19 months, George was back at school full-time but was not participating in sports. At 3-month follow-up, his parents felt that he was ‘back to normal’. Gains were maintained at 6 and 12 month follow-up. At 36 months post discharge, treatment questionnaire scores revealed that gains previously made had been maintained (figure 1). He had achieved good grades in his GCSE’s and was studying for A levels. By 54 months after the end of treatment, (September 2010), his mother informed me that he had achieved good A level results and had won a sports scholarship to a top university in the UK (figures 1 and 2).

Fatigue and social adjustment scores over time.
{kind=link}
{kind=link}
School attendance scores over time.
Discussion
Severely affected adolescents with CFS/ME can make a full recovery from this debilitating illness with time, patience, a clear explanation of factors contributing to the illness, clear pragmatic advice and a collaborative approach. Building a strong therapeutic alliance with the patient and family is essential as the treatment process can be very challenging for them, and emotions may run high particularly when set-backs occur. It is important for one professional to take the lead in the care to ensure good communication and consistency. A long-term commitment possibly over several years is necessary for the likelihood of success to occur. Although the National Institute for Clinical Excellence (NICE, 2007)6 have made some general recommendations for working with children and adolescents, increased time, effort and financial support needs to be focused on developing and training professionals to help this largely ignored group. In addition to becoming more skilled at helping those who are severely affected, it is imperative that professionals become skilled at early detection and management to prevent patient’s developing profound disability.
Learning points
▶ Severely affected adolescents with CFS/ME can make a full recovery.
▶ Long-term commitment by professionals possibly over several years is necessary for the likelihood of success to occur.
▶ Professionals need to become skilled at early detection and management of children and adolescents with CFS/ME to prevent the development of profound disability.
Acknowledgments
The authors would like to thank the patient and family referred to in this paper for giving their permission to write up this case.
Footnotes
-
Competing interests MB and TC are authors of overcoming chronic fatigue published by Constable and Robinson. TC is the author of Coping with chronic fatigue. Sheldon Press. London and Chalder T & Hussain K. (2002) Self Help for Chronic Fatigue Syndrome. A Guide for Young People. Blue Stallion Publication. Oxon.
-
Patient consent Obtained.