Article Text

Abstract
Objectives Data on the incidence of symptomatic osteoarthritis (OA) are scarce. We estimated incidence of clinical hip, knee and hand OA, and studied the effect of prevalent OA on joint-specific incident OA.
Methods SIDIAP contains primary care records for>5 million people from Catalonia (Spain). Participants aged ≥40 years with an incident diagnosis of knee, hip or hand OA between 2006 and 2010 were identified using International Classification of Diseases (ICD)-10 codes. Incidence rates and female-to-male rate ratios (RRs) for each joint site were calculated. Age, gender and body mass index-adjusted HR for future joint-specific OA according to prevalent OA at other sites were estimated using Cox regression.
Results 3 266 826 participants were studied for a median of 4.45 years. Knee and hip OA rates increased continuously with age, and female-to-male RRs were highest at age 70–75 years. In contrast, female hand OA risk peaked at age 60–64 years, and corresponding female-to-male RR was highest at age 50–55 years.
Adjusted HR for prevalent knee OA on risk of hip OA was 1.35 (99% CI 1.28 to 1.43); prevalent hip OA on incident knee OA: HR 1.15 (1.08 to 1.23). Prevalent hand OA predicted incident knee and hip OA: HR 1.20 (1.14 to 1.26) and 1.23 (1.13 to 1.34), respectively.
Conclusions The effect of age is greatest in the elderly for knee and hip OA, but around the menopause for hand OA. OA clusters within individuals, with higher risk of incident knee and hip disease from prevalent lower limb and hand OA.
- Osteoarthritis
- Epidemiology
- Health services research
Statistics from Altmetric.com
Background
According to national health survey statistics (Catalan Health Survey 2011), self-reported osteoarthritis (OA) is highly common in the population of Catalonia (Spain): 46% and 21% of women and men aged 45 years and over in the region respectively report suffering OA.1 Cohort studies carried out in Spain have shown a high prevalence of knee and hand OA of 10% and 6%, respectively.2 OA has a huge impact on healthcare costs: in Spain, costs of knee and hip OA were of more than €4700 million in 2007, equivalent to 0.5% of the national gross national product that same year3
Despite this, national data on incidence of OA are lacking, and studies are scarce even in the international context. Although estimates of incident OA have been published for other populations, most of these reports focused on radiographic OA,4 ,5 which is much more common but less clinically and economically relevant than symptomatic OA.6 Only one of these studies explored the epidemiology of hip, knee and hand OA in the same cohort.7
Women have consistently been shown to be at higher risk of hip, knee and hand OA, and some studies have even reported a lower joint space width and higher narrowing in women.8 Whether this increase in risk is constant with age or changes in relation with endogenous oestrogen production and menopause is unclear.9 ,10
We used a large population-based database to characterise the risk of incident OA related to age, gender and OA at other joints by: (1) estimating age and gender-specific incidence rates (IRs) of clinically diagnosed knee, hip and hand OA in actual practice conditions, and (2) studying the effect of a previous history of knee, hip and hand OA on risk of future incident joint-specific OA.
Methods
Study design
Population-based, retrospective cohort study.
Study population
General practitioners (GPs) are responsible for primary healthcare, long-term and most short-term drug prescriptions, and referrals to specialists and hospitals in Spain. The Spanish public healthcare system is universal, covering the practical totality of the population. The data for this study were obtained from the Sistema d‘Informació per al Desenvolupament de l‘Investigació en Atenció Primària (SIDIAP) database. SIDIAP (http://www.sidiap.org) comprises of anonymised primary care electronic medical records of a highly representative sample of patients attending GPs in Catalonia (North-East Spain), covering a population of about 5 million patients (80% of the total population) from 274 primary care practices and with a total of 3414 participating GPs. SIDIAP comprises of the clinical and referral events registered by primary care health professionals in medical records, comprehensive demographic information, prescription and corresponding pharmacy invoicing data, specialist referrals, primary care laboratory test results, hospital admissionsand their major outcomes.11 Health professionals gather this information using International Classification of Diseases (ICD)-10 codes and structured spreadsheets designed for the collection of relevant variables such as country of origin, gender, age, body mass index (BMI), smoking and drinking status, blood pressure measurements, etc. Encoding personal and clinic identifiers ensures the confidentiality of the information in the SIDIAP Database. All participants aged ≥40 years old with no history of OA at index joint on 1 January 2006 were eligible for this study. Study participants were then followed up until the end of the study (31 December 2010), transfer out or death date, whatever came first.
Ascertainment of clinically diagnosed osteoarthritis
Date of incident diagnoses of OA registered in the period from 1 January 2006 to 31 December 2010 in the study population were identified using ICD-10 codes for the following: knee OA (M17, M17.0, M17.1, M17.2, M17.3, M17.4, M17.5 and M17.9), hip OA (M16, M16.0, M16.1, M16.2, M16.3, M16.4, M16.5, M16.6, M16.7 and M16.9) and hand OA (M15.1, M15.2, M18, M18.0 to M18.5 and M18.9). Data on OA coding within SIDIAP have been validated against self-reported OA in the Global Longitudinal Study of Osteoporosis in Women (GLOW) population-based cohort.12 SIDIAP does not contain data on laterality of the joint affected, and therefore joint site (eg, knee) is considered here as a whole.
Validation of OA diagnosis in SIDIAP
Previous studies have shown that an OA diagnosis in SIDIAP is highly correlated with self-reported OA (sensitivity 71% (95% CI 69% to 73%), specificity 94% (95% CI 92% to 95%)) in the GLOW cohort.12 To explore this further, we reviewed free text from the medical records of a random sample of 150 study participants with a newly registered OA code. We extracted any free text introduced in the primary care records in the 3 months before and after the date of an OA diagnosis. Then, we have used automatic natural language chain methods to anonymise the extracted text. Finally, one of the investigators, with a medical background and extensive knowledge of the Catalan and Spanish language (DP-A) reviewed this text to identify: (1) mention of an x-ray report and (2) an alternative diagnosis.
Age and gender measurements
Age at cohort entry (on 1 January 2006 or first registration date in SIDIAP) was calculated based on date of birth, which was obtained from ID card or passport as well as gender.
Statistical analyses
Age (in 5-year groups) and gender-specific IRs (and 99% CIs) in the study period were estimated. Age-specific female-to-male rate ratios (RRs) (and 99% CIs) were calculated using Poisson regression.
Survival analysis methods were used to model time from study initiation (1 January 2006) or date when the patient registered in one of the primary care practices covered by SIDIAP (whatever came last) to the date when the first of these events occurred: joint site OA diagnosis, date when the patient transferred out of the area, date of death, or date of end of study (31 December 2010). Cox regression modelling was used to compute adjusted (for age, gender and BMI) HRs and 99% CIs for an incident clinical diagnosis of hip and knee OA according to prevalent joint-specific OA status. As a proportion of participants had missing information for one of the confounders (BMI), we created a category for patients with missing values in order to avoid dropping these patients in the multivariable analysis. All the statistical analyses were carried out using Stata SE for Mac V.12.0.
Results
After excluding SIDIAP participants aged <40 years, 3 266 826 participants were observed for a median (IQR) of 4.45 (4.19–4.98) years. Among these, 96 222, 30 350 and 37 590 incident cases of knee, hip and hand OA were identified respectively. In addition, 4492 patients developed incident hip and hand OA, 14 171 knee and hand OA, 14 585 knee and hip OA, and 1391 people developed incident OA at these three sites during the observation period. Baseline characteristics for these three groups and for patients with no prevalent or incident OA are shown in table 1. New cases of hand OA were younger, more likely to be women, thinner, and had fewer comorbidities than participants with newly diagnosed knee or hip OA.
Baseline characteristics of study participants
Among the reviewed medical records extracts for 150 participants with an incident OA diagnosis, 59 (39.3%) had evidence of an x-ray confirmation, and only 2 (1.3%) patients had an alternative diagnosis (1 polymyalgia rheumatica and 1 senile rheumatoid arthritis).
IRs (99% CIs) of knee OA were 6.5/1000 person-years (6.4–6.6) overall, 8.3/1000 person-years (8.2–8.4) for female participants, and 4.6/1000 person-years (4.5–5.7) for men. Similarly, IRs of hip and hand OA were: 2.1 (2.0–2.1) and 2.4 (2.4–2.4) overall, 2.4 (2.4–2.5) and 3.5 (3.5–3.6) for women, and 1.7 (1.7–1.8) and 1.3 (1.2–1.3) among male participants. Age and gender-specific IRs of knee, hip and hand OA are shown in figure 1 (and online supplementary tables ST1, ST2 and ST3, respectively). In female participants, rates of knee and hip OA increased progressively with age, with a steepest slope in the ages 50 years to 70 years, which then slowed down and peaked at 75–80 years and at 80–85 years, respectively, with a slight decrease in the final years of life (age 85 years and older) (figure 1A,B). In contrast, IRs of hand OA in women increased more rapidly at earlier ages (40–45 years onwards) peaking at 60 years and then decreased in the elderly (>65 years) until reaching a trough at age 80–85 years to increase again in the last years of life (>85 years) (figure 1C). Rates of knee, hip and hand OA followed a more similar pattern in men: IRs increased continuously with age, and peaked only in the oldest ages (>85 years).

Age and gender-specific incidence rates (/1000 person-years) of knee osteoarthritis (OA) (black), hip OA (red), and hand OA (green). Solid, All population; short dash line, women; long dash line, men.
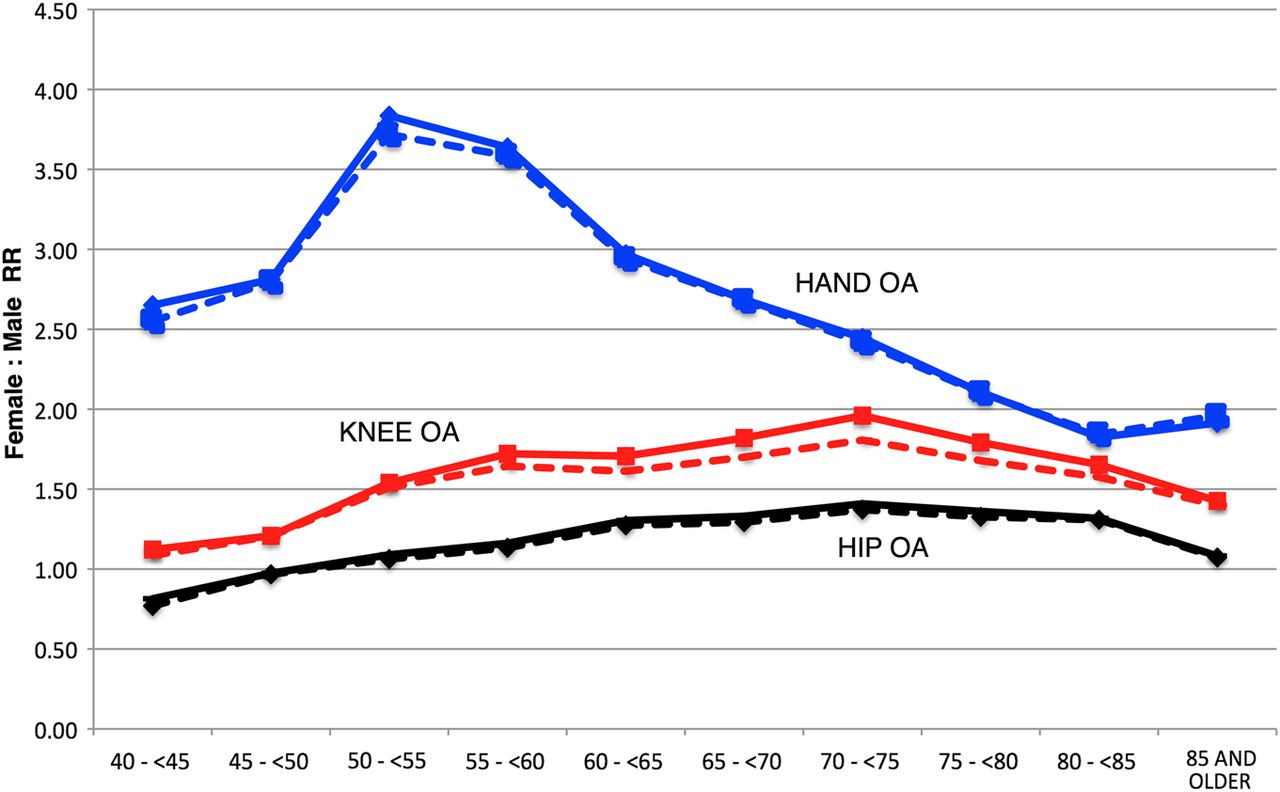
Risk of all three joint-specific OA appeared overall higher in women: adjusted RRs 1.52 (1.47–1.54, p<0.001) for knee OA, 1.19 (1.15–1.23, p<0.001) for hip OA and 2.50 (2.38–2.56, p<0.001) for hand OA. However, different age patterns for the gender effect were observed (figure 2). Women appeared at higher risk of knee OA from age 45 years onwards (adjusted RR 1.21 (1.17–1.25), p<0.001 for participants aged 45–50 years), and the gender-related excess risk increased progressively peaking at age 70–75 years (adjusted RR 1.81 (1.76–1.86), p<0.001) to decrease slowly in the final stages of life. Hip OA followed a parallel pattern but starting at older ages: women had lower rates of hip OA than men in their 4th decade of life (adjusted RR 0.77 (0.73–0.81, p=0.006) in the 40–45 years), and risk was only increased for women aged 55 years and older (adjusted RR 1.13 (1.06–1.20), p=0.001 in those aged 55 years to <60 years); this excess risk increased with age reaching a peak among participants aged 70–75 years (adjusted RR 1.37 (1.32–1.42), p<0.001), and then slowly decreased to approximate male rates in the oldest ages. As for hand OA, the effect of gender was noticeable from the youngest ages (adjusted RR 2.55 (1.89–3.21), p<0.001 in participants aged 40 years to 45 years), peaked at age 50–55 years (adjusted RR 3.72 (3.43–4.01), p<0.001) and then decreased with age, more steeply in the range of 60 years to 80 years (figure 2).
{kind=link}
{kind=link}
Age-specific unadjusted (solid) and multivariate adjusted (dash) female-to-male rate ratios (RRs) for knee, hip and hand osteoarthritis (OA).
Results for Cox regression models on the effect of previous OA on incident hip and knee OA were as follows: previous hip or hand OA were related to incident knee OA (age and gender-adjusted HR 1.36 (1.28–1.45), p<0.001 and 1.47 (1.40–1.54), p<0.001, respectively) independent of BMI (further BMI-adjusted HR 1.15 (1.08–1.23), p<0.001 for prevalent hip OA and 1.20 (1.14–1.26), p<0.001 for previous hand OA). Similarly, knee or hand OA predicted future hip OA, with age and gender-adjusted HR of 1.66 (1.58–1.75), p<0.001 and 1.41 (1.30–1.53), p<0.001, respectively. This stood for further adjustment for BMI: HR 1.35 (1.28–1.43), p<0.001 for previous knee OA, and HR 1.23 (1.13–1.34), p<0.001 for a history of hand OA (tables 2 and 3).
Effect of prevalent hip and hand OA on risk of knee OA
Effect of prevalent knee and hand OA on risk of hip OA
Discussion
Key results
We report for the first time population-based estimates of incidence of clinically diagnosed knee, hip and hand OA among men and women aged 40 years and older in a Southern European/Mediterranean nation (Catalonia).
We show that the effects of age on hip and knee OA risk in women follow similar patterns, increasing rapidly between ages 50 years and 75 years, and then decreasing in the oldest. Conversely, risk of incident hand OA peaks in women after typical menopause ages (55–60 years) and then plateaus, decreasing eventually in the elderly. Age-specific incidence of knee, hip and hand OA follow parallel trends in men, increasing continuously with age until the last stages of life. Gender-related excess risk for hip and knee OA is fairly stable with age, increasing slowly from 50 years to 70–75 years, and then decreasing in the oldest ages. By contrast, the effect of female gender on risk of hand OA peaks around menopause, with more than 3.5-fold higher rates in women aged 50 years to 60 years when compared with men of similar age. At older ages, the effect of age on hand OA risk attenuates, approximating to the effect of female gender on knee OA among those aged 80 years and older. Finally, we demonstrate that a history of hand OA is associated with increased risk of hip and knee OA, and that previous knee OA is related to higher risk of hip OA and vice versa, independently of age, gender and BMI.
Interpretation/put in context
Studies on incidence of OA are scarce, and it has been recognised that different definitions of disease make comparisons between them difficult. Most studies have reported estimated rates of either radiographic OA (usually defined by a Kellgren & Lawrence score ≥2),4 ,13–17 or symptomatic OA (radiographic OA accompanied by typical OA symptoms), and some have studied self-reported OA.18 Although heterogeneity in case definition is always present, reliability problems have been raised particularly for radiographic studies,16 with studies on symptomatic OA offering more homogeneous and comparable results.19 Although we used a different definition of OA based on physician diagnosis, our estimates of incidence are comparable with other cohorts: as an example, IRs of symptomatic knee OA were 6/1000 person-years in the study by Kannus et al20 conducted in Finland, 10/1000 in the Framingham cohort,21 7.3/1000 in the Norwegian population,18 7.6/1000 in Japan17 and 6.5/1000 in our data. Clinically diagnosed OA is most important with relation to patients’ quality of life and healthcare costs.
Only some of the incidence studies published had enough power to estimate age-specific IRs, and register-based studies similar to ours did not report joint-specific estimates.22 ,23 The few papers reviewed demonstrated a continuously increasing risk of knee and hip OA after the age of 40 years for both genders, peaking at ages around 75–80 years, close to our results.7 ,17 ,24 By contrast, the differing patterns for hand OA in women versus men observed in our study have been shown in some studies, but not all: while Oliveria et al7 showed continuously increasing risk until the age of 80 years, recent estimates from the Framingham cohort have suggested a peak in hand OA incidence around menopause, probably due to erosive hand OA, which appeared most commonly at the age of 50–55 years in that same population.25
The effect of female gender on the risk of OA has been estimated in a number of studies13 ,26 ,27 and even compiled in a meta-analysis,28 but the interaction with age has not been explored in the past. Our estimates of adjusted female-to-male age-specific risk ratios hence cannot be compared with previous publications, but crude estimates can be calculated based on the information provided in some of the papers in press: while a gender effect would increase slowly in hip and knee OA,7 ,17 the highest excess risk related to female sex seen around typical menopause ages (up to 59 years) on hand OA is consistent with previous reports.7 ,25 We speculate that this suggests a stronger effect of hormonal status on hand than on lower limb OA, which might at least partially explain the controversial results obtained from clinical trials on the effect of hormone replacement therapy on OA, which focused on knee and hip disease.29 ,30 Alternatively, gender differences in health-seeking behaviour (eg, women being more dissatisfied with hand deformity), or a higher awareness of hand OA in women patients by GPs could explain this finding.
Data on the association between prevalent OA at one joint and incident symptomatic disease at others are scarce. Contrary to our results, Felson and Cols reported no association between previous hand OA and incident knee OA in the Framingham cohort,15 but other authors have demonstrated that there is an association between hand OA and knee31–33 and hip OA.31–34 Even a recent study has shown that hand joint space narrowing predicts MRI-based knee OA traits.35 The effect size (HR) of the associations described are ostensibly attenuated when adjusted for BMI in our data, suggesting that mechanical loading is important but does not fully explain the pathogenesis of OA. Unobserved variables (genetics, joint shape, pain perception, etc) could explain this BMI-independent association.
Strengths and limitations
Strengths of our study are a big sample size, allowing us to study the interactions between gender and age on joint-specific OA risk, and the representativeness of the information gathered, which covers >80% of the population of the region. However, we are uncertain whether these findings are generalisable to other (eg, Northern European, American) populations.
The impact of the disease is predominantly due to cases with clinically symptomatic disease seeking medical attention, which drives the impact on patient symptoms as well as the pharmacy or surgery interventions and healthcare-related costs.
The main potential limitation of these data is the lack of validation of each individual diagnosis of OA, but previous cross-validation against classical cohort data have shown OA coding in SIDIAP to be highly specific.12 In addition, although x-ray imaging is not required for the diagnosis of OA,36–38 we found evidence of radiological confirmation of the diagnosis in almost 40% of a random sample of 150 cases. Only about 1% of these patients had an alternative diagnosis close to the date of OA coding. All this suggests a high reliability of the recording of OA in SIDIAP.
Conclusions
The incidence of knee and hip OA increases continuously with age for both genders, while hand OA risk peaks around menopause in women. Related to this, the gender-related excess risk observed for hand OA is highest at the age of 50–55 years, with a maximum increase of almost fourfold for female patients compared with male patients. Further investigations are required in order to clarify the potential mechanisms underlying this interaction.
In addition, we demonstrate a BMI-independent association between previous hand OA and incident knee and hip OA, supporting a systemic background for OA disease.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online tables
Footnotes
-
Handling editor Tore K Kvien
-
DP-A and AJ are joint first authors. AD-P and NKA are joint last authors.
-
Contributors Data acquisition: DP-A, AD-P. Data analysis: DP-A. Data interpretation and manuscript preparation: all authors.
-
Funding NIHR BRU; Idiap Jordi Gol and partial funding from unrestricted grant by BIOIBERICA SA.
-
Competing interests DP-A has received unrestricted funding from BIOIBERICA SA. All other authors have no conflicts of interest to declare in relation with this work.
-
Ethics approval Idiap Jordi Gol ethics committee.
-
Provenance and peer review Not commissioned; externally peer reviewed.