Article Text

Abstract
Objective To investigate frequencies and reasons for switching, treatment responses and drug survival in patients with ankylosing spondylitis (AS) switching tumour-necrosis-factor-α inhibitor (TNFi) treatment in routine clinical care.
Methods AS patients were identified in the Danish nationwide DANBIO registry. Disease activity, treatment responses (50% or 20 mm reduction in Bath AS Disease Activity Index (BASDAI)), duration and rates of drug survival and predictors thereof were studied in patients receiving ≥2 different biological drugs.
Results Of 1436 AS patients starting TNFi treatment, 432 patients (30%) switched to a second and 137 (10%) to a third biological drug. Compared with non-switchers, switchers were more frequently women (33%/22%), had shorter disease duration (3 years/5 years) and higher BASDAI (62(52–76) mm/56(43–69) mm (median(interquartile-range))), Bath AS Functional Index (BASFI) (54(39–71) mm/47(31–65) mm) and visual-analogue-scale (VAS) global, pain and fatigue scores when they started the first TNFi (all p<0.01). Main reason for switching was lack of response (56%). During the first, second and third treatment BAS- and VAS scores had decreased after 6 months' treatment (all p<0.05). Median drug survivals were 3.1, 1.6 and 1.8 years respectively (p<0.001). After 2 years of treatment 52% of switchers and 63% of non-switchers had achieved response (number needed to treat 1.9 and 1.6, respectively, p=0.01). Drug survivals were similar regardless of the reason for switching. Male gender and low BASFI predicted drug survival of the second TNFi.
Conclusions Nearly one-third of AS patients in clinical practice switched biological treatment. Response rates and drug survivals were lower among switchers, however, half of switchers achieved treatment response.
- Ankylosing Spondylitis
- Anti-TNF
- Disease Activity
Statistics from Altmetric.com
Introduction
The beneficial effect of tumour-necrosis-factor-α-inhibitor (TNFi) treatment in ankylosing spondylitis (AS) has been documented in several randomised trials.1–3 However, some patients experience lack of treatment effect (LOE) and some patients terminate treatment due to side effects.
In Denmark, four TNFi are currently marketed for the treatment of AS (infliximab, etanercept, adalimumab and golimumab). The drugs have different chemical structures, routes of administration and pharmacokinetics.4 Thus, if a patient fails to achieve adequate response during the first treatment or experiences adverse events (AE), a switch to a second TNFi seems appealing.
Among patients with rheumatoid arthritis (RA), switching has become daily practice5–10 and approximately 55% of RA switchers achieve ACR20 response.11 However, the rate and success of switching may be different in patients with AS.12 ,13
Currently, experiences from switching in patients with AS mainly originate from one large open label trial14 and several smaller observational studies including few treatment centres or less than 50 switch episodes.8 ,12 ,15–22
The Danish nationwide DANBIO registry now includes up to 10 years of prospective follow up of patients with inflammatory arthritis treated with biologicals in routine care.23 We have previously described treatment response and predictors thereof in AS patients receiving the first TNFi treatment.24 The aims of the present study were to investigate frequencies and reasons for switching, treatment responses, drug survivals and predictors thereof among patients switching TNFi treatment.
Patients and methods
The Danish DANBIO-registry is a nationwide registry that was commenced in year 2000 and approved as a clinical quality registry in 2006. DANBIO covers >90% of adults treated with biologics due to rheumatic disease in routine care.25–27 According to Danish legislation, any registration and publication of data from clinical registries does not require patient consent or approval by Ethics Committees.
Biological treatment courses initiated before 1 January 2011 were included in the present study and follow-up was until 20 April 2011. By 1 January 2011, 2039 patients with a diagnosis of AS according to specialists in rheumatology had been registered. It is not explicitly stated in DANBIO how individual patients fulfill the diagnostic criteria for AS. Patients with psoriatic arthritis were excluded from this analysis. We excluded 518 AS patients only treated with disease-modifying anti-rheumatic drugs (DMARDs), 84 patients treated with biologicals as part of clinical trials, and one patient who did not receive TNFi as the first biological. Thus, 1436 biologically naïve patients, who had been registered in DANBIO from the time of initiation of the first TNFi were included. Of these, a subgroup of 432 patients (switchers) had received treatment with ≥two different biological drugs (TNFi or other) during follow-up (table 1). The total number of treatment courses was 2061.
Baseline demographics and disease activity when patients started the first tumour necrosis factor inhibitor
Axial disease activity was assessed by Bath AS Disease Activity Index (BASDAI), Bath AS Function Index (BASFI), Bath AS Metrology Index (BASMI) and thorax excursion range (introduced in year 2003). C reactive protein (CRP) level (normal range ≤10 mg/l), visual analogue scales (VAS) for pain, global and fatigue scores were also registered. Since year 2010 the AS Disease Activity Score (ASDAS) was registered. Data collection occurred at minimum biannually.
Queries were sent to the hospitals regarding treatment series with incomplete follow-up. All calculations were based on observed data and no imputation of missing data was performed. All observations were censored at 20 April 2011.
Drug adherences
Drug survival was calculated as the number of days individual patients maintained treatment with the drug. Start date was the date of the first given dose and stop date was the date of the first missed dose. Temporary treatment interruptions (eg, due to infections or surgery) of <3 months' duration were allowed. If a patient restarted treatment with the same biological drug after >3 months treatment interruption, the second treatment course with the drug was deleted from the dataset (62 cases).
The reasons for drug discontinuation are registered in pre-specified categories: LOE, AE, pregnancy, surgery, infections, loss to follow up and other. In the following, switching-AE denotes switching due to side effects, infection, death or cancer. Switching-LOE denotes switching due to lack/loss of effect. Switching-other denotes switching due to any other cause (pregnancy, surgery, lost to follow up, disease remission) or several reasons for drug discontinuation.
Treatment response
Disease activity was evaluated by the CRP, VAS pain, fatigue and global, BASDAI, BASFI and BASMI-scores 0, 3 and 6 months after initiation of therapy.
Treatment response during each treatment course was evaluated as a reduction in BASDAI of at least 50% or >20 mm (BASDAI 50%/20 mm response).1 ,28 We classified patients as ‘responders’ if they achieved a sustained BASDAI 50%/20 mm response (yes/no) at both the 3 and 6-months’ visits compared with the BASDAI registration at 0 months. Thus only patients treated >3 months were included in this analysis. The individual components of the BASDAI score were not registered in DANBIO until year 2008, and therefore Assessment of SpondyloArthritis international Society (ASAS) response is not reported.
The overall long-term treatment response was evaluated at the 2-year visit (defined as the first visit >104 weeks after initiating the first TNFi). This time point was chosen arbitrarily to allow for an acceptable number of switch episodes without excluding too many patients with insufficient follow-up time. The BASDAI 50%/20 mm response at the 2-year visit was compared with the baseline BASDAI at the first treatment course, irrespective of switch episodes in the meantime. Thus, only patients with a registration of BASDAI at baseline and follow-up for ≥2 years were included in this analysis (609 patients). Also, the proportion of patients with BASDAI <40 mm at the 2-year visit was evaluated.
In the subgroup of patients with available ASDAS,29 ,30 disease activity was reported as the median ASDAS and the proportion of patients attaining ASDAS <2.1 (inactive/moderate disease activity) at the latest visit registered after ≥2 years follow-up.
Statistics
Statistical analyses were performed by SPSS (V.16.0, SPSS Inc., Chicago, Illinois, USA) and SAS software (V.9.0, SAS Institute Inc, Cary, North Carolina, USA). Demographic and descriptive data are presented by medians/IQR. Groups were compared by non-parametric testing (unpaired data: χ2 and Mann-Whitney tests, paired: Wilcoxon signed ranks test). The proportion of patients achieving treatment responses were expressed as Number-Needed-to-Treat (NNT) calculated as the reciprocal value of response rates. In all statistical tests, a p value <0.05 was considered statistically significant.
Kaplan Meyer plot and log rank test were used to visualise drug survival. Unadjusted/univariate and multvariate Cox regression analysis with HR were used for the identification of factors associated with drug survival of the second treatment course. Logistic regression analyses and OR were used to identify factors associated with BASDAI 50%/20 mm response. In the regression analyses, patient age, baseline CRP, BASDAI, BASFI, BASMI and VAS scores were included as continuous variables whereas gender, type of TNFi (current and previous treatment), use of methotrexate (yes/no) and reason for discontinuation of the first TNFi (AE/LOE/other) were included as categorical variables. The variables with the highest p value were excluded stepwise (backward selection) leaving only statistically significant variables in the final model.
In the following, unless otherwise stated, the term baseline is used to describe disease activity upon starting the individual treatment course.
Results
Baseline characteristics and patient disposition
Among the included 1436 patients, 360 (25%) were women and median age was 41 years (IQR 33–50 years). Median follow-up time was 2.4 years (IQR 1.0–4.8 years). The patient flow is outlined in figure 1. When data were censored, 432 patients (32%) had switched treatment and 773 patients were still treated with the original TNFi. Switchers were more frequently women, had shorter disease duration, were more frequently treated with methotrexate and had higher VAS scores, BASFI and BASDAI compared with non-switchers when they started the first TNFi (table 1). More non-switchers who continued treatment vs non-switchers who stopped treatment without starting a new TNFi, were men (80 vs 71%, p=0.002), but baseline disease activities were similar in the groups (all p>0.05, data not shown).
The most prevalently used first line drug was infliximab in year 2001–2008 and adalimumab in year 2009–2010. Adalimumab was the most frequently used second (46%) and third line (31%) treatment (table 2). Biologicals other than TNFi were only initiated in 19 of 2061 treatment series and will not be discussed further. The most frequent combinations of first and second TNFi were: infliximab-adalimumab (161 patients), infliximab-etanercept (88 patients), adalimumab-etanercept (84 patients), etanercept-adalimumab (36 patients).
Number of treatment courses according to biological drug

Flow -chart of treatment course 1,2 and 3 and reasons for drug discontinuation (n= 1,436). Numbers show the number of patients LOE: Lack of effects, AE: adverse events
Baseline infliximab doses among patients starting infliximab as the first, second and third treatment were 296 mg (3.9 mg/kg), 364 mg (4.6 mg/kg) and 366 mg (5.0 mg/kg), respectively. Similarly, the average doses at the latest registered visit were 324 mg (4.2 mg/kg), 382 mg (4.9 mg/kg) and 390 mg (5.4 mg/kg), respectively. At the latest visit, 21% of patients received infliximab every 6 weeks, 11% every 7 weeks and 56% every 8 weeks. Baseline use of methotrexate was more frequent among infliximab users and patients with peripheral joint disease (both p<0.01, data not shown).
A total of 231 patients stopped the first TNFi without starting a new. The main reason for switching was LOE (240 patients, 56% of switchers) or AE (118 patients, 27%). Among the 432 patients who started treatment with a second biological, 137 switched to a third (32%), 217 patients continued treatment, and 78 patients stopped without starting a new. The main reason for switching to a third biological was LOE (86 patients, 63% of switchers) (figure 1). Similarly, 39/137 patients (28%) switched to a fourth biological, and 12/39 patients (31%) switched to a fifth. Among the 432 switchers, baseline disease activity was similar irrespective of the reason for switching (see supplementary table S1).
Drug survival
Drug survival decreased after switching (p<0.001) (figure 2). Median drug survival of the first TNFi among switchers was 0.7 years (95% CI 0.6 to 0.8 years).
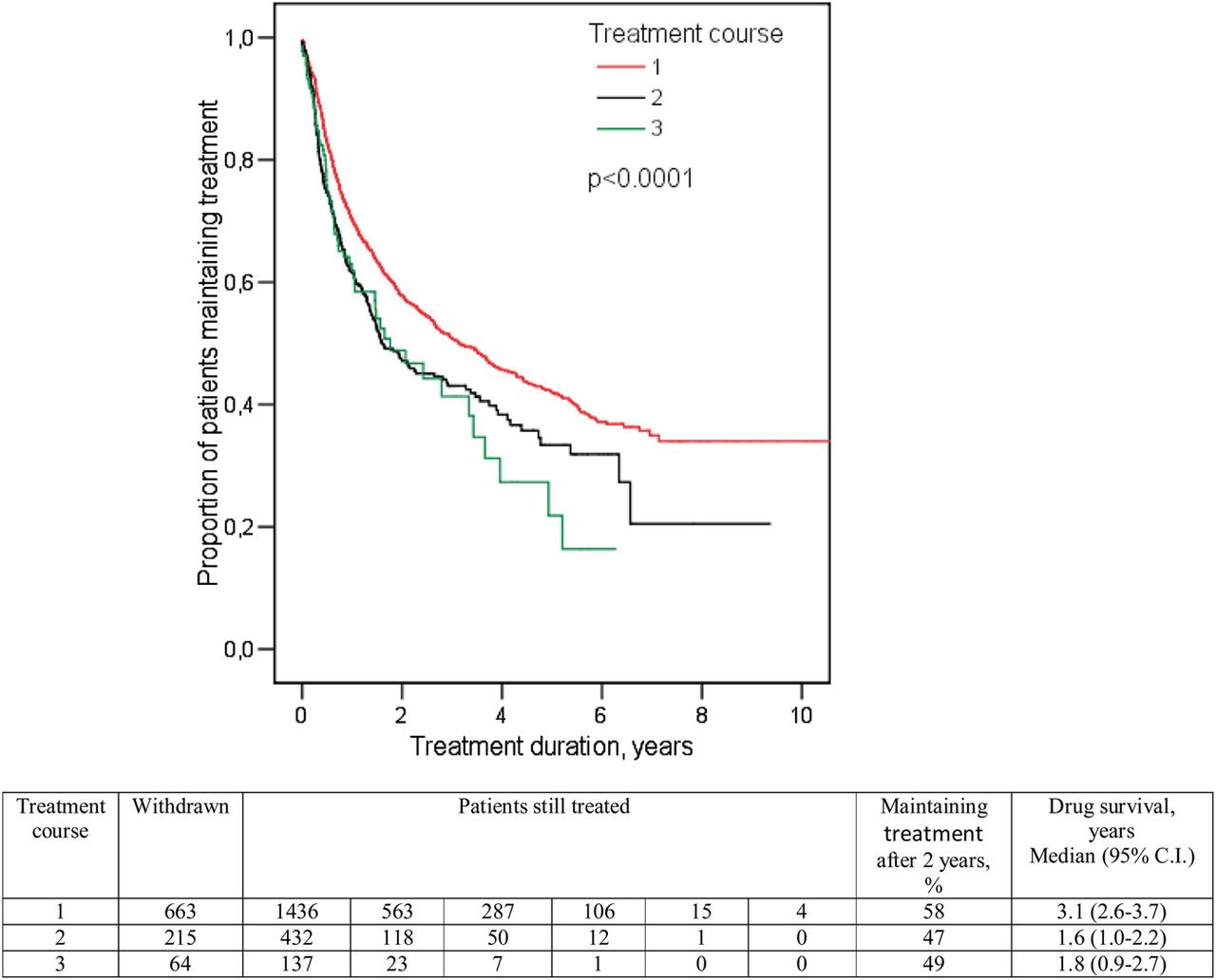
Drug adherences by treatment course. Kaplan Meyer drug survival curves. The table below show the number of patients still treated at the corresponding time points, the proportion of patients maintaining treatment after 2 years and the median drug survival. This figure is only reproduced in colour in the online version.
Treatment response
Most scores decreased after 3 and 6 months' treatment during the first, second and third treatment course (table 3). For switchers, baseline CRP was significantly lower at the second and third treatment course compared with the first (p<0.05) (figure 3). Baseline BASDAI and VAS global were significantly lower at the second treatment course compared with the first (p<0.001). For switchers, the delta values for the decrease in CRP, BASDAI and VAS global between baseline and 6 months were similar at the second and third treatment course compared with the first (all p>0.05) (figure 3).

{kind=link}
{kind=link}
{kind=link}
Disease activity for switchers at baseline, 3 months and 6 months during biological treatment course 1 (red). course 2 (grey) and course 3 (green) (n=432). Columns show medians. Panel A: C reactive protein (CRP), panel B: Bath AS Activity Index (BASDAI), panel C: Visual analogue scale (VAS) global. This figure is only reproduced in colour in the online version.
CRP level, VAS and BAS scores during the first (n=1436), second (n=432) and third treatment course (n=137)
During the first treatment course, the proportion of patients achieving BASDAI 50%/20 mm response within 6 months was 54% (NNT=1.9). Corresponding rates during the second and third treatment course were 37% (NNT=2.7) and 30% (NNT=3.4).
At the 2-year visit, 52% of switchers (NNT=1.9) and 63% of non-switchers (NNT=1.6) (p=0.01) had a BASDAI 50%/20 mm response (compared with the baseline visit of the first TNFi) and 54% of switchers (NNT=1.9) and 79% (NNT=1.3) of non-switchers (p<0.0001) had a BASDAI <40 mm. Switchers had received a median of two biological drugs (IQR 2–2).
Among patients treated ≥2 years, 316 patients had an available ASDAS-score at their latest visit. The proportion of patients with ASDAS<2.1 was 37% among switchers and 71% of non-switchers (p<0.001). Median ASDAS among switchers and non-switchers were 2.5 (IQR 1.8–3.5) and 1.6 (1.0–2.3), respectively.
Predictors of drug survival and response during the second treatment course
In univariate Cox regression, drug survival of the second biological was longer in men (p=0.03), patients treated with adalimumab (p=0.03), patients previously treated with infliximab (p=0.004) and patients with lower BASFI (p=0.03). Baseline CRP, BASDAI, BASMI and VAS-scores, age, use of methotrexate and reason for withdrawal of the first TNFi were not statistically significant. In multvariate Cox regression, predictors of longer drug survival were male gender (HR 1.76 (95% CI 1.2 to 2.5), p=0.002) and low baseline BASFI (HR1.07/cm (1.0–1.15), p=0.046), whereas type of TNFi (current or previous), reason for withdrawal of first TNFi, use of methotrexate, age, CRP, BASMI, BASDAI and VAS scores at the start of the second treatment were not predictive.
Predictors of BASDAI 50%/20 mm response during the second treatment course were higher CRP at baseline (OR 1.03/mg/l (95% CI 1.0 to 1.05), p=0.02), lower VAS fatigue (0.6/cm (0.5–0.9), p=0.008), and lower BASFI (0.6/cm(0.2–0.8), p=0.001) (multiple logistic regression analysis corrected for baseline BASDAI). Type of TNFi (current or previous), reason for withdrawal of first TNFi, gender, age, BASMI, VAS global, VAS pain and age were not significant.
Discussion
In this study of 1432 patients with AS we found that almost one third switched TNFi during up to 10 years of follow-up. Switchers were more frequently women and patients with high baseline subjective disease activity. The main reason for switching was LOE. The disease activity decreased significantly during the second and third treatment course. Although switchers had poorer treatment response and shorter drug survival than non-switchers, approximately half of switchers achieved clinical response. Two years after switching, half of switchers maintained treatment with the second biological.
Lack of efficacy explained half of the switch episodes, followed by AE in one out of four. Switches were almost exclusively between TNFi. Previous observational studies have included a limited number of switch-episodes. Lie et al found switching in 77/514 (15%) AS patients during 9 years of follow-up mainly due to AE.22 A French study described switching in 99/377 (26%) patients with spondyloarthropaties during 8 years of follow-up, the main reason was LOE.20 These differences are unexplained but possibly reflect regional differences in prescription practice.
We found that switchers were more often women and had higher subjective disease activity compared with non-switchers when starting the first TNFi, CRP and BASMI were similar. The Norwegian study found no such differences,22 however, the study may have been underpowered as baseline data only was available in 39% of switchers. Studies performed in RA patients report a similar tendency towards higher baseline disease activity among switchers.5 ,9 This might reflect that switchers are patients refractory to treatment for example, due to chronic disability or comorbidities.31
In the present study, response rates were markedly reduced among switchers. Similar results were found by Lie et al22 Rudwaleit et al reported response among 41% of 326 adalimumab treated patients with AS who previously failed treatment with infliximab and/or etanercept compared with 63% among TNFi-naïve patients (p<0.001).14 Furthermore, we found decreased drug survival after switching. Similar tendencies have previously been demonstrated.9 ,13 ,14 ,22
Although the response rates and drug survivals decreased after switching, the 6 months' response rate was 37% during the second treatment course. After 2 years' of treatment, 52% of switchers had achieved BASDAI50/20 mm response and 54% a BASDAI <40 mm. Rudwaleit et al and Lie et al reported BASDAI50 response among 41%14 and 28% of switchers.22 Observational studies including <25 patients report 43–83% response rates.8 ,15–18 A retrospective study among 56 switchers found a 80% response rate after 3 months' treatment.20 It should be noted that several clinical studies measure response rates as 50% reductions in BASDAI,14 ,17 ,22 which is a more conservative measure than the BASDAI50%/20 mm response used in the current study. However, in spite of great variation in study design and methodology, previous studies overall describe high response rates among AS patients switching therapy.
Increased CRP and low BASFI were associated with treatment response during the second treatment course. A similar pattern has previously been described among AS patients receiving their first TNFi.24 ,31–36 However, one previous study among 99 patients with spondyloarthropaties switching TNFi found no predictors,20 perhaps due to lack of power. Perhaps increased levels of CRP identify patients with higher cytokine mediated inflammation and therefore better response to TNFi. On the contrary, higher BASFI might be associated with chronic disability or psychological factors irresponsive to treatment.31
Currently, inflammatory markers and functional status are not included in the guidelines for prescribing TNFi in AS. However, possible predictors must be interpreted with caution in clinical settings: we found increased CRP to predict clinical response after switching and 50% of patients with CRP>10 mg/l achieved a BASDAI 50%/20 mm within 6 months. However, 30% of patients with normal CRP also achieved response. More complicated models are needed in order to predict clinical outcome of therapy in individual patients.32
We found longer treatment duration of the second biological drug in men compared with women. This is in accordance with previous studies, not only in AS but also RA and psoriatic arthritis.24 ,36–41 Why clinical response differs according to gender is still unclear.
The main switch patterns were from infliximab to adalimumab or etanercept. This reflects that infliximab was the first TNFi marketed to treat AS. Among patients starting treatment in year 2008 and thereafter, the most prevalent switch was from adalimumab to etanercept (48/157 switches). Drug survival during the second treatment course was longer among adalimumab treated patients and among patients previously treated with infliximab. However, we found no difference in efficacy among the different TNFi. Due to the non-randomised study design, these results must be interpreted with caution. Comorbidity, route of drug administration (subcutaneous/intravenously) and altered clinical practice due to marketing of new drugs might have affected the results.13 ,38
The treatment response of the second biological drug was similar among switchers due to LOE and AE. Some have reported similar results17 ,20 ,22—others describe better treatment effects among AE-switchers.8 ,12 ,14 Our study was limited by the fact that it was not possible to distinguish between treatment termination due to lack of or loss of treatment effect. According to some studies, patients who stop treatment due to secondary loss of treatment effect especially benefit from switching.12 ,14 Smoking status, comorbid disease, concomitant use of NSAIDs, enthesitis and HLAB27 status are factors that might influence treatment outcome.32 However these data are not routinely registered in DANBIO.
In conclusion, nearly one-third of AS patients switched TNFi in routine care during up to 10 years of follow-up, mainly due to inefficacy. The response rates and drug adherences decreased after switching. However, half of the switchers achieved clinical response. Thus, irrespective of the reason for discontinuation of the first TNFi, switching to another TNFi should be considered.
Acknowledgments
Thanks to the departments of rheumatology in Aalborg, Aarhus, Esbjerg, Fredericia, Frederiksberg, Gentofte, Glostrup, Gråsten, Hjørring, Holbæk, Holstebro, Horsens, Helsingør, Kolding, Køge, Næstved/Nykøbing Falster, Odense, Randers, Rigshospitalet, Roskilde, Silkeborg, Slagelse, Svendborg, Vejle, Viborg, Denmark for reporting to the DANBIO registry.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online table
Footnotes
-
Contributors All coauthors fulfilled criteria for co-authorship according to the Vancouver Protocol.
-
Competing interests MØ: Abbott, Centocor, GSK, MSD, Mundipharma, Novo, Pfizer, Roche, UCB, Wyeth (less than 10.000 USD each); AGL: MSD, UCB, Abbott (less than 10.000 USD each); AS: MSD, Pfizer, Roche (less than 10.000 USD each); HML: Roche, MSD (less than 10.000 USD each); CR: Pfizer, Abbott (less than 10.000 USD each); MLH: Abbott, Centocor, Roche, Pfizer (less than 10.000 USD each); BG, NSK, UT, NM, AH, VF, HN, LE, DVJ and PMP declare no conflict of interest.
-
Ethics approval The study reports data from a National Registry. Thus, approval from the regional ethics committee is not required. This is also stated in the methods’ section of the paper.
-
Provenance and peer review Not commissioned; externally peer reviewed.
-
Correction notice This article has been corrected since it was published online first. Figure 2 has been altered.