Article Text

Abstract
Objective Excess mortality in rheumatoid arthritis (RA) is expected to have improved over time, due to improved treatment. Our objective was to evaluate secular 5-year mortality trends in RA relative to general population controls in incident RA cohorts diagnosed in 1996–2000 vs 2001–2006.
Methods We conducted a population-based cohort study, using administrative health data, of all incident RA cases in British Columbia who first met RA criteria between January 1996 and December 2006, with general population controls matched 1:1 on gender, birth and index years. Cohorts were divided into earlier (RA onset 1996–2000) and later (2001–2006) cohorts. Physician visits and vital statistics data were obtained until December 2010. Follow-up was censored at 5 years to ensure equal follow-up in both cohorts. Mortality rates, mortality rate ratios and HRs for mortality (RA vs controls) using proportional hazard models adjusting for age, were calculated. Differences in mortality in RA versus controls between earlier and later incident cohorts were tested via interaction between RA status (case/control) and cohort (earlier/later).
Results 24 914 RA cases and controls experienced 2747 and 2332 deaths, respectively. Mortality risk in RA versus controls differed across incident cohorts for all-cause, cardiovascular diseases (CVD) and cancer mortality (interactions p<0.01). A significant increase in mortality in RA versus controls was observed in earlier, but not later, cohorts (all-cause mortality adjusted HR (95% CI): 1.40 (1.30 to 1.51) and 0.97 (0.89 to 1.05), respectively).
Conclusions In our population-based incident RA cohort, mortality compared with the general population improved over time. Increased mortality in the first 5 years was observed in people with RA onset before, but not after, 2000.
- Rheumatoid Arthritis
- Epidemiology
- Outcomes research
Statistics from Altmetric.com
Introduction
Since the 1950s, studies have drawn attention to the premature mortality in rheumatoid arthritis (RA) compared with the general population.1–7 Cardiovascular diseases (CVD) are the leading cause of excess mortality; infections and malignancies are other causes.8–15 Mortality risk is generally lower in incident than prevalent cohorts,2 ,4 ,5 ,8 as reflected by a lower standardized mortality ratio (SMR) (1.2 vs 1.9, respectively).16 Studies evaluating mortality in the early years of RA report mixed results.7 Some cohorts from early arthritis clinics, with early/aggressive disease-modifying antirheumatic drug (DMARD) treatment, report no excess mortality,17–19 while others report increased mortality apparent from early years of disease and increasing with RA duration.20–22 Others report excess mortality becoming apparent after 7–10 years.23
Increased mortality in RA is believed to be a consequence of inflammation, as markers of inflammation and disease severity have been associated with increased risk of death.24–31 With more effective treatments and a paradigm shift in treating RA aimed at achieving remission, mortality would be expected to have improved over time.32–37 Previous studies evaluating secular trends in RA mortality, including a meta-analysis,4 have generally found no improvement relative to the general population, with some studies suggesting a widening mortality gap, due to improved mortality in the general population but not, or to a lesser extent, in RA.4 ,16 ,23 ,38–43 However, these studies evaluated cohorts with RA onset up to the 1990s. In contrast, our study evaluates temporal trends in more contemporary incident cohorts with RA onset before versus after 2000, a period when RA treatment changed drastically32 ,44–47 and awareness of cardiovascular risk in RA, and its link to inflammation, increased.24 ,28 ,29 ,48–53
The objective of our study was to evaluate secular trends in RA mortality, by assessing whether the mortality risk over the first 5 years of RA, compared with general population controls, differed between incident RA cases diagnosed in 1996–2000 and in 2001–2006.
Methods
Study design
We conducted a longitudinal study of a population-based incident RA cohort with matched controls from the general population, using administrative health data from the entire province of British Columbia (BC), Canada.
Cohort definition
Incident RA cohort
All incident RA cases in BC who first met criteria for RA between January 1996 and March 2006 (using data from January 1990 onwards) were identified, using physician billing data from the Ministry of Health in a universal healthcare system, and were followed until December 2010. Using previously published criteria,54 individuals were identified as RA cases if they had at least two physician visits at least 2 months apart within a 5-year period with an International Classification of Diseases, Ninth Revision (ICD9) code for RA (714.X).55 To improve specificity, individuals were excluded if they had at least two subsequent visits with ICD9 codes for other forms of inflammatory arthritis (systemic lupus erythematosus, other connective tissue diseases, psoriatic arthritis, ankylosing spondylitis and other spondyloarthropathies). Cases were also excluded if a diagnosis of RA by a non-rheumatologist was never confirmed when the individual saw a rheumatologist; or if they had no subsequent RA diagnosis over more than 5 years of follow-up. These criteria have been validated in a subsample who participated in an RA survey. Using opinion of an independent rheumatologist reviewing medical records from their treating physicians as gold standard, we estimated the positive predictive value at 0.82.56
General population controls with no diagnoses of inflammatory arthritis were selected, using the same administrative databases as for the RA cohort, matching controls to RA cases in a 1:1 ratio on gender, birth year and index year.
The sample was divided into two cohorts: an earlier and later cohort (cases with RA onset in 1996–2000 vs 2001–2006, respectively, and their controls).
Data sources
Data were obtained from administrative databases of the Ministry of Health of British Columbia on all provincially funded healthcare services used since January 1990, including all physician visits, with one diagnostic code representing the reason for the visit, from the Medical Service Plan database57 as well as hospital discharge data.58 Vitals statistics data59 were obtained, from January 1996 onwards, on deaths and primary cause of death derived from death certificates. All data were available until December 2010. Several population-based studies have been published using these data.54 ,60–66
Ethics
No personal identifying information was provided. All procedures were compliant with BC's Freedom of Information and Privacy Protection Act. The study received ethics approval from University of British Columbia.
Statistical analyses
Person-years of follow-up were calculated for incident RA cases and controls, from index date to end of follow-up (censored at 5 years to ensure equal follow-up in earlier and later cohorts), last healthcare utilisation or death. Index date was defined, for RA cases, as when they met incident RA inclusion criteria; and, for controls, as the date of a randomly selected healthcare encounter occurring in the same calendar year as the index year of their matched case. Mortality rates from all-cause, CVD, malignancy and infections were calculated for RA cases and controls, along with mortality rate ratios, with 95% CIs, representing the risk of mortality in RA relative to controls. We also used a parametric exponential proportional hazards (PH) model to estimate HRs representing the mortality risk in RA compared with controls, adjusted for age. Analyses adjusted for comorbidities which differed at baseline between RA and controls, and for the Romano modification of the Charlson comorbidity index (with RA excluded from comorbidities)67–69 were also performed. To test if differences in excess risk of mortality (in RA relative to controls) changed over time, we tested the interaction between the indicators of RA (case vs control) and incident cohort (earlier vs later), in the exponential PH model. A statistically significant interaction indicates that the mortality risk in RA relative to the general population differs between the earlier and later cohorts.
Kaplan-Meier (KM) survival curves were estimated, describing survival from index date until death, stratified according to RA status, for all-cause and cause-specific mortality, censoring at 5 years of follow-up, last healthcare utilisation or death from other cause (for cause-specific analyses). Separate analyses were conducted for 1996–2000 and 2001–2006 cohorts. Sensitivity analyses estimated survival curves using all available follow-up time (ie, not censoring at 5 years). Analyses were performed using SAS V.9.4 (SAS Institute, Cary, North Carolina, USA).
Results
The sample included 24 914 individuals with RA and 24 914 general population controls. Using BC population estimates, our cohorts yield age-standardised and sex-standardised incidence rates of 58 per 100 000 for the 1996–2000 cohort and 68 per 100 000 for the 2001–2006 cohort, consistent with reported RA incidence rates.70 ,71 During the first 5 years, 2747 deaths were observed in the RA cohort and 2332 in controls.
Baseline characteristics of the RA cohorts and controls, measured at index date, are described in table 1. RA cases had more comorbidities than controls (higher rates of prior CVD, chronic obstructive pulmonary disease (COPD), hospitalised infections, hospitalisation rate), but no difference in overall comorbidity score (Romano score with RA excluded from comorbidities).67–69 Of note, age at index date was slightly lower in the later than earlier RA cohort, although the difference is not clinically meaningful (mean (SD): 57.49 (12.8) and 58.35 (12.9) years, respectively). Furthermore, our analyses are age adjusted.
Baseline characteristics of RA cases and controls in the earlier (incidence 1996–2000) and later (incidence 2001–2006) cohorts
Mortality rates, and mortality risk in RA relative to general population controls, are shown in table 2. In the entire cohort, mortality rates of 24.43 and 20.72 per 1000 person-years were observed in RA and controls, respectively, yielding an all-cause mortality rate ratio of 1.18 (95% CI 1.12 to 1.25). Greater mortality in RA compared with controls was observed for mortality from CVD and infections.
Mortality risk in RA compared with general population controls
When comparing mortality risk in RA relative to controls, across incident cohorts, we observed important differences between the 1996–2000 and 2001–2006 cohorts. A 39% increase in all-cause mortality was observed in the earlier RA cohort relative to the general population, whereas no increase was observed in the later cohort. Similarly, increased mortality was observed in earlier, but not later, RA cohorts relative to controls for deaths from CVD, cancer and infections. These time-differences in excess mortality were confirmed in age-adjusted exponential models, where significant interactions between RA (vs controls) and incident cohort (earlier vs later) were found for mortality from all-causes (p<0.001), CVD (p<0.001) and cancer (p=0.002), but not from infection (p=0.097).
To confirm our findings, we assessed age at death. Despite being matched on age to general population controls, RA cases in the earlier cohort died, on average, 1.3 years earlier than controls (mean (SD) age at death from all causes: 76.7 (12.9) vs 78.0 (11.0) years in controls), but not in the later cohort (77.3 (12.8) vs 77.8 (11.4) years in controls).
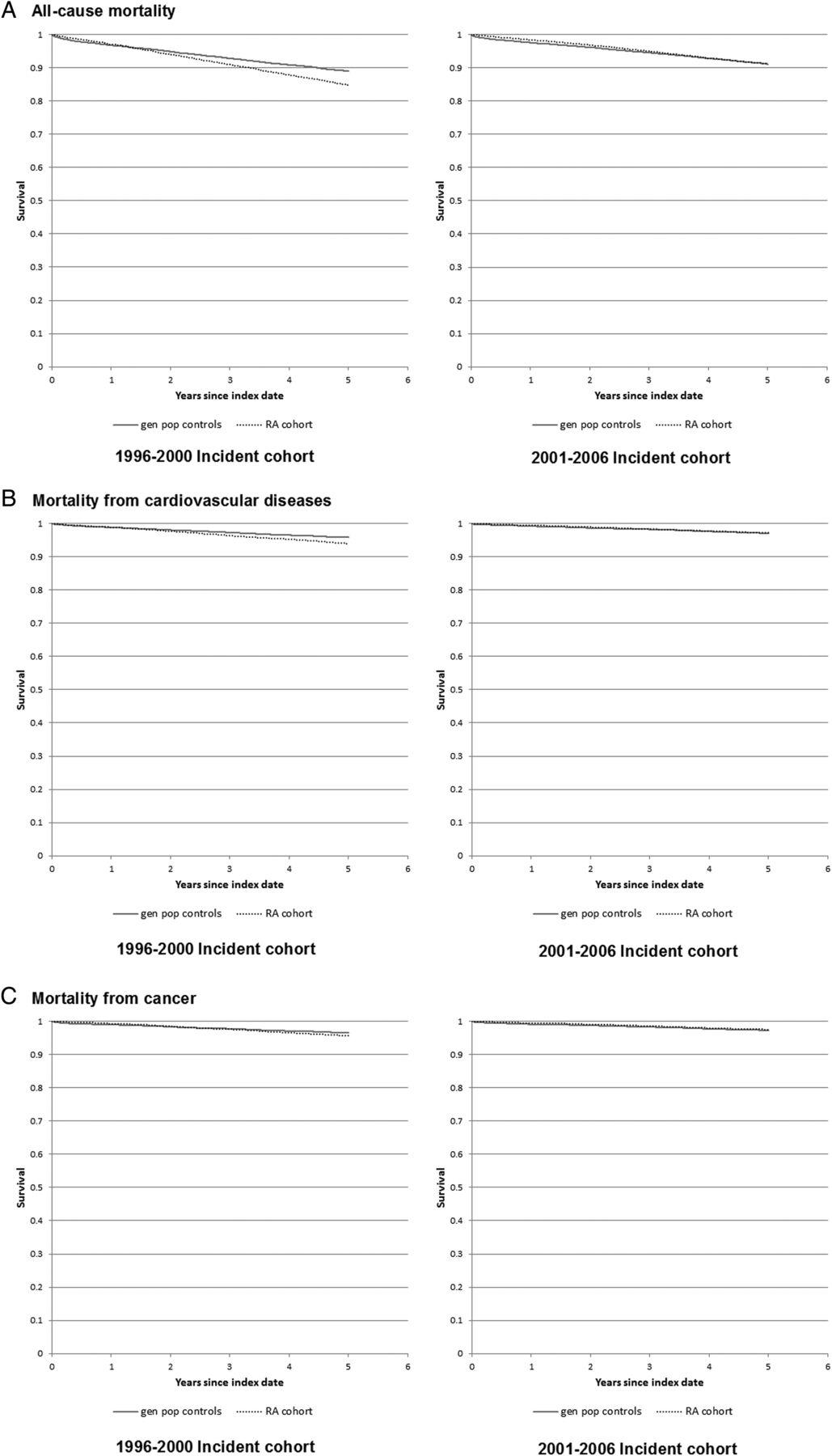
Similarly, KM curves revealed lower survival in RA cases than in general population controls for death from all-causes, CVD and cancer, in the earlier cohort (log rank test p<0.01), but not the later cohort (p=0.695, 0.583, 0.127, respectively) (figure 1). Of note, KM analyses require cautious interpretation as they are unadjusted and based on relatively few cause-specific mortality events. Too few deaths from infections were observed to allow adequate interpretation of results. KM results were similar when survival was uncensored (log rank test p≤0.01 for mortality from all-causes, CVD and cancer in earlier cohort; and p=0.210, 0.510 and 0.473, respectively, for the later cohort with up to 8 years of follow-up) (see online supplementary figure S1).

{kind=link}
Survival from all-causes, cardiovascular diseases, cancer and infection, in rheumatoid arthritis (RA) and general population (gen pop) controls. (A) All-cause mortality; log rank test comparing Kaplan-Meier (KM) survival in RA versus controls for 1996–2000 cohort: p<0.001; and for the 2001–2006 cohort: p=0.695. (B) Mortality from cardiovascular diseases; log rank test comparing KM survival in RA versus controls for 1996–2000 cohort: p<0.001; and for the 2001–2006 cohort: p=0.583. (C) Mortality from cancer; log rank test comparing KM survival in RA versus controls for 1996–2000 cohort: p=0.007; and for the 2001–2006 cohort: p=0.127.
supplementary data
Robustness of our results was tested in sensitivity analyses. Because individuals moving to BC could appear to be incident cases, we excluded all cases/controls with <6 years of Medical Services Plan enrolment at index date. This yielded similar results (table 2). Because the lead-in time to differentiate incident from prevalent RA was longer for the 2001–2006 cohort (11 vs 6 years), we limited the 2001–2006 cohort's lead-in time to 6 years. Results did not differ (all-cause mortality rate ratio: 0.96 (0.89 to 1.04) vs 0.98 (0.91 to 1.07)). To ensure baseline differences in RA duration across the two cohorts did not confound the interaction,72 we adjusted the exponential PH models for RA duration at index date. To avoid near-collinearity between RA/control status and RA duration (which, by definition, equals 0 for all controls), RA duration in RA cases was centred to a mean of 0.73 Results were similar (all-cause mortality adjusted HR 1.48 (1.37 to 1.60) for earlier; 0.92 (0.85 to 1.00) for later cohorts) and the interaction remained significant (p<0.001).
Discussion
We conducted a population-based study of a large incident RA cohort with general population controls, using administrative health data in a universal healthcare system, to evaluate RA mortality trends over time. Our study reveals that the risk of death in RA compared with the general population has improved over time. Statistically significant improvement was observed for all-cause mortality, as well as deaths from CVD, and cancer, but not from infections. In our cohort, over 5 years of follow-up, an increased risk of mortality in RA compared with the general population was observed in people with RA onset on or before 2000, but not in people with RA onset after 2000. Although improvement in mortality risk was clearly observed in our study, one should be cautious about interpreting our results as indicating that mortality differences between RA and the general population no longer exist, as 5 years of follow-up is relatively short, and it is possible that differences between RA and the general population would be observed with longer follow-up, especially since previous studies have suggested that the greatest increase in mortality risk may occur after 7–10 years of disease.23 Of note, in sensitivity analyses, KM survival curves estimated using all available follow-up (up to 8 years for the later cohort) yielded similar results.
Strengths of our study include the population-based nature of our cohort with complete capture of all RA cases in BC, ensuring the sample is representative of the entire spectrum of RA disease and of patients treated in everyday clinical practice; the inclusion of incident cases with complete follow-up from RA onset to death or study end and the large sample size providing adequate power to look at rare events such as mortality.
Limitations of our study are those inherent to observational studies and studies using administrative data. They include uncertainty around RA diagnosis identified using administrative data and possible effect of unmeasured confounding. Measuring the timing of RA onset is imprecise with administrative data. For these to influence the observed difference in mortality risk between the earlier and later cohorts, they would have to differentially affect both cohorts. Temporal differences in billing code practices during the prediagnosis phase could influence timing of the index date. Temporal differences in accuracy of billing data could influence the number of ‘true/false’ RA cases included. However, over the period examined, one would expect improved accuracy as a result, for example, of the introduction of electronic medical records. This would constitute a conservative bias as less non-RA cases would be included in the later cohort. We observed a small increase in RA incidence rate over 1996–2006. A similar trend was reported in Olmsted County, USA over the same period.74 Nonetheless, inclusion of a greater number of non-RA cases in the later cohort could bias results towards a reduced mortality difference with the general population.
Survival could appear improved in the later incident cohort if RA was diagnosed earlier, or if people presented to care earlier, as a result of recent efforts to raise awareness about the importance of early RA diagnosis and treatment. Of note, median RA duration at index date was slightly shorter (3 months) in the 2001–2006 than the 1996–2000 cohort; and mean age at index date was only slightly lower in the later cohort (57.5 vs 58.4 years in the earlier cohort). Furthermore, a younger age at death in RA relative to controls was observed in the earlier, but not the later, cohort. However, caution is warranted when comparing age at death, as a number of factors can influence it.
It is also possible that incident cohorts are contaminated with prevalent cases. Given our minimum lead-in period of 6 years, this would require gaps between consecutive RA visits longer than 6 years. In our cohort, this occurred very infrequently (only 0.44% of periods between consecutive RA visits were >6 years; 94.3% were <1 year; 97.3% <2 years). Because of potential differential effect on the two cohorts (with less prevalent cases in the 2001–2006 cohort due to longer lead-in time), we performed sensitivity analyses limiting the lead-in time of the 2001–2006 cohort to 6 years, which yielded similar results. Furthermore, we explored how much misclassification of prevalent cases as incident cases in the earlier cohort would be necessary to eliminate the difference in excess mortality observed. Analyses (described in online supplementary file) revealed that highly unlikely assumptions were required, indicating that misclassification cannot reasonably account for the observed results. Prevalent RA cases moving to BC during the study period could also be included. However, this would likely not differentially affect the two cohorts, and sensitivity analyses excluding individuals registered <6 years prior to index date yielded similar results.
Two other recent studies, until now published only in abstract form, also support the concept that the mortality risk in RA compared with the general population has recently improved.75 ,76 A population-based study of Olmsted County found a significant reduction in cardiovascular mortality among patients with RA onset in 2000–2007 vs 1990–1999 (HR: 0.43, 95% CI 0.19 to 0.94),75 with no difference with the general population for the 2000–2007 patients. However, their results are based on a small sample (315 patients with RA in 2000–2007 cohort), and only 8 deaths observed in RA and 9 in controls. Our analyses provide more robust confirmation of these findings in an independent, much larger sample, with >2000 deaths in RA and controls. Interestingly, previous studies from the same group described a gradual widening of the mortality gap, relative to the general population, for patients with RA with more recent onset over 1955–2000.38 ,39 This suggests that improvement in mortality may be limited to patients with RA onset after 2000, as observed in our study. The second study used an electronic medical record database in the UK to compare all-cause mortality in two incident RA cohorts (RA onset 1999–2005 followed until end of 2005; and RA onset 2006–2012 followed until end of 2012) compared with general population controls.76 Consistent with our findings, they found a significant reduction in the HR for all-cause mortality, relative to controls, for the later RA cohort (p=0.027 for interaction). However, even in the later cohort, RA mortality remained increased compared with the general population (HR 1.21, 95% CI 1.05 to 1.39).
Our findings have important implications for people living with arthritis, clinicians and health policy makers. It provides reassuring evidence suggesting that time trends in the disease itself and/or its management are having a beneficial impact on an outcome of utmost importance to people living with arthritis. Exploring why mortality has improved over time is beyond the scope of this study. We speculate that it may be due to improved RA treatment, with more effective control of inflammation, from availability of more effective DMARDs and from the paradigm shift in RA management towards early, aggressive treatment with the aim of eradicating inflammation. Alternatively, improved survival could be due to improved prevention, detection or management of life-threatening comorbidities, such as CVD, as a result of increased awareness of its role as a leading cause of premature death. It is also possible that the natural history of RA has evolved over time. Exploration of these reasons warrants further study. Furthermore, future long-term studies should compare mortality in RA versus general population over >10 years of follow-up, since RA onset.
In conclusion, in our population-based incident RA cohort, the 5-year mortality risk compared with the general population has improved for patients with RA onset in the 21st century. Statistically significant relative risk reductions were observed for all-cause mortality, as well as deaths from CVD, and cancer, but not from infections. In our cohort, during the first 5 years after RA diagnosis, the mortality gap between RA and the general population observed in people with RA onset on or before 2000 was not observed for people with RA onset after 2000. Longer follow-up is needed before concluding that mortality differences between RA and the general population no longer exist.
Acknowledgments
We would like to thank the Ministry of Health of British Columbia and Population Data BC for providing access to the administrative data. All inferences, opinions and conclusions drawn in this publication are those of the authors, and do not reflect the opinions or policies of the Data Stewards.
References
Footnotes
Handling editor Tore K Kvien
Contributors All authors contributed to the conception and study design. DL and AA-Z contributed to data acquisition, all authors contributed to data analysis or interpretation; all authors contributed to drafting or reviewing the manuscript and all approved the final draft of the manuscript.
Funding This study was funded by the Canadian Institute for Health Research (#32615), who played no role in the design or conduct of the study, other than providing peer-review of the study proposal.
Competing interests None declared.
Ethics approval University of British Columbia Ethics Board.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement Results from sensitivity analyses not presented in full in the manuscript including in supplementary files are available on request to the corresponding author.