Article Text

Abstract
Objectives Bisphosphonates have some reported beneficial effects in treating osteoarthritis (OA). This study examined the effects of bisphosphonate use on symptoms and structural progression of knee OA in participants from the NIH Osteoarthritis Initiative cohort.
Methods People with typical OA trial entry criteria (KL2/3, minimum joint space width 2.5–5.0 mm and pain ≥4 on a numeric rating scale) were classified as bisphosphonate users (≥3 of the 5 years; n=55) or non-users (no use in the preceding 5 years or during follow-up; n=268). Annual data over 4 years were analysed using linear mixed modelling and generalised estimating equations.
Results Bisphosphonate compliance was 85% at year 1, reducing to 76% by year 4. Numeric rating scale pain scores were significantly reduced among bisphosphonate users at years 2 and 3 (year 3, −0.9 vs −2.2, p=0.004), though not year 4, after adjustment for baseline pain and analgesic use. Differences in Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC) pain and disability scores did not reach statistical significance at any time point. There was a trend to less joint space narrowing in bisphosphonate users over time (year 4, 0.51 vs 0.29 mm; p=0.06).
Conclusions Significant reduction in numeric rating scale pain was observed in the first 3 years with bisphosphonate use; diminution of effects by year 4 may reflect reduced compliance. Differences in results obtained using numeric rating scale and WOMAC may reflect different constructs measured by these tools. The beneficial trend on structural progression should be considered in terms of the sample size.
- Osteoarthritis
- Knee Osteoarthritis
- Outcomes research
Statistics from Altmetric.com
Osteoarthritis (OA) is a growing cause of chronic disability and a major problem for health economies.1–4 Current therapies are symptomatic with limited effect size in terms of pain reduction,5 while development of disease-modifying OA drugs has been challenging.6 Therefore, there is a major need to develop new, effective therapies.
Recent work has highlighted some beneficial effects of agents with potential for both cartilage and bone-modifying effects in OA of the knee7–9 and spine.10 The subchondral bone is known to be an important factor in OA pain and structural progression. Bone marrow lesions (BML) seen on MRI have been associated with knee pain and ipsilateral progressive cartilage loss.11–13 Bone area and elevated bone mineral density (BMD) in the subchondral bone have been shown to predict cartilage defect development14 ,15 and bone area to predict cartilage volume loss.15
Of these potential therapies, bisphosphonate use has been explored in a number of OA studies with apparent mixed results.16 Effects on bone have generally been positive, with one cross sectional study showing reduction in odds of having a bone marrow abnormality of nearly 90% with the use of alendronate (OR 0.11, p≤0.05).17 Other work demonstrated that risedronate 50 mg weekly prevented an increase in BML size,18 although this did not reach statistical significance. Zoledronic acid has been reported effective in reducing knee pain and the size of BMLs.7 However, although risedronate (15 mg) reduced markers of cartilage degradation and bone resorption, it did not achieve Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC) symptom reduction or slowing of radiological progression of joint space narrowing (JSN) over 2 years.19 ,20
The NIH Osteoarthritis Initiative (OAI) provides a large, comprehensive dataset which permits exploration of the effects of bisphosphonates over a number of years. We aimed to examine the effect of bisphosphonate use on OA symptom and structural outcomes in people selected from the OAI cohort for typical OA trial inclusion criteria and followed for 4 years.
Patients and methods
Study design, setting and participants
Data used in the preparation of this article were obtained from the OAI cohort, a publicly available multicentre population-based observational cohort study of knee OA (available for public access at http://www.oai.ucsf.edu/). Specific datasets used are detailed in online supplementary table S1. The OAI comprises data on persons aged 45–79 years within three subcohorts, the Progression group (persons with existing knee OA; n=1390), the Incidence group (persons with risk factors for knee OA; n=3284) and the non-exposed Control group (n=122).21 Both knees of 4796 participants were studied annually using 3T MRI (not used in these analyses) and fixed flexion radiography22 ,23at baseline, 1, 2, 3 and 4 years follow-up.
Persons were excluded from the OAI if they had inflammatory arthritis, severe JSN in both knees, unilateral knee joint replacement and severe JSN in the contralateral knee, inability to undergo MRI, or to provide a blood sample, required use of walking aids excepting a single straight cane ≤50% of the time, or were unwilling to provide informed consent. Patients were recruited at four clinical sites, and the study was approved by the institutional review boards at each of the sites. All participants gave informed consent. Radiological endpoints are now available for 4 years of observation (79% of population retained) and clinical data for 5 years.
Participants: inclusion and exclusion criteria for these analyses
For these analyses, we were interested in a group who were in the early stages of clinical OA and who were at increased risk of developing incident OA or of worsening OA over time. Therefore, persons with knee replacements at baseline (n=64) and those in the non-exposed control group (n=122) were excluded from the analysis. To further simulate a population similar to patients commonly included in clinical trials of knee OA, we included participants whose knees were scored as having JSN of Grade 2 or 3 on the Kellgren and Lawrence grading system,24 medial joint space width (JSW) of 2.5–5 mm, an osteophyte (medial osteophyte grade 1 and above) using the Altman atlas,25 and had pain of 4–10 on a numeric rating scale. Only one knee was used for each participant. When both knees met the above criteria for an individual patient, the knee with the most severe features of OA was selected by serially choosing the knee with the worst (highest) Kellgren-Lawrence (KL) grade, the worst osteophyte(s) (higher grade), the highest pain and the lowest JSW.
Bisphosphonate use
Bisphosphonate use was calculated by classifying self-reported use of any bisphosphonate to treat osteoporosis or Paget's disease in the last year, then summarising number of years used. Patients were classified as long-term bisphosphonate users if they self-reported bisphosphonate use in the past year on 3–5 occasions between baseline and 4 years of observation. Misclassification due to missing data was minimised by classifying patients as users on a particular occasion if they had missing data for that occasion, but reported bisphosphonate use in the last year at both the preceding and subsequent years. Non-users of bisphosphonates were defined as persons who reported not using bisphosphonates in the preceding five years at baseline, and did not report use of bisphosphonates in the past year for years 0–5.
Participants were also asked if they had been told by a doctor that they had sustained a bone fracture since age 45.
Inclusion criteria
Participants were included in these analyses if they had all of the following: KL grade 2 or 3, a definite osteophyte, medial JSW 2.5–5 mm, and a knee pain score of 4 or more on the numeric rating scale. Additionally, they had to either report no use or high use of bisphosphonates over our time period (3–5 years). We limited our analysis to women as the prevalence of bisphosphonate use in men was low.
Knee pain severity scale
Global knee pain severity during the past 7 days was assessed using an 11-point (0–10) numeric rating scale.
WOMAC questionnaire
The pain, function and stiffness scales of the WOMAC V.LK 3.1 (5-point Likert scale) were used to assess knee pain and function for right and left knees separately over the preceding 7 days.
Knee radiographs
Knee radiographs of both knees were taken annually, using fixed flexion radiographs, filmed in the standing position in posterior–anterior projection with knees flexed to 20–30° and feet internally rotated 10°, with a plexiglass positioning frame (SynaFlexer) used to standardise positioning.21 Trained readers at each clinical centre assessed JSW using the knee radiographs using a classification based on the OARSI atlas grades.25
Measurement of minimal JSW measures was facilitated by the use of automated software that delineated the femoral and tibial margins of the joint.26 Measurement of minimum JSW was made by the software at the location of the smallest distance between the femur and tibia margins in the medial compartment.27
Radiological and radioclinical progression
Participants were considered radiological progressors if minimal JSW reduced by 0.5 mm or greater28 and radioclinical progressors if JSW reduced by 0.5 mm or greater and 20% or less improvement in WOMAC pain scores.8
Joint replacements
Data on joint replacements were collected at each follow-up visit.
Statistical methods
Primary hypotheses were tested using all available data on participants who met the entry criteria at baseline. Statistical significance was determined using a p value ≤0.05 (two–tailed) and using Stata V.12.0. Student t tests, χ2 tests and Fisher's exact tests were used to compare differences in means and proportions between bisphosphonate users and non-users.
Linear mixed effect modelling was used to assess the effect of bisphosphonate use on continuous outcomes (pain numeric rating scale scores, WOMAC scores and medial JSW).
Quadratic and cubic transformations of the time variable were added to each model to allow for non-linear changes and were retained if statistically significant. We also incorporated a random effect of patient identification number to account for the dependence in repeated observations on the same person over time and a random slope for the effect of time, enabling differences in trajectory to be modelled, and adjusting for heteroskedasticity in outcomes over time where applicable (JSW).
Binary outcomes (radiological and radioclinical progression) were assessed using generalised estimating equations for the binomial family and using a log link.
Adding study recruitment site as a random effect made no difference to outcomes and so site was not included as a random effect in these analyses.
Group, time and the interaction between group and time were entered as predictor variables, and age and body mass index (BMI) were included as covariates. Data on pain outcomes were additionally adjusted for baseline pain and use of analgesia. Yearly estimates were calculated from the model using the linear combination of estimators function (lincom).
The number of patients available for this analysis was limited to those who had been recruited to the OAI. Having determined that 323 patients satisfied our inclusion criteria and a reasonable proportion (17%) had taken bisphosphonates for 3, 4 or 5 years during follow-up, we calculated that we had 92% power to detect a clinically meaningful difference in pain numeric rating scale and 80% power to detect a difference in the WOMAC pain subscale.
Results
Participants
Bisphosphonate users were older, shorter, thinner, less physically active and more likely to be white than non-users. Prevalent fractures were common in both groups but more common in bisphosphonate users (table 1).
Demographic profile of study patients, by use of bisphosphonates
Bisphosphonate use
Within our highly compliant bisphosphonate users, compliance peaked early in the observation period (years 1–3) and diminished by year 4 (table 2). Overall, 49% used bisphosphonates for all 5 years, with 21.4% using for 3 and 21.4% for 4 years. The most commonly used bisphosphonate in years 1–4 was alendronate (table 3). Most participants classified as bisphosphonate users over years 1–4 were already using bisphosphonates at baseline (78%).
Bisphosphonate use in patients reporting bisphosphonate use on 3–5 occasions over 5 years, by year
Bisphosphonate medication used in past 5 years
Study outcomes
Numeric rating scale
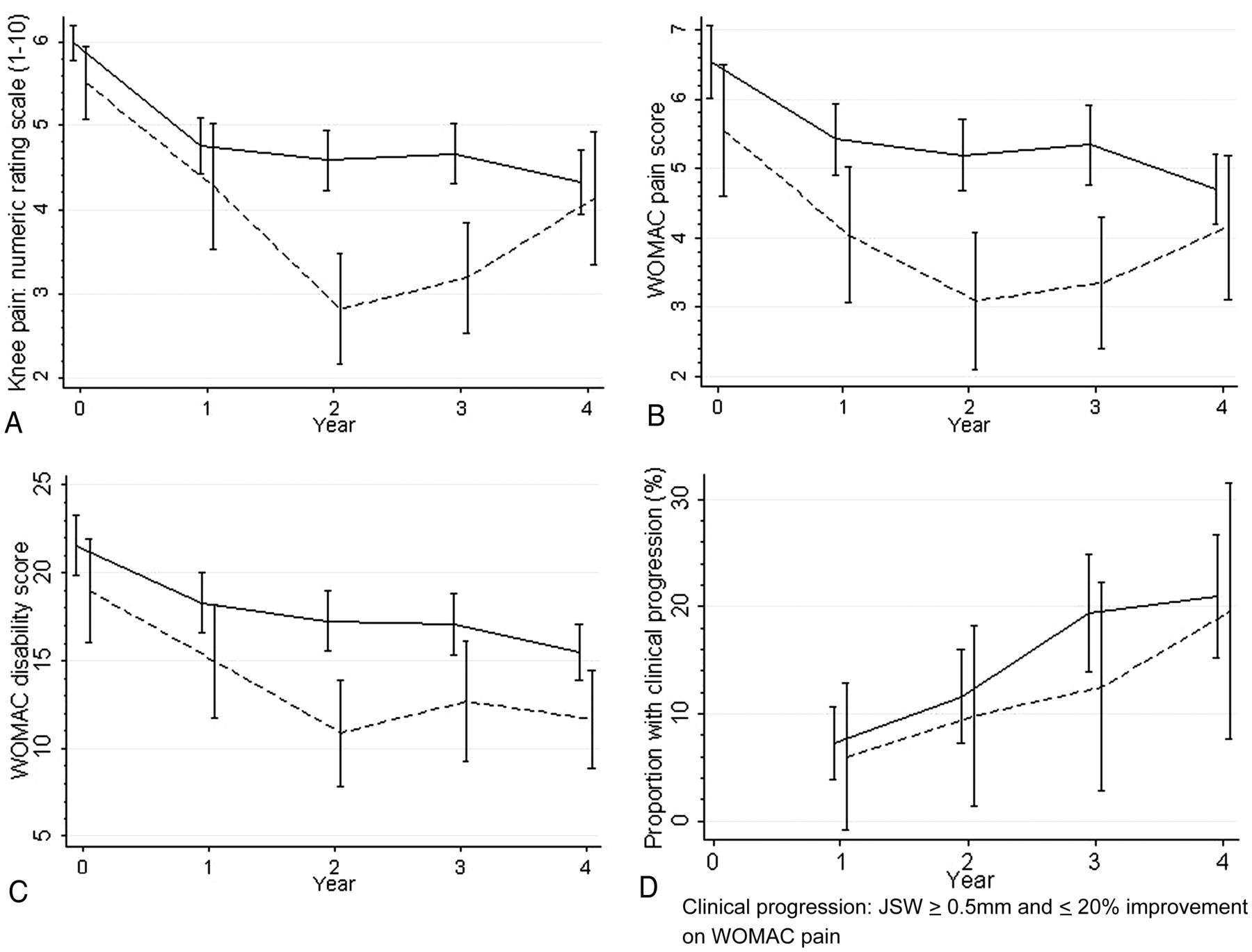
The effect of time on numeric rating scale in the non-users was modelled using quadratic and cubic terms, and the effect of bisphosphonate use modelled using quadratic and cubic interaction terms. Numeric rating scale scores reduced in both groups between baseline and 1 year, with differences between groups the largest at years 2 and 3. Differences were statistically significant at both year 2 and 3 (−0.97, p=0.001 at year 2, −1.15, p=0.004 at year 3). By year 4, users and non-users had similar numeric rating scale scores (table 4, figure 1A).
Effect of bisphosphonate use on radiographic and clinical measures of knee osteoarthritis over 4 years of observation
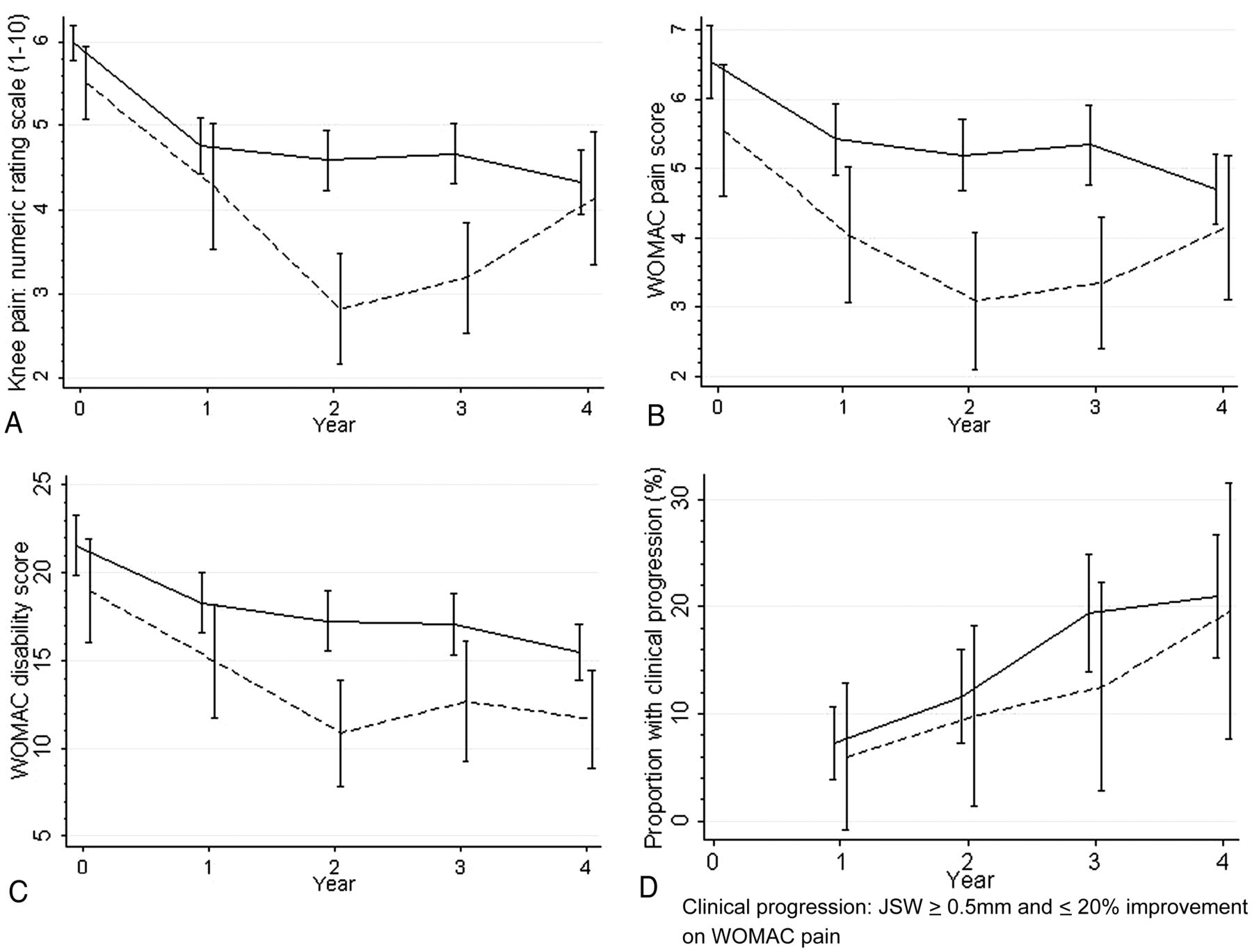
Relationship between bisphosphonate use and clinical outcomes. (A) Pain scores (numeric rating scale) over 4 years of observation, by bisphosphonate use (unadjusted data). (B) Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC) pain scores over 4 years of observation, by bisphosphonate use (unadjusted data). (C) WOMAC disability scores over 4 years of observation, by bisphosphonate use (unadjusted data). (D) Radioclinical progression over 4 years of observation, by bisphosphonate use (unadjusted data). Solid line: non-users; dashed line: bisphosphonate users.
WOMAC pain, disability and stiffness
WOMAC pain scores reduced over time in both bisphosphonate users and non-users, with the rate of change non-linear in both groups (figure 1B). The effect of time was modelled using a quadratic effect in non-users, and the effect of bisphosphonate use modelled using a quadratic interaction term. Groups were most different at year 2 (−0.72 units for pain; 2.85 units for disability), but differences were not statistically significant. Differences narrowed by year 4. There was no effect of bisphosphonate use on the stiffness score.
WOMAC disability scores were linear over time for non-users, but the effect of bisphosphonate use was modelled using a quadratic interaction term (figure 1C). Differences in WOMAC disability score were not significant at any time point. WOMAC stiffness scores were modelled using a quadratic effect in non-users, but interaction terms were not significant, with no effect of bisphosphonate use on the stiffness score.
Radiological changes
JSW reduced linearly over time in both groups. The difference in JSW between bisphosphonate users and non-users reached 0.35 mm by year 4 (p=0.06) (table 4, figure 2).

{kind=link}
{kind=link}
Relationship between bisphosphonate use and radiological outcomes. (A) Medial minimum joint space width over 4 years of observation, by bisphosphonate use. (B) Radiological progression over 4 years of observation, by bisphosphonate use (unadjusted data).
The proportion of participants with radiological and radioclinical progression increased over time both in bisphosphonate users and non-users. Incidence of progression was lower in the bisphosphonate group (incidence rate ratio (IRR) of 0.63; p=0.04) after 3 years of observation. There was no difference in the incidence of radioclinical progression between users and non-users (table 4, figure 1D).
Joint replacements
The numbers of joint replacements in these cohorts were small and differences in numbers and rates of joint replacement were not statistically significant.
Discussion
This longitudinal study demonstrated reduction in numeric rating scale pain, differences in radiological progressors and trend to reduction of JSN in OAI participants meeting OA clinical trial inclusion criteria and reporting 3–5 years of bisphosphonate use, compared with similar participants not using bisphosphonates. Compliance in bisphosphonate use diminished by year 4, potentially reducing the effect size for bisphosphonate use. However, this study also suggests that bisphosphonate use (predominantly alendronate) does not result in sustained pain relief or structural protection after bisphosphonate discontinuation.
This study provides the longest reported period of observation for examining bisphosphonate effects on OA pain and structural endpoints. Randomised trials observed patients for a maximum of 2 years,20 and none followed participants once bisphosphonate used ceased, in order to investigate the effect of drug discontinuation on pain and structural outcomes.
Bisphosphonates may work through a variety of mechanisms, including effects on the subchondral bone and osteochondral junction.29 As bisphosphonates are reported to have anti-inflammatory actions,30 ,31 such effects may play a role in an immediate analgesic benefit, as distinct from that which might arise as a consequence of osteochondral structural alteration, and explain why analgesic benefits in this study did not persist beyond the period of drug use.
We observed discrepancies between the two measures of pain, as reduction in pain was significant for the numeric rating scale but not WOMAC total pain score. The time reference for these questions was identical (7 days) and both were Likert scales; therefore, differences in outcomes either reflect sensitivity to change of the measure, or the questions may assess different aspects of pain. The numeric rating scale may be a more true measure of pain intensity, whereas Rasch analyses of the WOMAC pain subscale have previously suggested that it measures a combined function–pain construct.32 ,33
Bisphosphonate users were older than non-users, but had similar baseline JSW, which persisted after adjustment for age and BMI (data not shown). One explanation for the baseline similarity is that most of the bisphosphonate users (76%) were existing rather than new users. Therefore, the bisphosphonate group could be 6 months further ahead in their bisphosphonate use than the data appears here, potentially minimising differences between groups and thereby reducing apparent effect size. We could have further limited our sample of bisphosphonate users to include only new users of bisphosphonates, but doing so would further limit the size of our sample. Another explanation is confounding by indication; some persons were more likely to receive bisphosphonate therapy even with the same risk factors due to a third factor, such as health literacy or access to healthcare.
Bisphosphonates have well-defined beneficial effects on BMD in the osteoporosis literature, increasing BMD and thereby reducing fracture risk.34 However, the relationship between systemic and subchondral BMD in OA is not clearly defined.16
The Fracture Intervention Trial demonstrated increased systemic BMD with alendronate use,35 and post hoc analyses showed that alendronate decreased osteophyte progression and disc space narrowing at the thoracic and lumbar spine between the 3- and 4-year follow-ups.36 However, high systemic BMD increased the risk of incident knee OA (but not radiographic progression) in a multicentre OA trial.37 At the subchondral bone, data are also mixed; some studies show lower than expected subchondral BMD in persons with knee OA,38 ,39 yet others showed that elevated subchondral BMD was associated with deleterious effects on radiographic markers of OA cross sectionally40–42 and longitudinally.15 Therefore, while the mechanism and direction of effect remains controversial, the evidence suggests that bisphosphonates have effects at the subchondral bone. Longitudinal studies (especially randomised trials) are required to assess the effect on patients with OA.
The effects of bisphosphonates on bone and cartilage endpoints would be expected to take months or years to be evident. In terms of structural endpoints, we observed a trend of reduction of joint space loss over the 4-year period of observation with reduction in the proportion of progressors in the bisphosphonate group. Clinical trials with structure modification endpoints typically require hundreds of patients per arm to demonstrate a statistically significant effect over time. Therefore, the 55 bisphosphonate users and 268 non-users meeting the clinical trial criteria in the OAI result in suboptimal power to assess structural endpoints. Additionally, the reduction in compliance in this cohort diluted differences between bisphosphonate users and non-users from year 4, further reducing available power.
The strengths of this study include the large size of the underlying cohort (the OAI), the long duration of follow-up (4 years, with data collection ongoing) and the comprehensive nature of data collection, including radiology and clinical data. Additionally, as bisphosphonates are already off patent or soon to be off patent, large randomised trials of bisphosphonate use with OA outcomes over such long periods of time (4–5 years) are unlikely to occur, rendering observational studies more valuable.
There are other limitations to this study. As this was an observational study rather than a randomised clinical trial, there were baseline differences between bisphosphonate users and non-users, and we cannot be certain that the groups were otherwise statistically equivalent. Bisphosphonate use was self-reported simply as use or non-use and we have no method to validate compliance. While bisphosphonate users mostly used alendronate, use of other bisphosphonates occurred, and the existing sample size precluded further subgroup analyses. These agents have different potencies and slightly different mechanisms of action, which could affect the pain and structural modification outcomes. Poor compliance with oral bisphosphonates continues to be an ongoing concern in the community.43 ,44 We limited our bisphosphonate users to those using bisphosphonates for 3, 4 or 5 years, but only 50% of these patients used for all 5 years. While this potentially reduces the effect size detected, it does reflect treatment patterns in the community, and therefore provide good external validity for the findings.
In summary, this paper further strengthens the concept that treatment with bisphosphonates may have beneficial symptomatic and perhaps structural benefits for people with OA. Therapeutic agents with bone-modifying potential require further exploration for a field lacking effective therapeutic options.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online table
Footnotes
Handling editor Tore K Kvien
-
Contributors PGC and MB conceived the study. LL, SRK, EMAH, MB and PGC analysed and interpreted the data. LLL, SRK, EMAH and PGC drafted the manuscript. LLL, SRK, EMAH, MB and PGC approved the final version for submission.
-
Funding SRK, EMAH and PGC are funded in part by Arthritis Research UK and the NIHR Leeds Musculoskeletal Biomedical Research Unit. LLL was funded by an OARSI Young Investigator Scholarship. The OAI is a public–private partnership comprised of five contracts (N01-AR-2-2258; N01-AR-2-2259; N01-AR-2-2260; N01-AR-2-2261; N01-AR-2-2262) funded by the National Institutes of Health, a branch of the Department of Health and Human Services, and conducted by the OAI Study Investigators. Private funding partners include Merck Research Laboratories; Novartis Pharmaceuticals Corporation, GlaxoSmithKline; and Pfizer, Inc. Private sector funding for the OAI is managed by the Foundation for the National Institutes of Health.
-
Competing interests None.
-
Patient consent Obtained.
-
Ethics approval Committee on Human Research, University of California, San Francisco (IRB approval number 10-00532).
-
Provenance and peer review Not commissioned; externally peer reviewed.
-
Data sharing statement This manuscript was prepared using an OAI public use data set and does not necessarily reflect the opinions or views of the OAI investigators, the NIH, or the private funding partners.