Article Text

Abstract
Objective To evaluate the effects of a mindfulness-based group intervention, the Vitality Training Programme (VTP), in adults with inflammatory rheumatic joint diseases.
Methods In a randomised controlled trial, the VTP—a 10-session mindfulness-based group intervention including a booster session after 6 months—was compared with a control group that received routine care plus a CD for voluntary use with mindfulness-based home exercises. The primary outcome was psychological distress measured by the General Health Questionnaire-20. Self-efficacy (pain and symptoms) and emotion-focused coping (emotional processing and expression) were used as co-primary outcomes. Secondary outcomes included pain, fatigue, patient global disease activity, self-care ability and well-being. Effects were estimated by mixed models repeated measures post-intervention and at 12-month follow-up.
Results Of 73 participants randomised, 68 completed assessments post-intervention and 67 at 12 months. Significant treatment effects in favour of the VTP group were found post-treatment and maintained at 12 months in psychological distress (adjusted mean between-group difference −3.7, 95% CI −6.3 to −1.1), self-efficacy pain (9.1, 95% CI 3.4 to 14.8) and symptoms (13.1, 95% CI 6.7 to 19.3), emotional processing (0.3, 95% CI 0.02 to 0.5), fatigue (−1.1, 95% CI −1.8 to −0.4), self-care ability (1.0, 95% CI 0.5 to 1.6) and overall well-being (0.6, 95% CI 0.1 to 1.2). No significant group differences were found in emotional expression, pain or disease activity.
Conclusion The VTP improved most primary and secondary outcomes compared with individual use of CD exercises. Improvements were maintained at 12 months, suggesting that the VTP is a beneficial complement to existing treatments for patients with inflammatory rheumatic joint diseases.
Statistics from Altmetric.com
Introduction
Inflammatory rheumatic joint diseases such as rheumatoid arthritis (RA), ankylosing spondylitis (AS) and psoriatic arthritis generally cause symptoms of pain, fatigue and functional limitations that can place long-term stress on individuals.1,–,3 Several studies have shown increased psychological distress and reduced emotional well-being in patients with rheumatic diseases.4,–,7 Substantial recent advances in the medical treatment of these conditions have improved the quality of life for many patients.8,–,10 However, treatment strategies are more effective in patients with disease of recent onset than in patients with established disease, not all patients are eligible for the new medications, and the disease process is still only partly controllable.11 Many patients need to make demanding lifestyle changes. There is therefore a need for complementary interventions that enhance individuals' health-promoting resources and help them to adjust to their disease.12
The majority of interventions that have been designed to strengthen patients' coping abilities, such as self-management programmes and cognitive behavioural therapy (CBT), have focused on improving individuals' cognitive coping skills by means of goal-setting, problem-solving and modifying negative thoughts.12,–,16 However, the effects of these interventions are generally found to be short-lived,17,–,19 suggesting that patients may find disease management burdensome and difficult to integrate into their lives.12 More recent studies have shown that acknowledgement and expression of stressful disease-related emotions are an essential part of adjustment to chronic disease.12 20 A range of approaches categorised as mindfulness- and acceptance-based therapies have advocated the importance of non-judgemental attention to unwanted thoughts, feelings and bodily experiences without attempting to avoid or change them.21 It is believed that experiencing the present moment with an attitude of openness, acceptance and curiosity can effectively counter the effects of stressors, whereas excessive orientation towards the past or future can be related to feelings of depression and anxiety.16 22 23 A recent meta-analytical review concluded that mindfulness-based therapy is effective for improving anxiety and depressive symptoms in patients with various chronic disorders including RA.24 A study in which patients with RA were randomly assigned to CBT, mindfulness-based therapy or an education control group found favourable effects of the mindfulness-based intervention in coping efficacy and pain management in patients with recurrent depression.
The Vitality Training Programme (VTP) is a mindfulness-based group intervention that particularly addresses the relationship between thoughts, emotions and bodily experiences.25 26 Rather than focusing on strategies to reduce symptoms, the VTP aims at strengthening the personal resources of individuals and enhancing their capacity to engage responsibly and satisfactorily in the process of everyday living. The VTP was originally developed and tested for persons with chronic musculoskeletal pain27,–,29 and has been adjusted for persons with inflammatory arthritides (IA) in a pilot study.30 Participants' experiences from the VTP have been explored in a qualitative focus group study.31
The present study is the first randomised controlled trial of the VTP in patients with IA. Our specific objective was to evaluate whether participation in the VTP could improve psychological well-being, self-efficacy and emotion-focused coping in this group of patients.
Methods
Study design
In this randomised controlled trial, participants in the VTP were compared with a routine care control group that received a CD with mindfulness-based home exercises for individual voluntary use. Participants were assessed at baseline, post-intervention and after 12 months.
Participants
Women and men aged 20–70 years diagnosed with an inflammatory rheumatic joint disease at least 1 year earlier were eligible for inclusion and were recruited from three rheumatology departments in south-eastern Norway between March 2007 and June 2009. Inability to understand Norwegian was an exclusion criterion.
A project assistant at each department (TØH, LRE, AKL) asked patients who regularly visited their clinics to participate. In addition, participants were recruited from random samples of patients drawn from two registers at Diakonhjemmet Hospital in Oslo fulfilling the American College of Rheumatology 1987 criteria for RA and the New York classification criteria for AS. All interested participants attended information meetings chaired by the project assistants. Participants received oral and written information about the intervention and the study procedures before deciding whether to take part and gave informed consent before inclusion.
Intervention
The VTP comprised 10 group sessions over a period of 15 weeks plus a booster session approximately 6 months after the end of the course (see figure S1 in online supplement). Each session lasted 4.5 h and addressed a specific topic related to living with chronic illness (table 1).
Topics addressed in each session
The number of participants in each VTP group ranged from 8 to 12. Through mindfulness-based exercises, participants were encouraged to become aware of, and intentionally attend to, their emotions, thoughts and bodily experiences. In addition, various creative exercises, such as guided imagery, music, drawing, poetry and metaphors, were used to encourage experiential learning processes. Reflections on individuals' own experiences were promoted through writing, sharing and listening to one another within the group. Between sessions the participants performed awareness and relaxation training by listening to a CD with mindfulness-based exercises and wrote reflective diaries (see online supplement). The group facilitators were health professionals (ie, physiotherapists, occupational therapists, nurses and social workers) who had been trained in mindfulness-based exercises (awareness) and delivery of the VTP. The training comprised six 3-day workshops over 1 year, together with home assignments and a practical examination at the end of the training. They were specially trained not to give advice or to present the ‘right answers’, but to help individuals explore and discover their individual resources and personal values and to find their own meaningful answers.25 The topics and methods were described in a manual used by all the group facilitators.
Participants in the control group were informed that they would be invited to participate in the VTP after all data collection was completed. Both groups received routine care throughout the study.
Outcomes
The primary outcome used for sample size calculation was psychological distress assessed by the General Health Questionnaire, 20-item version (GHQ-20), which balanced between positively-phrased items indicating psychological health and negatively-phrased items indicating psychological distress. In studies measuring change, scoring on a 4-point Likert scale (0–3) is recommended.32 33 This gives a possible sum score of between 0 (no distress at all) and 60 (much more distress than usual). A suggested threshold for serious psychological distress is a sum score above 23.33 The GHQ-20 has been validated and used in various samples of chronically ill persons in Norway.33,–,36
Two co-primary outcomes (self-efficacy and emotion-focused coping) were included. Self-efficacy was assessed by the pain (five items) and symptoms (six items) subscales of the Arthritis Self-Efficacy Scale. Each item is scored from 10 to 100 (100=‘totally confident’),37 and the Norwegian translation has been validated in previous prospective studies.38 Emotion-focused coping was assessed by the Emotional Approach Coping Scale (EAC) that measures ability to acknowledge and express emotions and comprises two subscales: emotional processing (eight items) and emotional expression (eight items).39 Each item is scored from 1 to 4 (4=in high degree). The EAC has been validated in Norwegian patients with rheumatic diseases.40
The secondary outcomes pain, fatigue and patient-reported global assessment of disease activity were assessed by Numerical Rating Scales (NRS) scored from 0 to 10 (where 10 is intolerable pain/fatigue/very bad symptoms). Self-care ability and overall well-being were assessed by NRS scored from 0 to 10 (where 10 is very good).
The participants completed a comprehensive questionnaire including all outcome measures at baseline, post-intervention (ie, immediately after the 10 group sessions) and at the 12-month follow-up. Questionnaires were sent to all participants with a postage-paid return envelope. In addition to being included in the questionnaires, psychological distress and the secondary outcomes of pain, fatigue, global disease activity, self-care ability and overall well-being were measured by telephone interviews four times at 2-week intervals at each assessment point—that is, a total of five measurements of these outcomes (see figure S1 in online supplement).
Sample size
Because there are no clear recommendations in the literature about what a clinically relevant change in the GHQ-20 might be, we based our sample size calculation on our previous pretest–post-test study.30 However, because of the considerable day-to-day variation in self-reported health status in patients with inflammatory rheumatic joint diseases, a previous study in Norwegian patients with RA has shown that using up to five repeated measurements per patient can decrease the between-person SD and consequently the number of patients required in a trial by as much as 20%.41 We therefore conducted a pilot study in which we calculated the individual means for five repeated measures on the GHQ-20 at baseline and the follow-up visits. The α value was set at 0.05 (type I error) and β at 0.2 (type II error). Based on this study, we hypothesised that the randomised controlled trial would detect a difference between groups of 4.5 in GHQ-20 with an estimated SD of 3.9 and a probability of a slight improvement of 0.9 in the control group. A bootstrap procedure was performed, and the sample size was calculated as 34 in each group.
Randomisation and blinding
A statistician generated randomisation lists using Statistical Analysis System (SAS) version 9.1.3, with blocks of 10 and 15 for each department to ensure approximately equal sample sizes. Participants were given consecutive numbers and a person not involved in the data collection or intervention allocated each participant to the corresponding number on the randomisation list.
The persons conducting telephone interviews were blinded for group assignments, and participants were instructed not to discuss their intervention with the interviewer. A blinded statistician conducted statistical analyses. The randomisation code was not opened until the primary analyses were completed.
Statistical analyses
The average mean values of the five repeated measurements, as well as the single means of variables measured once at each time point, were used in the analyses. Treatment effects (mean differences between the groups post-treatment and at 12 months) were estimated with mixed models repeated measures analysis. This model includes the interaction of treatment and time (ie, post-treatment or 12 months). For each outcome measure we adjusted for the individual baseline values as well as for gender, age, disease duration, education and civil status, but none of these were significant in any model and were therefore removed. The mixed models analysis is robust to missing values because the patients are included at time points with non-missing values only. A parametric bootstrap procedure was applied to ascertain the robustness of the findings. The model assumptions were assessed using Cook's d and Covratio statistics for individuals as well as for the estimated covariance. The treatment effect sizes (Cohen's d statistic) were calculated as the adjusted between-group difference in scores divided by the pooled SD of the baseline scores for each variable.42
Data were analysed according to the intention to treat principle and p values ≤0.05 were considered statistically significant. The analyses were performed using SAS Version 9.2.
Results
Characteristics of participants
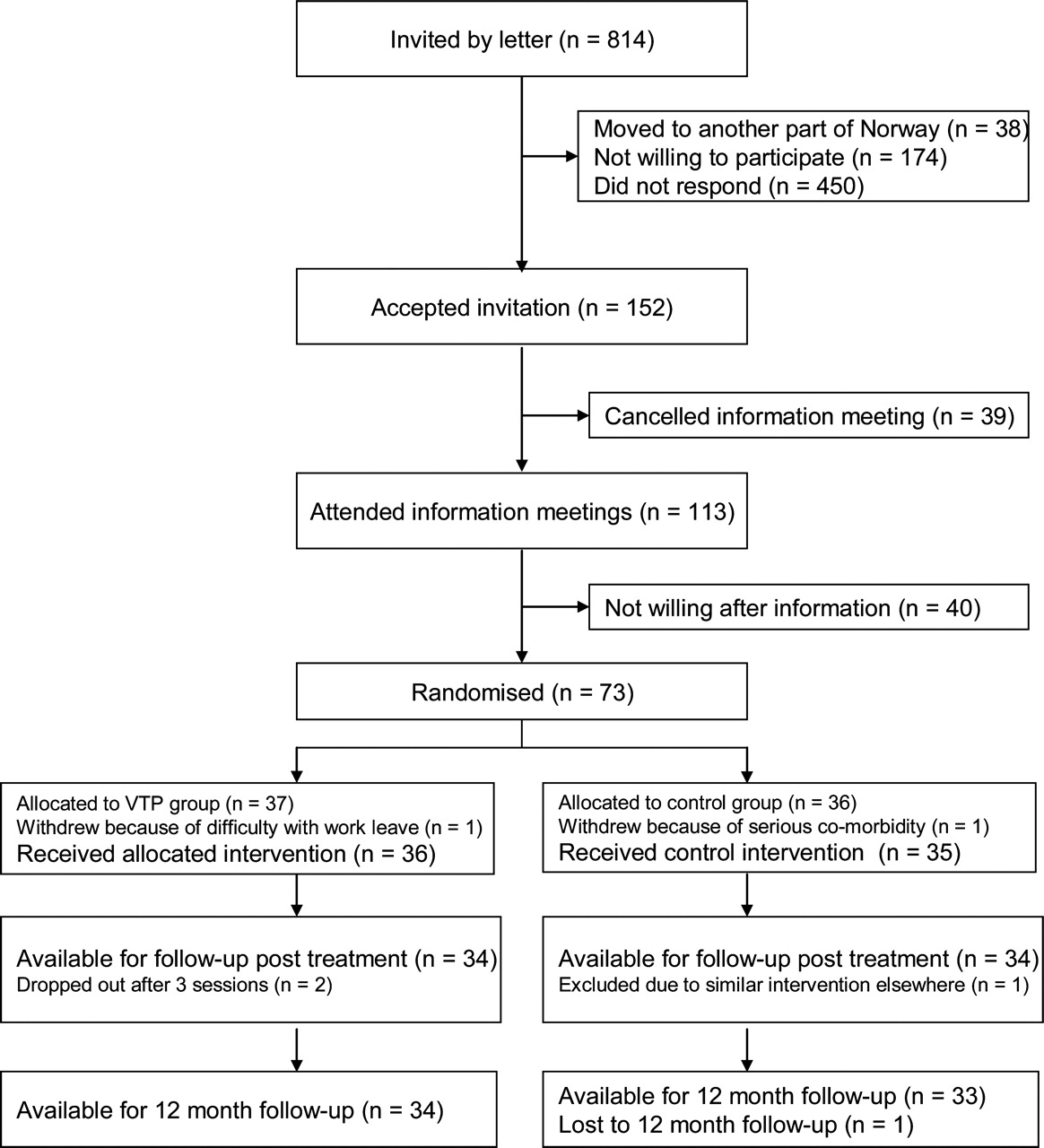
From a total of 814 invited subjects, 113 (14%) attended the information meetings. Seventy-three were willing to participate in the study and were randomised (37 to VTP and 36 to the control group, figure 1). The VTP and control groups were well matched at baseline with regard to demographic and disease variables (table 2) and all outcome measures; p values ranged from 0.13 to 0.95. Ten subjects in the control group and 13 in the VTP group exceeded the GHQ-20 threshold of 23. There were no significant differences between the various diagnostic groups in any of the outcome measures at baseline.

{kind=link}
Flow chart of participants. VTP, Vitality Training Programme.
Baseline characteristics of participants allocated to the VTP group or routine care plus individual voluntary use of mindfulness-based home exercises on CD
The subjects who completed the VTP attended an average of 9 sessions (range 6–10). Twenty-five subjects (69%) took part in the booster session. Sixty-eight subjects (93%) were available for follow-up after treatment (34 in each group) and 67 (92%) completed the 12-month assessments (34 in the VTP group and 33 in the control group; figure 1).
Primary outcomes
Significant treatment effects in favour of the VTP group were found post-treatment and at 12 months in psychological distress (GHQ-20), self-efficacy pain and symptoms, and emotional processing (table 3). Mean treatment effects in psychological distress were −4.7 (95% CI −7.8 to −1.8) post-treatment and −3.7 (95% CI −6.3 to −1.1) at 12 months, effect sizes 0.73 and 0.58, respectively. Both groups showed a slight reduction in distress from post-treatment to 12 months. In the VTP group the number of subjects exceeding the GHQ-20 threshold of 23 was reduced from 13 (36%) at baseline to 2 (6%) at 12 months compared with 10 (29%) at baseline to 8 (24%) at 12 months in the control group (p=0.045). Treatment effects in self-efficacy pain and symptoms increased slightly from post-treatment to 12 months in favour of the VTP group, effect sizes 0.59 and 0.92, respectively. No significant between-group effects were found in emotional expression (table 3). However, there were significant within-group changes in emotional expression from baseline to 12 months (p=0.03 in the VTP group and p=0.04 in the control group).
Mean (95% CI) scores and treatment effects (differences post-treatment and 12 months) and overall p values estimated with mixed models linear repeated measures analysis*
Secondary outcomes
Significant treatment effects in favour of the VTP group were found post-treatment and at 12 months for fatigue, self-care ability and overall well-being. The improvement in fatigue was increased at 12 months in the VTP group whereas the control group was unchanged from baseline. The mean treatment effect at 12 months was −1.1 (95% CI −0.4 to −1.8), effect size 0.50 (table 3). Effects in pain and the patient global assessment of disease activity did not reach statistical significance; mean effects were −0.6 (95% CI −1.28 to 0.02) and −0.7 (95% CI −1.4 to −0.05), respectively (table 3). No adverse events were reported.
Discussion
In this randomised controlled trial we found that the VTP group improved significantly in most primary and secondary outcomes compared with a routine care control group that received a CD with mindfulness-based home exercises for voluntary use. After 1 year the number of subjects with serious psychological distress in the VTP group was reduced from 13 to 2 compared with a reduction of from 10 to 8 in the control group. Moreover, the treatment effects in self-efficacy pain and symptoms and in fatigue increased from post-treatment to 12 months. As opposed to results from other psychoeducational interventions for people with arthritis that have documented only short-term transient effects,17,–,19 this study showed maintained improvements in the VTP group 1 year after the intervention. These lasting improvements indicate that the participants may have incorporated some mindfulness strategies into their daily lives and that these strategies have strengthened their ability to respond to their stressful experiences in a more flexible way, which has also been reported in a previous qualitative study.31
Although there has been an increasing focus on the impact of fatigue in patients with inflammatory arthritis in recent years,3 43,–,45 only a few studies on interventions aimed at improving the ability of individuals to cope with fatigue have been published.46 Individual and group CBT interventions with a special focus on fatigue have been found to improve fatigue impact and coping in patients with RA.47,–,49 The VTP did not address fatigue explicitly. However, through mindfulness practice, the participants learnt to be more fully present in their immediate experiences without making an effort to avoid or change them. In addition, the creative exercises used in the VTP were directed at helping participants to discover more of their health-promoting resources and to make choices consistent with their personal values. These may well be energy-releasing processes. Some studies have reported an association between fatigue and psychological distress.3 44 It is possible that improvement in psychological distress might have mediated a reduction in fatigue. However, this association will have to be investigated further.
The VTP explicitly addressed disease-related emotions and aimed at helping individuals to attend to their emotions in an open non-judgemental way. As hypothesised, the VTP group significantly increased their emotional processing (ie, acknowledging and understanding emotions) compared with the control group. There is an increasing body of evidence showing that avoidance and inhibition of emotions is associated with maladaptive outcomes of chronic somatic diseases, whereas recognising and expressing emotions may decrease the stressful impact of negative emotions such as anger, fear and self-blame.12 20 However, it may be questioned whether the ability to understand and express emotions is a mediator of psychological distress and should have been included as a process measure rather than outcome. This remains a question for further research.
Interestingly, psychological distress and emotional expression improved in both groups at the 12-month follow-up. To compensate for the negative effects from being allocated to routine care only, the control group received a CD with mindfulness-based home exercises for voluntary use. Additionally, the control group was called four times at 2-week intervals on three occasions during the control period. Although we do not consider this attention to be comparable with the attention given to the VTP group, the fact that someone asked participants about emotional issues 12 times during the year may have increased their awareness and thus partly explain the improvements in the control group.
Some limitations have to be addressed. First, only a small sample of the people approached enrolled in the study, which probably reflects a selection bias in the direction of highly motivated individuals. Consequently, the results cannot be generalised to the whole population of persons with IA. However, from our clinical experience we know that there are waiting lists for the existing VTP courses, and that the low uptake may partly be explained by unwillingness to participate in a randomised controlled trial. In order to obtain a sufficient sample size for the trial, we therefore approached people on patient registers who did not regularly visit the clinics and whom we assumed had not heard about the VTP before. We do not know if these patients were in need of such an intervention at the time they were approached. However, the majority of the people who enrolled in the VTP attended between 8–10 sessions, suggesting high commitment to the intervention. Also, the calculated sample size based on five repeated measures of the primary outcome was achieved and the completeness of the data collection was satisfactory, with 92% of participants completing the 12-month follow-up assessments.
Second, the baseline data were collected after randomisation. The reason for this was pragmatic; the participants needed to know which group they were allocated to as early as possible in order to plan their time schedule, and the data collection by five repeated measurements extended over 2 months with the last assessment the day before the intervention. This might have biased the responses, but the baseline data showed that the groups were well matched on all variables. The participants were asked not to tell the telephone interviewers which group they were allocated to and, according to the interviewers, the participants complied with this instruction. Moreover, none of the interviewers was involved in the intervention.
Third, multiple primary outcomes were included. The reason for this was that we hypothesised that the VTP, in addition to reducing psychological distress, would have beneficial effects on self-efficacy and emotion-focused coping. However, these outcomes could equally be characterised as process measures. The associations between these measures will have to be analysed in further studies.
Finally, all the outcome measures in this trial were patient-reported, and the core set for disease activity measurement was not included. However, most outcomes used in this trial are validated and widely used within rheumatology, and a strength of patient-reported outcomes is that they reduce the effect of observer bias.
Conclusions
This randomised controlled trial has shown that the VTP, a 10-session mindfulness-based group intervention that explicitly addresses emotion-focused topics and includes a booster session after 6 months, significantly improved psychological distress, self-efficacy, processing of emotions and fatigue. Improvements were maintained at the 12-month follow-up. The VTP may be considered as a beneficial complement to existing treatments in subjects with IA, particularly for those who experience heightened psychological distress and fatigue. Further studies should be conducted to evaluate the comparative effectiveness of the VTP and other group interventions such as CBT interventions.
Acknowledgments
The authors thank the group facilitators Guro Mjønner, Innlandet Hospital, Astrid Jonassen, Betanien Hospital and May Britt F Lyngroth and Anne Tøvik, Diakonhjemmet Hospital. The authors would also like to thank Aase Frich, Diakonhjemmet Hospital, for secretarial help and all the telephone interviewers for their invaluable work on this project. The authors owe special thanks to all the patients who made this study possible.
References
Supplementary materials
Press release of this article.
Files in this Data Supplement:
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Web Only Data - This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
- Web Only Data - This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
-
Funding The study was supported by Diakonhjemmet Hospital.
-
Competing interests None.
-
Ethical approval The study protocol was approved by the Regional Committee for Medical Research Ethics and the Data Inspectorate.
-
Provenance and peer review Not commissioned; externally peer reviewed.