Article Text

Abstract
Objectives To study the impact of the introduction of biological disease-modifying anti-rheumatic drugs (bDMARDs) and associated rheumatoid arthritis (RA) management guidelines on the incidence of total hip (THR) and knee replacements (TKR) in Denmark.
Methods Nationwide register-based cohort and interrupted time-series analysis. Patients with incident RA between 1996 and 2011 were identified in the Danish National Patient Register. Patients with RA were matched on age, sex and municipality with up to 10 general population comparators (GPCs). Standardised 5-year incidence rates of THR and TKR per 1000 person-years were calculated for patients with RA and GPCs in 6-month periods. Levels and trends in the pre-bDMARD (1996–2001) were compared with the bDMARD era (2003–2016) using segmented linear regression interrupted by a 1-year lag period (2002).
Results We identified 30 404 patients with incident RA and 297 916 GPCs. In 1996, the incidence rate of THR and TKR was 8.72 and 5.87, respectively, among patients with RA, and 2.89 and 0.42 in GPCs. From 1996 to 2016, the incidence rate of THR decreased among patients with RA, but increased among GPCs. Among patients with RA, the incidence rate of TKR increased from 1996 to 2001, but started to decrease from 2003 and throughout the bDMARD era. The incidence of TKR increased among GPCs from 1996 to 2016.
Conclusion We report that the incidence rate of THR and TKR was 3-fold and 14-fold higher, respectively among patients with RA compared with GPCs in 1996. In patients with RA, introduction of bDMARDs was associated with a decreasing incidence rate of TKR, whereas the incidence of THR had started to decrease before bDMARD introduction.
- rheumatoid arthritis
- dmards (biologic)
- epidemiology
- orthopedic surgery
- anti-tnf
Statistics from Altmetric.com
Introduction
In uncontrolled or severe rheumatoid arthritis (RA), inflammation can lead to irreversible joint damage.1–3 In end-stage joint damage, prosthetic replacement of the damaged joint is the only available treatment. A recent study from the UK showed that the accumulated burden of disease activity measured by the disease activity score with 28-joint count (DAS28) within the first 5 years following diagnosis predicted the need for major joint surgery, and the highest incidence rates of surgery were observed among patients with moderate and high disease activity.3 These findings lend further support to the importance of early and aggressive treatment emphasised in current RA treatment guidelines.4 5 In non-contemporary RA cohorts, it was found that more than 50% of patients required joint surgery during the course of their disease.6 7
The introduction of tumour necrosis factor-alpha inhibitors (TNFi) as the mainstay of biological DMARDs (bDMARDs) in the late 1990s has improved the treatment of RA and shown to halt radiographic progression and development of joint erosions,1 8 but it is unclear if these properties translate into a decreased need for total joint replacements. Most studies have suggested a decrease in the incidence of joint surgery following introduction of bDMARDs,9–15 but studies showing no changes or increased number of joint surgeries have also been published.9 10 16 17
If treatment with bDMARD reduces the need for joint replacements, this will likely change the cost-effectiveness of these drugs. Joint replacements are expensive procedures and carry the risk of potential adverse events; and risk estimates for complications are increased in patients with RA.18
Using data from national Danish healthcare registers, we aimed at investigating the possible impact of the introduction of bDMARDs and associated guidelines for TNFi treatment in Denmark in 2002 on the 5-year incidence rate of total hip replacements (THR) and total knee replacements (TKR) in patients with incident RA compared with general population comparators (GPCs).
Patients and methods
Study design
This is a register-based, nationwide interrupted time-series analysis,19 20 investigating the impact of introduction of bDMARDs in Denmark for the treatment of RA on the 5-year incidence rate of THR and TKR. Study methods and results are reported in accordance with Strengthening the Reporting of Observational Studies in Epidemiology guidelines.21
Setting
All Danish residents have a personal identification number consistent throughout all registers making register-linkage possible. The study period was from 1 January 1996 to 31 May 2016.
Data sources
The Civil Registration System (CRS) captures all deaths and migrations among Danish residents.22 From CRS, we obtained dates of birth, emigration and death for all patients. Furthermore, CRS was used for the procedure of matching patients with RA with GPCs.
The Danish National Patient Register (DNPR) includes information on all inpatient (1977) and outpatient (1995) visits at Danish hospitals and private clinics.23 Discharge diagnoses have been registered in accordance with the International Classification of Diseases (ICD) 10th edition since 1994, and from 1996, surgeries have been coded in accordance with the Nordic Medico-Statistical Committee (NOMESCO) Classification. With every discharge, information is provided on up to 20 diagnoses. For descriptive purposes, we obtained information on comorbidities in DNPR for both study populations (see online supplementary table S1 for ICD-10 codes).
Supplementary file 1
DANBIO is a nationwide Danish rheumatology register established in 2000 to monitor the development in use and efficacy of bDMARDs.24 The DANBIO steering committee publishes annual reports available online.25
Study population
Patients with RA
Patients with RA were identified using DNPR. We included all incident patients who received a diagnosis of RA (ICD-10: M05-06) at a hospital department or private clinic specialised in rheumatology or general internal medicine in the period of 1 January 1996 to 31 May 2011. A study by Thygesen et al found a high positive predictive value of DNPR diagnoses for conditions included in the Charlson Comorbidity Index with the positive predictive value of 98% for connective tissue diseases, including RA.26
General population comparator
For each patient with RA identified, we matched with up to 10 persons from the general population of Denmark. Matching criteria were sex, year of birth and municipality. Matching was carried out only once and thus no replacement matching took place following subsequent patient exclusions. The date of RA diagnosis and corresponding matching date for GPCs is termed ‘index date’ throughout the remainder of this paper.
Exclusion criteria
Individuals aged <18 years at the index date were excluded. Patients and GPCs who had received a THR prior to index date were excluded for the THR analysis; likewise, individuals with previous TKR surgery were excluded in the TKR analysis.
Outcomes
Outcomes of interest were primary THR and TKR within 5 years of index date in patients with incident RA and GPCs. NOMESCO codes were used for identification of the procedures in DNPR (THR: KNFB; TKR: KNGB). As THR and TKR were analysed separately, patients and GPCs could potentially have both outcomes.
To allow patients diagnosed near the end of the study period to contribute with the same amount of follow-up time as those diagnosed in the first years of the study period, we focused on the first 5 years after diagnosis for all patients and GPCs. Patients with moderate-to-high disease activity score during the first year(s) of RA are at increased risk of major joint replacement surgery.3
Follow-up
Separate analyses for THR and TKR were undertaken. In analyses of THR, follow-up started at index date and ended at date of THR, death, emigration or 5 years of follow-up, whichever came first. For analyses of TKR, follow-up started at index date and ended at first occurrence of TKR, death, emigration or 5 years of follow-up.
Intervention
The time of the intervention—introduction of bDMARDs—was set to a 1-year period from 1 January 2002 to 31 December 2002 representing the time at which TNFi treatment was introduced for the treatment of RA in Denmark. Infliximab was available for treatment of RA in Denmark in 2000, but there were three main reasons for choosing 2002 as the time of intervention. Figures from the annual DANBIO report showed that the use of TNFi dramatically started to increase in 2002.25 27 Second, in 2002, three different TNFis were available for the treatment of RA, and according to the DANBIO figures, the use of each of these drugs increased.25 Third, the Danish Institute for Rational Pharmacotherapy published their first national guideline for TNFi treatment in November 2002.28
We introduced the 1-year lag period in 2002 as changes in prescription patterns and guideline implementation were likely ‘phased in’ during this period rather than abruptly changed overnight.
Statistical analyses
Demographics and descriptive data are presented by means and SD. Groups were compared by independent t test and χ2 test as appropriate.
We calculated the 5-year age and sex standardised incidence rates for THR and TKR separately among incident RA and GPCs, respectively, within each 6-month period from 1996 to 2011. An interrupted time-series analysis was carried out using biannual incidence rates of THR and TKR in two time segments: pre-bDMARD era (1996–2001) and bDMARD era (2003–2016) interrupted by the lag period in 2002.
We estimated the change in level (incidence rate/1000 person-years (pyrs)) and trend (Δ incidence rate/1000 pyrs per each 6-month period) in THR/TKR following the 1-year lag period in 2002. Using a backward stepwise procedure, the most parsimonious models were specified (P entry <0.05; P exit ≥0.20).20 Results are presented as 1996 baseline incidence rates; pre-bDMARD era trend; change in incidence rate at start of bDMARD era; and trend in bDMARD era. It is not uncommon for residuals from ordinary least-squares regression of time-series data to be temporally correlated. We therefore tested for first-order autocorrelation (not present) using Durbin-Watson tests, with all values of the test statistics being close to 2.0.20 Statistical analyses were performed using Stata V.13.1 (Stata, Texas, USA).
Sensitivity analyses
We performed a sensitivity analysis using data derived from incident patients and GPCs within 3-month periods instead of 6-month periods allowing us to inspect if results differed when the balance between the number of time points (2 vs 4 per year) and number of patients and events per time point changed. Furthermore, we tested models based on quarterly data for seasonality, which was not present.
Results
Baseline characteristics
We identified 30 404 patients with incident RA diagnosed between 1996 and May 2011 (online supplementary table S2) and 297 916 GPCs (online supplementary table S2 and figure S1). Following exclusion of patients and GPCs who prior to index date had received a THR or TKR, 29 427 patients with RA were eligible for comparison with 290 778 GPCs in THR analyses, and 29 703 patients with RA and 294 806 in TKR analyses (table 1). A higher proportion of patients with RA suffered from comorbidities (table 1 and online supplementary table S5).
Baseline characteristics of rheumatoid arthritis (RA) and general population comparators (GPCs) included in the interrupted time-series analysis for total hip replacement (THR) and total knee replacement (TKR), respectively
Total hip replacements
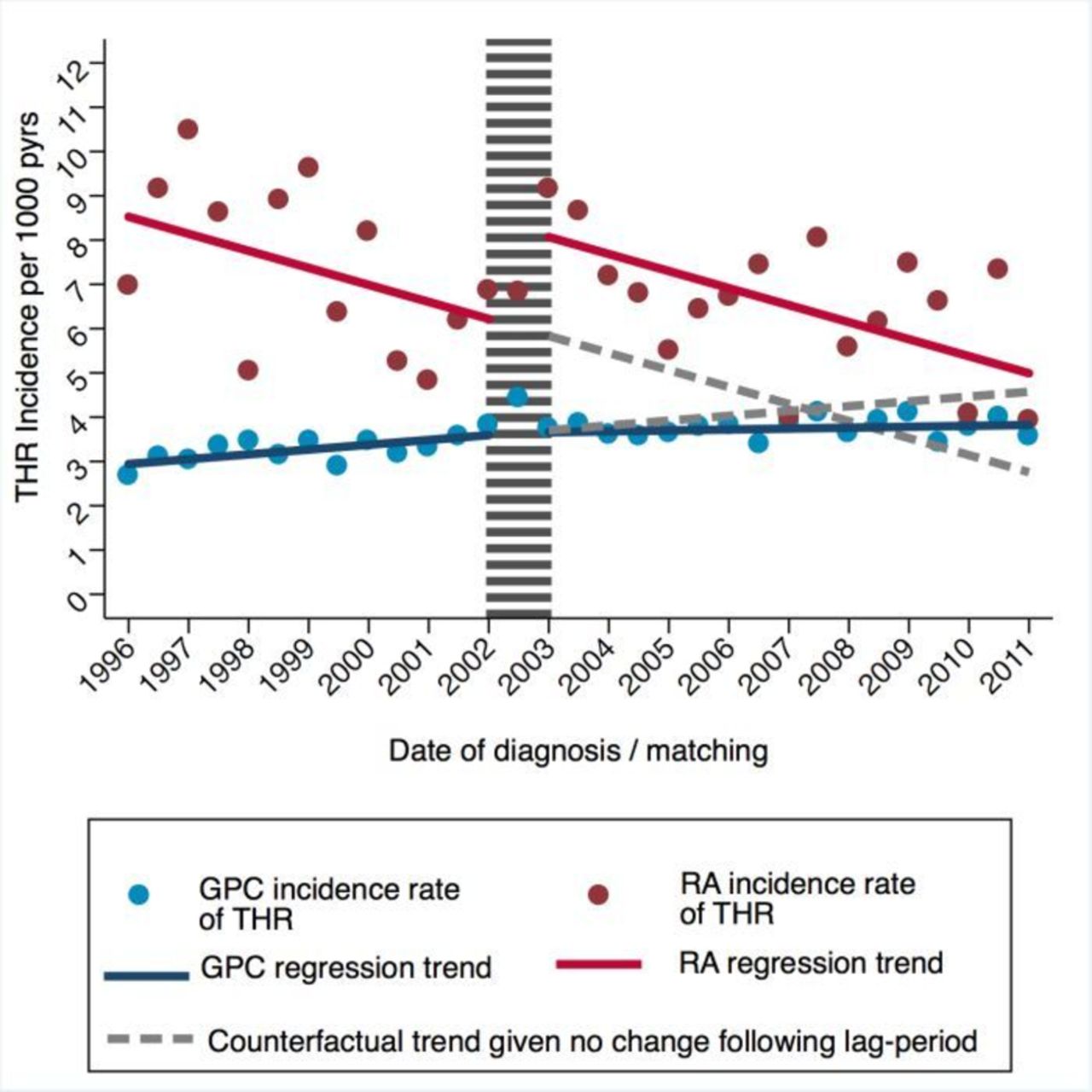
In patients with RA, the 5-year incidence rate of THR was 8.72/1000 pyrs (95% CI 7.48 to 9.95) at the start of 1996 compared with 2.89/1000 pyrs (95% CI 2.64 to 3.14) in GPCs (table 2 and figure 1). In the pre-bDMARD era from 1996 to end of 2001, there was a decreasing trend in the incidence rate of THR among patients with RA. Following the lag period in 2002, there was a borderline significant step change increase in incidence rate (+2.23 THR surgeries/1000 pyrs, P=0.075). Following the lag period, the incidence rate of THR continued to decrease at the same rate as observed in the pre-bDMARD era. In parallel, incidence rates of THR increased among GPCs throughout the whole study period, but to a lesser extent from 2003 and onwards (table 2 and figure 1). Overall, results did not differ from the primary analysis when using quarterly instead of biannually derived data (online supplementary table S3).
Changes in 5-year incidence rate of total hip replacement (THR) in patients with incident rheumatoid arthritis (RA) following introduction of biological DMARDs (bDMARDs) compared with secular trends in age, sex and municipality-matched general population comparators (GPCs)
Results from interrupted time-series analysis of changes in 5-year incidence rates (per 1000 person years (pyrs)) of total hip replacement (THR) in patients with rheumatoid arthritis (RA) compared with general population comparators (GPCs) following introduction of biological DMARDs in 2002.
Total knee replacements
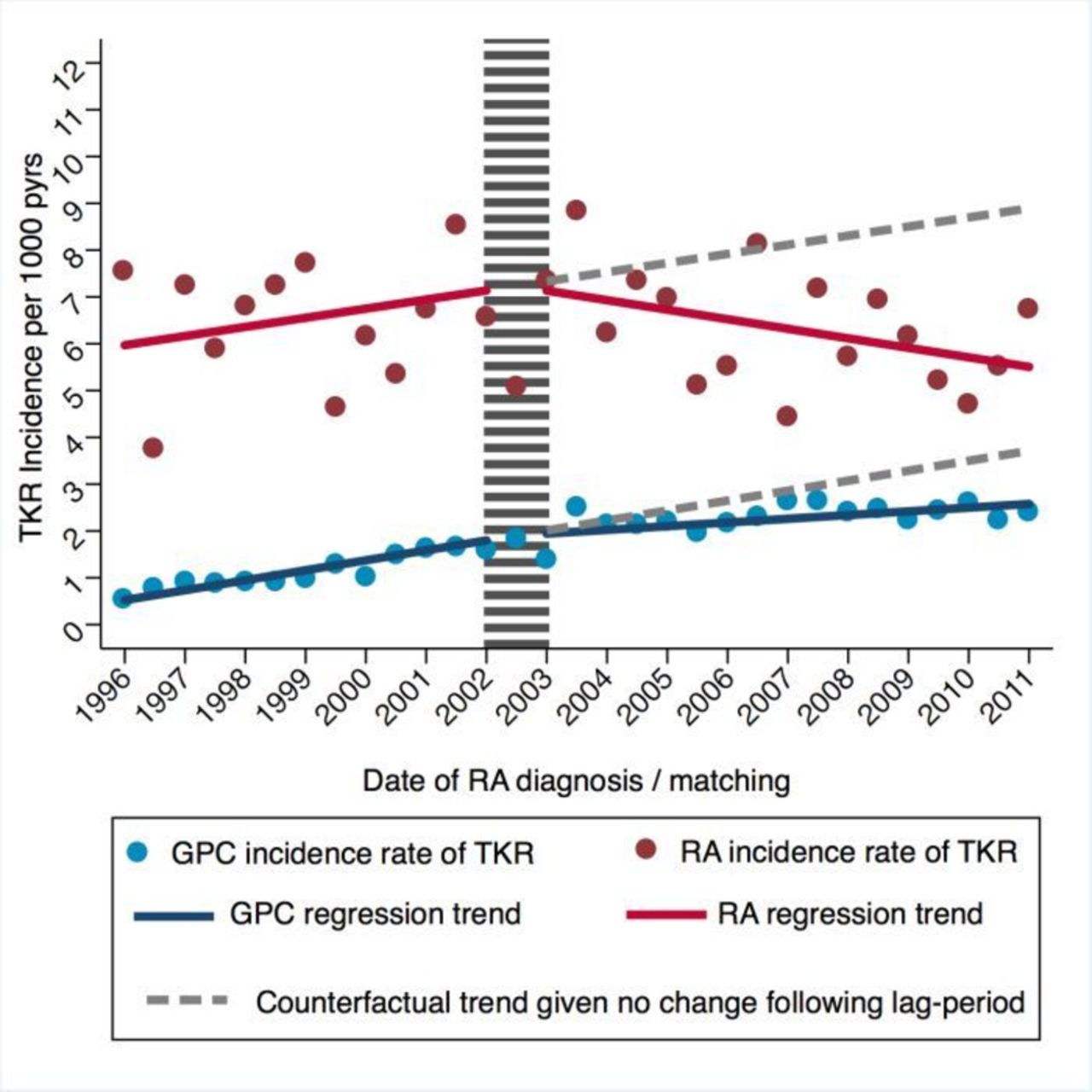
At the start of 1996, the age and sex standardised incidence rate of TKR was 14 times higher among patients with RA compared with matched GPCs: 5.87 vs 0.42/1000 pyrs (table 3). In the pre-bDMARD era, the incidence rate of TKR increased with +0.19 per year (P=0.173), but started to decrease with −0.20 per year (P=0.083) in the bDMARD era (figure 2). None of these trends were statistically significant. However, when applying quarterly instead of biannually derived data, the decreasing trend of TKR surgeries among patients with RA in the bDMARD era became statistically significant (−0.21 TKR surgeries/1000 pyrs per year, P=0.03) (online supplementary table S4 and figure S3).
{kind=link}
{kind=link}
Results from interrupted time-series analysis of changes in 5-year incidence rates (per 1000 person years (pyrs)) of total knee replacement (TKR) in patients with rheumatoid arthritis (RA) compared with general population comparators (GPCs) following introduction of biological DMARDs in 2002.
Changes in 5-year incidence rate of total knee replacement (TKR) among patients with incident rheumatoid arthritis (RA) following introduction of biological DMARDs (bDMARDs) and age, sex and municipality-matched general population comparators (GPCs)
Among GPCs, the incidence rate of TKR increased from 1996 to 2001 but less so from 2003 and onwards (table 3). This pattern was also observed in when applying quarterly derived data (online supplementary table S4).
Discussion
In this nationwide study, we set out to estimate the impact of the introduction of bDMARDs along with the publication of associated treatment guidelines on the 5-year incidence of THR and TKR among patients with incident RA compared with matched GPCs. We found that the incidence of TKR started to decrease among patients with RA following introduction of bDMARDs, whereas the incidence rate of THR had already started decreasing prior to bDMARD introduction. Incidence rates of THR and TKR among GPCs increased throughout the entire study but less so in the later years.
Our observed incidence rates and trends of THR and TKR among patients with RA are very similar to those observed among English and Welsh patients with RA.29 Using data from primary care in England and Wales, we found that introduction of TNFi and publication of NICE Technology Appraisal 36 concerning TNFi treatment in patients with RA was associated with a significant decline in rates of TKR, but not THR.29 By applying the same method on two different RA populations from different countries with different healthcare systems and reaching the same overall conclusion allows us to have greater confidence in our results. In patients with RA, knees are more often affected by synovitis than hips, and knee but not hip joints are routinely investigated in the widely used DAS28,30–34 which could be an explanation for an impact of bDMARD introduction on TKR but not THR. However, it can also be speculated that the changes observed for THR are due to the more aggressive treat-to-target and tight disease-control strategies with conventional synthetic DMARDs implemented in the mid-1990s, resulting in a gradual decline in the incidence of THR due to RA-related synovitis and erosions, followed by a continued decline due to less frequent occurrence of secondary osteoarthritis of the hip.
Surprisingly, we observed an increase in the incidence of THR among patients with RA in 2003. We have no clear explanation for this finding, but a change in government in late 2001 and a subsequent political focus on bringing down the waiting lists for elective surgeries offer a potential explanation. Another explanation could be that patients with RA were considered more fit for surgery due to improved treatment options. Unfortunately, we are not able to verify these theories. Interestingly, the same increase in level for THR was observed in an English and Welsh RA population.29 Hekmat et al investigated incidence rates in a regional RA population from Malmo, Sweden, and found that the incidence rate of THR had decreased from 1997 to 2007 in agreement with our findings. However, in that study, the incidence of TKR increased.9 Possible explanations for the different findings could be that the Swedish cohort included both incident and prevalent RA patients, and a less widespread use of TNFi at the time in south Sweden. Nikiphorou et al used two RA inception cohorts from UK to investigate changes in the use of major orthopaedic surgery from 1986 to 2011. Whereas intermediate and minor surgical interventions decreased during this period, there were no changes in use of major joint surgery.16 Studies from the USA have suggested a decline in joint surgery among patients with RA, but because of differences in healthcare access/systems, those results are more difficult to compare with ours.14 15
We decided to use biannually derived data for our primary analysis and quarterly data for the sensitivity analysis. At the time where this decision was made, there was no published guidance regarding the relative importance of number of time points in the pre-intervention and postintervention periods contra the number of individuals/outcomes occurring per time point. However, the results of a recent simulation study (unpublished) would suggest that given our large sample size, the use of quarterly derived data is the more appropriate in terms of providing greater statistical power. Indeed, while the overall findings did not change in sensitivity analyses using quarterly data, the results of the TKR analysis became statistical significant in patients with RA.
All patients and GPCs were followed up for the first 5 years following diagnosis, thus only allowing us to capture joint replacements performed within the first years after disease onset. Although this could underestimate the true long-term impact of bDMARDs on the outcomes, it allowed for all patients to have an equal amount of follow-up time regardless if they entered the study in the pre-bDMARD or the bDMARD era. Also, as observed in our study and a recent study by Nikiphorou et al, a non-negligible proportion of patients with RA go on to require joint replacement surgery within 5 years with the highest proportions among patients with moderate or severe disease activity.3 Thus, the 5-year incidence of joint replacement does not serve as a long-term outcome, but rather as a surrogate marker of the inflammatory burden suffered by the patient in the early years of the disease.
Our study has some important limitations. There is an inherent risk of misclassification of patients with RA using healthcare registers,35 but our extraction criteria are likely to have minimised this as we only included patients with RA diagnosed at an inpatient or outpatient facility specialised in rheumatology or general internal medicine according to the DNPR. Another important limitation is one inherent to all correlational studies. We acknowledge that our findings of decreased need for TKR among patients with RA could at least partly be due to increased use of treat-to-target strategies and more aggressive conventional synthetic DMARD combination therapy.36 Changes in diagnostic criteria for RA introduced in 2010 are not likely to have affected our results, but we cannot rule out that referral patterns of patients with RA to orthopaedic surgery have changed. Increased focus on and changes in non-treatment factors such as obesity along with changes in prevalence of certain comorbidities that would affect the use of or willingness to perform joint replacement surgery around the time of bDMARD introduction could theoretically also play a role in our findings. However, we found no changes in prevalence of comorbidities nor lifestyle-related diagnoses such as obesity and chronic obstructive pulmonary disease (online supplementary table S5), and no major changes were introduced to treatment guidelines except for those directly aimed at bDMARD treatment around the time of the intervention. To investigate the true impact of bDMARDs on the need for joint surgery, studies using individual-level based information on DMARD treatment are needed.
However, this study has also several strengths, including the nationwide population-based design with access to complete follow-up in a large sample of patients with RA and matched GPCs in a universal, tax-funded healthcare system. We compared our findings with trends among GPCs, thereby gaining insight into secular trends and enabling us to review our findings for the RA population in that context. The interrupted time-series analysis as choice of method is another strength. Had we not been able to identify the upward going/constant trend in incidence of TKR among patients with RA in the pre-bDMARD era but rather just compared the overall incidence rate in the two separate eras or used a survival analysis design comparing the risk of THR and TKR in each era, we would have concluded that the incidence rates and HRs of TKR were similar as the trends in the pre-bDMARD and the bDMARD era were equal but opposite.
In conclusion, we report that the incidence rate of THR and TKR was 3-fold and 14-fold higher, respectively among patients with RA compared with GPCs in 1996; that in patients with RA, but not in matched GPCs, introduction of bDMARDs was associated with a decreasing incidence rate of TKR, but not THR.
Acknowledgments
We wish to thank Christian Cato Holm at The Parker Institute for his invaluable help with data management.
References
Footnotes
Handling editor Josef S Smolen
Contributors RLC and LD had full access to all of the data in the study and take responsibility for the integrity of the data and the accuracy of the data analysis. RLC, DPA, LD, SH: study concept and design. RC and LD: acquisition of data. RC, SH, DPA: statistical analysis. All authors: interpretation of data; critical revision of the manuscript for important intellectual content. RLC: drafting of the manuscript. LD, AO, LEK, DPA and SO: study supervision.
Funding The study was funded by The Danish Rheumatism Association, The Bjarne Jensen Foundation, The Oak Foundation and The Danish Council for Independent Research. This work has been supported by the National Institute for Health Research (NIHR) Biomedical Research Centre, Oxford. DPA is funded by a National Institute for Health Research Clinician Scientist award (CS-2013-13-012). This paper presents independent research funded by the NIHR. The views expressed are those of the author(s) and not necessarily those of the NHS, the NIHR or the Department of Health.
Competing interests DPA’s research group has received research grants from Servier, UCB and Amgen; consultancy fees from UCB outside the present work. PH has received speaking fees from Celgene and UCB outside the present work. LEK has received fees for speaking and/or consultancy from Pfizer, AbbVie, Amgen, UCB, Celgene, BMS, Biogen, Sanofi, MSD, Novartis, Eli Lilly and Janssen Pharmaceuticals. LD has received speaking fees from MSD and UCB outside the present work.
Ethics approval Approval was given by the Danish Data Protection Agency (GEH-2014-043, I-Suite: 03166).
Provenance and peer review Not commissioned; externally peer reviewed.