Article Text

Abstract
Objectives To compare mortality risks in patients with rheumatoid arthritis-associated interstitial lung disease (RA-ILD) and patients with RA without ILD.
Design Matched cohort study.
Setting The study was conducted in Denmark, using nationwide, prospectively collected data.
Participants Among patients with RA diagnosed between 2004 and 2016, 679 patients with RA-ILD were matched for birth year, gender and age at RA diagnosis with 11 722 patients with RA but without ILD.
Main outcome measures Mortality risks were assessed using Kaplan-Meier mortality curves, and hazard rate ratios (HRRs) for death were estimated using Cox proportional hazards regression models.
Results The number of prevalent RA patients more than doubled from 15 352 to 35 362 individuals during the study period. RA-ILD was seen in 2.2% of incident RA patients. 34.0% of RA-ILD cases were diagnosed within 1 year prior to and 1 year after the RA diagnosis. One-year mortality was 13.9% (95% CI, 11.4% to 16.7%) in RA-ILD and 3.8% (95% CI, 3.5% to 4.2%) in non-ILD RA, 5-year mortality was 39.0% (34.4% to 43.5%) and 18.2% (17.3% to 19.1%) and 10-year mortality was 60.1% (52.9% to 66.5%) and 34.5% (32.8% to 36.1%), respectively. The HRRs for death were 2 to 10 times increased for RA-ILD compared with non-ILD RA, irrespective of follow-up period. Stratified analysis showed that the HRR for death was highest in the first months after the diagnosis of RA-ILD was made, especially in patients diagnosed with RA before diagnosis of ILD. HRR was higher in males and in patients without comorbidity as assessed by the Charlson Comorbidity Index.
Conclusions ILD is a serious complication in RA, with a significantly increased mortality compared with a large matched cohort of RA comparisons without ILD.
- Rheumatoid Arthritis
- Epidemiology
- Pulmonary Fibrosis
Statistics from Altmetric.com
Introduction
The mortality of patients with rheumatoid arthritis (RA) has declined over the past decade, and the decline appears greater than that in the general population.1–3 New treatment strategies for RA with early and effective intervention leading to reduced disease activity4 are the likely cause for this improvement. However, mortality is still increased in RA,1 and cardiovascular disease and interstitial lung disease (ILD) are the primary contributors to premature deaths.5 6
Subclinical interstitial lung abnormalities (ILAs) may be detected in 30%–50% of patients with RA,7 8 but the individual risk of progression to clinically significant ILD is not known. However, ILAs are associated with increased mortality.9 Clinically significant ILDs are seen in 5%–10% of patients with RA.10–13 Reported estimates vary considerably due to differences in disease definition and diagnostic methods. Known risk factors for RA-ILD are tobacco smoking, male gender and high anti-citrullinated protein antibody (ACPA) levels.10 In consecutive RA patients examined with high-resolution CT (HRCT), the prevalence of RA-ILD was 19%.14 One-third of these patients showed significant progression during a 2-year period, and the strongest predictor of progression was pre-existing pulmonary function impairment.15 The presence of usual interstitial pneumonia on HRCT has been associated with worse outcome than non-specific interstitial pneumonia.16–19 However, a recent study20 showed that pulmonary function, but not baseline HRCT pattern, independently predicted mortality after controlling for influential variables.
The reported median survival in previous RA-ILD studies ranges from 3 to 10 years.11 12 20
We designed the present study as an attempt to overcome the limitations of small RA-ILD cohorts, referral bias and changing management strategies over long study periods. We hypothesised that mortality in RA-ILD was increased compared with RA without ILD in a large population-based cohort of recent RA patients treated in accordance with current recommendations. The aim was to compare mortality among patients with RA-ILD with that in patients with RA without ILD and to investigate the impact of gender, age, seropositive RA and comorbidity on the risk of death in a matched cohort design.
Methods
Setting
We conducted the study in Denmark, in a population of 5.6 million persons at risk (2016), using prospectively collected data from population-based medical databases.
Data sources
The Danish National Patient Registry (DNPR)21 contains information about central person registry (CPR) number, dates of hospital admissions and discharges, diagnostic and surgical procedure codes and discharge diagnoses in all somatic hospitals in Denmark since 1977, and additionally, all outpatient hospital contacts and emergency department contacts since 1995. The International Classification of Diseases eighth edition (ICD-8) was used for discharge diagnoses coding until the end of 1993 and the ICD-10 codes thereafter. The DNPR was used as the source of information about all outpatient contacts and hospital admissions. Since the information is part of the reimbursement system for the hospitals, a high level of completeness is ensured.
The Danish Civil Registration System (CRS)22 contains information about date of birth, place of residence, vital status and migration into or out of Denmark since 1968. The CPR number assigned to all Danish residents is a unique 10-digit personal identifier, which goes through all Danish registries including the CRS, enabling individual level linkage across all different registries. The system ensures complete follow- up with respect to mortality.
The Danish National Database of Reimbursed Prescriptions23 includes data on all reimbursed prescriptions redeemed at Danish community pharmacies since 2004. The database contains no data on drugs dispensed during inpatient hospital stays and drugs dispensed directly to patients at hospital-based outpatient clinics.
Medication use for RA or RA-ILD were defined as reimbursement of at least two prescriptions for the same drug within 3 months before and 12 months after the index date. Data from 2004 until December 2015 were available.
The study was approved by the Danish Data Protection Agency (record number 1-16-02-277-16) and the Danish Health Data Authority.
Identification of patients with RA
We used the DNPR to identify all patients with a first-time diagnosis of RA as primary or secondary diagnosis during hospital admission or as outpatient contacts between 1 January 2004 and 1 July 2016. We used the ICD-10 codes M05 (seropositive RA) and M06 (other RA) for identification of RA. American College of Rheumatology (ACR) 1987 criteria24 were used for the diagnosis of RA until 2009 and the ACR/European League Against Rheumatism (EULAR) criteria from 2010.25 To ensure that only incident RA cases diagnosed after 2004 were included, we excluded all RA cases identified during the period 1977–2003 using ICD-10 codes from 1994 onward and ICD-8 codes before 1994 (712x RA and allied conditions).
Identification of RA patients with ILD (index cohort)
Information on primary and secondary ILD diagnoses was also obtained from the DNPR using all available hospital admission and outpatient contact information. ILD diagnoses prior to, synchronous with or after RA diagnosis were included. The ICD-10 codes used for the identification of ILD were J84 (other interstitial pulmonary diseases) and M05.1c (RA with pulmonary fibrosis). Screening for pulmonary involvement is not part of the follow-up programme for RA in Denmark, and HRCT scans are not performed systematically in asymptomatic patients. The index date was defined as the date when the patient had two diagnoses, RA and ILD, regardless of which one was assigned first.
We randomly selected matched comparisons with the same gender, year of birth and first time diagnosis of RA assigned ±1 year of the date of the RA diagnosis of the RA-ILD patients. The identification of the matched comparison cohort is described in detail in the online supplementary material.
Mortality
We obtained information on death from all causes from the CRS.22
Covariates
To obtain a complete hospitalisation history for the identified RA-ILD patients and matched RA comparisons without ILD, we used all inpatient and outpatient diagnoses recorded in the DNPR 5 years before the index date.
To measure comorbidity, we computed a Charlson Comorbidity Index (CCI) score26 for each patient using the ICD-10 diagnostic codes listed in the online supplementary table 2s. RA and ILD diagnoses were not included in the CCI. Based on the score, we defined three comorbidity categories: 0 (no comorbidity, applied to patients with no previous record of conditions included in the CCI), 1 to 2 (moderate) and 3+ (severe).
Assessment of seropositivity was based on ICD-10 codes of either seropositive or seronegative/other RA and not on results of serological testing, which was not available from the national registries.
Data analysis
We described the cohort of RA-ILD patients and matched RA comparisons without ILD according to age, gender, CCI score, presence of ischaemic heart disease, cardiac failure, and diabetes, tabulating the number and proportion of patients overall. Cumulative mortality for the two groups were compared using Kaplan-Meier mortality curves. All individuals were followed from the index date until death, emigration or 1 July 2016, whichever came first. We used Cox proportional hazards regression to estimate hazard rate ratios (HRRs) for death and corresponding 95% CIs. Taking the matching into account, we computed crude HRRs and HRRs adjusted for CCI score and RA seropositivity. We computed the mortality risk and HRR during the different follow-up periods from the index date: 0 to 30 days, 31 day to 6 months, >6 months to 1 year, >1 year to 5 years and >5 years to 10 years. We reported the number of patient who were at risk of death at the start of each follow-up period and the number of patients who died during the same follow-up period. The assumption of the proportional hazards was assessed graphically.
In order to study potential differences in the association between ILD and mortality in subgroups of patients, we stratified all analyses on gender, age groups and comorbidity for different follow-up periods calculating both crude HRRs and HRRs adjusted for comorbidity and seropositive RA.
Results
During the period 2004–2015, the incidence of RA remained stable, but a remarkable increase in the prevalence of RA was seen from 15 000 in 2004 to 35 000 individuals in 2016 (figure 1). A total of 31 333 incident RA patients diagnosed between 2004 and 2016 were included in the study. RA-ILD was seen in 679 (2.2%) of the incident RA patients. The distribution of gender, age and seropositivity of the entire RA cohort is shown in table 1. RA-ILD patients were older, more likely to be male and the frequency of seropositivity was higher.
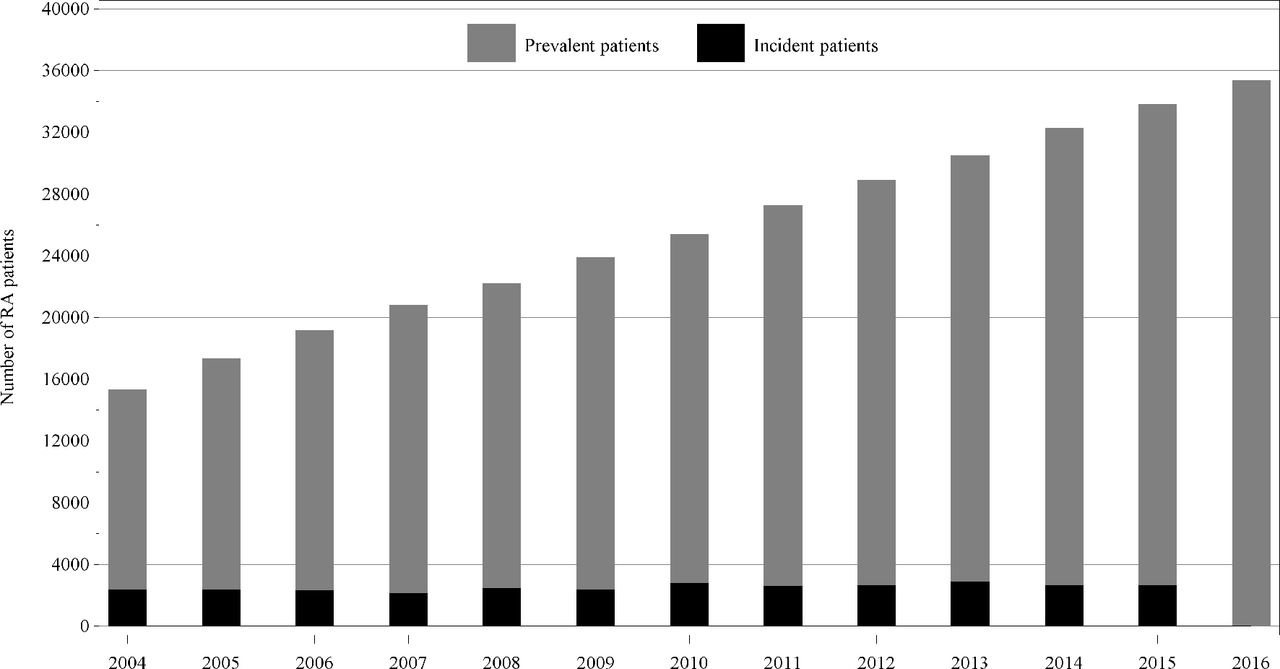
Incidence and prevalence of RA in Denmark from 2004 to 2016. RA, rheumatoid arthritis.
Characteristics of RA patients with and without ILD
The cohort of 679 RA-ILD patients was matched with a cohort of 11,722 RA patients without ILD. The demographics of the RA-ILD patients and the matched cohort of RA patients without ILD are presented in table 2. The distribution of the ICD-10 codes is listed in the online supplementary table 1s.
Characteristics of RA-ILD patients and matched comparisons
Fourteen per cent of ILD cases were diagnosed 1–5 years before RA. Thirty-four per cent were diagnosed within 1 year prior to the RA diagnosis, synchronous with the RA diagnosis, or within the first year after the RA diagnosis. Twenty-eight per cent were diagnosed 1 to 5 years after the RA diagnosis (see online supplementary table 3s).
The burden of comorbidity assessed by the Charlson Comorbidity Index was higher in the RA-ILD group (CCI ≥1 in 59.6% of RA-ILD patients and 38.0% of RA comparisons without ILD).
Individual comorbidity diagnoses of ischaemic heart disease, congestive heart failure and diabetes were also more frequent in the RA-ILD group, the difference being more pronounced for congestive heart failure (8.5% in the RA-ILD group and 4.4% in the non-ILD RA group). Table 3 shows the medication used for RA and RA-ILD based on reimbursed prescriptions in the first year after the RA diagnosis had been assigned. No data on hospital-dispensed medication were available.
Treatment based on at least two reimbursed prescriptions within 3 months before and 1 year after the index date
Cumulative mortality in RA-ILD patients and matched comparisons without ILD is shown in figure 2. One-year mortality was 13.9% (95% CI, 11.4% to 16.7%) in RA-ILD patients and 3.8% (95% CI 3.5% to 4.2%) in matched comparisons, 5-year mortality was 39.0% (34.4% to 43.5%) and 18.2% (17.3% to 19.1%) and 10-year mortality was 60.1% (52.9% to 66.5%) and 34.5% (32.8% to 36.1%), respectively.

{kind=link}
{kind=link}
Kaplan-Meier survival curves for RA with and without ILD. ILD, interstitial lung disease; RA, rheumatoid arthritis.
Median survival was 6.6 years in RA-ILD (95% CI 5.6 to 8.6 years). The median of survival was not reached in the matched RA cohort. The HRRs for death were increased for RA-ILD patients for all time periods during follow-up (table 4). Stratified analysis showed that HRR for death was higher in patients who were diagnosed with RA prior to ILD (see online supplementary table 4s).
HRR for risk of death among RA patients with ILD compared with matched RA cohort
The HRR for death within the first 30 days after the index date was 10.4 (95% CI 5.9% to 18.2%) in RA ILD patients (26 deaths in 679 patients) compared with matched comparisons (41 deaths in 11 722 patients). In stratified analyses, HRR for early death was even higher in males (HR 14.5, 95% CI (6.2% to 34.2%)) and higher in the age group 65 to 74 years. Seropositivity was not associated with differences in survival when compared with seronegativity/other RA. Assessment of the impact of the Charlson Comorbidity Index on risk of death in days 0–30 revealed that the HRR was 16.4 for CCI=0 and 10.0 for CCI=1–2, compared with 3.0 in the high comorbidity group (CCI=3+) (see online supplementary table 5s).
Discussion
In this population-based cohort study from 2004 to 2016, the all-cause mortality among patients with RA-ILD was significantly higher than in a comparison cohort of RA patients without ILD matched for birth year, gender and age at RA diagnosis. The prevalence of RA increased during the study period, although the incidence remained stable. The main explanation to the increasing prevalence is the marked increase in survival among RA patients over the last decade.1 This observation is in agreement with other recently published findings.27 28 The 2010 change in diagnostic criteria for RA may have identified more patients with early RA.25 29 However, the change did not affect the incidence of RA based on the DNPR data, and it is unlikely to have contributed to the increase in RA prevalence.
It is well established that smoking increases the risk of RA.30 The prevalence of smokers in the Danish population has been stable since 2009 after decades of decrease.31 If this smoking pattern can be generalised to the RA population, it may have contributed to the stability in the incidence of RA. It is not yet clear whether the systematic effort aimed at identifying and treating risk factors has prevented deaths from ischaemic heart disease in the RA population. The strategy used by rheumatologists in Denmark follows the EULAR recommendations.32 Furthermore, an ongoing study compares the effect of a targeted, intensified, multifactorial intervention with that of conventional treatment of modifiable risk factors for cardiovascular disease in patients with early RA.33
The high risk of death within 30 days of diagnosis, particularly among patients who had been diagnosed with ILD after or at RA diagnosis, may be due to acute exacerbations in previously undiagnosed ILD. Previous cohort studies have shown that acute exacerbation as the first manifestation of ILD is common.34 35 It is a serious complication in RA-ILD as well as in idiopathic ILD and has a very high mortality.36–38 Diagnostic delay and severe disease at the time of ILD diagnosis has been described for other ILDs,39 40 and may also contribute to the high initial mortality.
The difference in risk of death between RA-ILD and matched comparisons was especially high at short-term follow-up for RA-ILD patients with low CCI. RA-ILD patients with higher CCI and longer follow-up still have significant excess mortality compared with non-ILD RA patients, but the ‘mortality gap’ diminishes because of increasing mortality among the comparisons.
Stratified analysis based on the initial diagnosis of seropositive RA (M05), or other/seronegative RA (M06.0 and M06.9) showed no difference in mortality between the two groups. The frequency of seropositive RA may be under-reported in registry data. In RCT cohorts from Denmark,41 42 the percentage of seropositivity equals the findings in other countries, with approximately 60% seropositive RA. A possible explanation to this difference may be the fact that some patients are assigned the diagnosis of RA at the first contact to the public health service when serological data may not yet be available. Seroconversion during the cause of follow-up may also occur.
In Denmark, RA is diagnosed by specialists in rheumatology, and thus, the validity of the registry data is likely to be high. This is supported by previous findings of a high positive predictive value of DNPR diagnoses for conditions included in the CCI.43 In the same study, the positive predictive value of DNPR diagnoses of connective tissue disease, including RA, was 98%. A recent study of the Swedish National Patient Registry demonstrated a validity of the registry-based RA diagnoses of 90% for incident as well as prevalent RA.44 The majority of the remaining patients had other inflammatory rheumatic diseases. In the Nordic countries, hospital-based rheumatologists treat the majority of RA patients, and many similarities exist between healthcare systems. Therefore, the Swedish findings strongly support the validity of the RA diagnoses in the DNPR.
Future large studies are needed that include specific levels of IgM rheumatoid factor and anticyclic citrullinated peptide in the assessment of outcome in RA-ILD.
The frequency of ischaemic heart disease was only slightly higher in the RA-ILD group, and it is unlikely that this difference would account for the increased mortality. Other CCI groups, including cancer and lymphomas, showed an equal distribution between cases and comparisons. The main differences were seen in chronic pulmonary diseases, congestive heart failure, and connective tissue diseases. A previous study of patients with pulmonary fibrosis reported that almost half of the participants had been given an incorrect initial diagnosis of respiratory disease other than ILD.45 This may contribute to the differences seen in the frequency of chronic respiratory diseases.
Strengths and limitations
The strength of the present study is the large, population-based RA cohort with complete follow-up of all patients and the match of 95% of patients with RA-ILD with at least 10 comparisons. Because of the unbalance between the RA-ILD and RA non-ILD groups, we used a matched cohort design in order to cope better with confounding. We achieved a good balance between the RA-ILD group and the comparison group. Furthermore, the matched design provided exact start of follow-up for RA patients without ILD.
The limitations are the lack of information about radiological ILD pattern, lung function impairment, smoking history, level of autoantibodies, RA activity and full therapy history, which are not available from the medical registries. No validation studies of registry ILD diagnoses exist. Rare diagnoses like ILD are likely to have a high positive predictive value, but they are also likely to be under-reported or misclassified as other, more common respiratory diseases. We used broad diagnostic codes for ILD based on our experience that J848 (other ILD) and J849 (unspecified ILD) are often used for RA-ILD. We also included J841 (ILD with fibrosis) to ensure the inclusion of patients misclassified with a diagnosis of idiopathic ILD, for example, idiopathic pulmonary fibrosis. RA-ILD is likely to be underdiagnosed, and thus, our study may overestimate the true mortality, but this should only encourage the identification of symptomatic patients and earlier diagnosis of RA-ILD.
In conclusion, our study showed a significantly increased risk of death in patients with RA-ILD compared with matched RA comparisons without ILD, especially in the first month after the final diagnosis of RA and ILD was made. Mortality remained significantly increased throughout the course of the disease.
Generalisability and clinical implications
The generalisability of the findings is likely to be very high, since the study is population based and uses high-quality health registry data with complete follow-up of all patients. It is the largest cohort described to date and represents recently diagnosed RA patients managed in accordance with currently recommended treatment strategies. Furthermore, the Danish welfare system provides the same high level of healthcare to the whole population. The results can be generalised to other populations with similar genetic backgrounds, environmental exposures and lifestyles.
The findings of this study, as well as the absence of RCT-based evidence to guide therapy in patients with RA-ILD,46 emphasise the need of a close collaboration between rheumatologists and pulmonologists in the effort to improve the management of these patients.
References
Footnotes
Contributors CH, EB, OH and TE conceived the study idea and developed it in collaboration with ABP, SPU and AL. CH, ABP and SPU collected the data. CH, TE, EB, AL, AB, and OH reviewed the literature. ABP and SPU directed the initial analyses. These were developed further by the other coauthors and then carried out by ABP and SPU. CH, OH, ABP, SPU, AL, EB and TE participated in the discussion and interpretation of the results. CH organised the writing and wrote the initial draft. All authors critically revised the manuscript for intellectual content and approved the final version before submission. CH is the guarantor.
Funding The study was supported by a grant from The Danish Rheumatism Association and by the Program for Clinical Research Infrastructure (PROCRIN) established by the Lundbeck Foundation and the Novo Nordisk Foundation.
Competing interests None declared.
Patient consent Detail has been removed from this case description/these case descriptions to ensure anonymity. The editors and reviewers have seen the detailed information available and are satisfied that the information backs up the case the authors are making.
Ethics approval The study was approved by the Danish Data Protection Agency (record number 1-16-02-277-16). As this study did not involve contact with patients or an intervention, it was not necessary to obtain permission from the Danish scientific ethical committee.
Provenance and peer review Not commissioned; externally peer reviewed.