Article Text

Abstract
Background: Chronic systemic inflammation may contribute to accelerated atherosclerosis and increased arterial stiffness in patients with rheumatoid arthritis (RA). In addition to lowering cholesterol, statins have immunomodulatory effects which may be especially beneficial in patients with RA who have systemic immune activation.
Objective: To investigate the effect of atorvastatin on the augmentation index (AIx: a measure of arterial stiffness) and systemic inflammation in RA.
Methods: 29 patients with RA (mean (SD) age 55 (13) years) with moderately active disease of long duration were studied. AIx, lipid levels, serum inflammatory markers, and disease activity score were measured before and after 12 weeks of atorvastatin 20 mg daily.
Results: AIx improved significantly from 34.1 (11.6)% to 29.9 (11)% (p = 0.0002), with the greatest improvements in AIx occurring in those subjects with the highest disease activity scores (r = −0.5, p = 0.007). Total and LDL cholesterol were reduced from 5.5 (0.9) to 3.9 (0.7) mmol/l and 3.3 (0.8) to 1.9 (0.6) mmol/l, respectively (p = 0.0001). Serum inflammatory markers remained unchanged during the study.
Conclusions: Atorvastatin significantly reduced arterial stiffness in patients with RA. The greatest improvements were seen in patients with more active disease, suggesting that, in addition to the beneficial effects of cholesterol reduction, immune modulation may contribute to the cardioprotective effect of statins.
- AIx, augmentation index
- CRP, C reactive protein
- DAS28, 28 joint disease activity score
- ESR, erythrocyte sedimentation rate
- LDL, low density lipoprotein
- NNT, number needed to treat
- NO, nitric oxide
- PWA, pulse wave analysis
- RA, rheumatoid arthritis
- arterial stiffness
- atherosclerosis
- cardiovascular disease
- rheumatoid arthritis
- statins
Statistics from Altmetric.com
- AIx, augmentation index
- CRP, C reactive protein
- DAS28, 28 joint disease activity score
- ESR, erythrocyte sedimentation rate
- LDL, low density lipoprotein
- NNT, number needed to treat
- NO, nitric oxide
- PWA, pulse wave analysis
- RA, rheumatoid arthritis
Rheumatoid arthritis (RA) is associated with increased cardiovascular mortality and morbidity.1 Parallels between the inflammatory and immunological mechanisms operating in atherosclerotic plaque and rheumatoid synovitis have been highlighted,2 and atherosclerosis is widely considered to be an inflammatory disease. It may be that chronic systemic inflammation in RA contributes to excess cardiovascular disease in this population either by potentiating and/or accelerating atherosclerosis1 or by other mechanisms such as diffuse subclinical vasculitis.3 Arterial stiffness is a marker of vascular dysfunction and an independent risk factor for cardiovascular disease.4 We have previously shown that subjects with RA free from cardiovascular risk factors have increased arterial stiffness compared with healthy controls matched for age and sex,5 suggesting that arterial stiffness may be a useful marker of early vascular dysfunction in RA.
HMG-CoA reductase inhibitors (statins) have demonstrated benefit in the primary and secondary prevention of cardiovascular disease.6–8 The protective effect of statins appears to be greater than can be explained by their cholesterol lowering activity9 and the benefit of statins appear to be even greater in the presence of higher C reactive protein (CRP) levels.10,11 Statins are known to have a number of immunomodulatory effects which may affect vascular function, plaque stability, and thrombosis.12 These immunomodulatory effects of statins may be especially important in patients with RA who have systemic immune activation. Statins have been demonstrated to reduce disease activity and inflammatory responses in a murine model of inflammatory arthritis and in patients with RA.13,14 The present study aimed at evaluating the effect of atorvastatin on arterial stiffness in patients with RA. Systemic markers of inflammation and disease activity were also assessed.
PATIENTS AND METHODS
Patients
Twenty nine subjects (9 male, 20 female) with RA according to criteria of the American College of Rheumatology15 were recruited from the Royal Melbourne Hospital Rheumatology clinic. Exclusion criteria were age <18 years, current treatment with lipid lowering drugs, contraindication to statins, renal or liver failure, pregnancy, and cancer. The study was approved by the institutional ethics committee and written informed consent was obtained from all subjects.
Study protocol
Subjects took atorvastatin 20 mg daily for 12 weeks and attended for assessment on three occasions: week 0 (before starting atorvastatin), week 6, and week 12. Arterial stiffness was measured at each visit by pulse wave analysis (PWA) as described below. Fasting venous blood was drawn after PWA for measurement of erythrocyte sedimentation rate (ESR), CRP, lipid levels (total, high density lipoprotein, low density lipoprotein (LDL) cholesterol, and triglycerides), liver function, and creatine kinase. Disease activity was measured with the 28 joint disease activity score (DAS28), a validated composite score incorporating tender and swollen joint count, ESR, and a patient global assessment of disease activity (100 mm visual analogue scale).16 A DAS28 ⩽1.6 indicates remission, whereas a value ⩾4.3 suggests active disease.16
Pulse wave analysis
PWA was performed using the SphygmoCor apparatus (Atcor Medical, Sydney, Australia) by a single trained investigator (SV) using the standard technique.17 Subjects attended in the morning after an overnight fast. Blood pressure was recorded in the supine position after several minutes of rest. Radial artery waveforms were recorded from the wrist of the dominant arm using a high fidelity tonometer (Millar SPT-301, Millar Instruments, Houston, Texas). Data were collected directly into a portable computer and when 20 sequential waveforms were acquired the integral software generated an averaged peripheral and corresponding central waveform using a validated transfer function.17 An augmentation index (AIx), a measure of systemic arterial stiffness, was calculated by the integral software as the difference between the second and first systolic peaks, expressed as a percentage of the pulse pressure. The mean of three measurements of the AIx was used in data analysis.
Reproducibility of same-day measurement of AIx as performed by SV was evaluated in 29 people (not the study subjects) before the start of the present study. The mean (SD) AIx for this group was 23.7 (12.5)% and the within observer difference (mean (SD)) was 1.1 (3.0)%. The correlation coefficient between the two AIx measurements was 0.97. These results compare favourably with data reported by other investigators. Wilkinson et al evaluated the same-day reproducibility of AIx in 33 subjects.17 The mean AIx for the study group was 19.6 (12)% and the within observer difference (mean (SD)) was 0.49 (5.4)%. In a reproducibility study of AIx in 100 healthy subjects by Rietzschel et al the correlation coefficient between first and second measurements of AIx was 0.95.18
Statistics
Results are expressed as mean (SD) unless otherwise indicated. Differences in variables before and after atorvastatin treatment were examined by the two tailed, paired t test. Correlation between AIx and reported variables was calculated using regression analysis. Statistical significance was inferred at p<0.05.
RESULTS
Table 1 shows the baseline demographic and clinical characteristics of the subjects with RA. All subjects enrolled in the study attended for the week 6 visit. Three subjects discontinued the study drug between weeks 6 and 12 and did not provide week 12 data. The reasons for withdrawal were rash, a flare of RA requiring high dose prednisolone, and an elective total hip replacement. For these subjects week 6 data were used in the final analysis; however, analysis of the data excluding these three subjects did not alter the findings. Table 2 summarises the results obtained.
Demographic details of the 29 patients with RA*
Results at baseline, week 6, and week 12 of atorvastatin treatment*
Lipids, inflammatory markers, and clinical parameters
As expected, total and LDL cholesterol were reduced from 5.5 (0.9) to 3.8 (0.6) mmol/l and 3.3 (0.8) to 1.8 (0.5) mmol/l, respectively, after 6 weeks of atorvastatin (p = 0.0001) and remained essentially unchanged at week 12. No changes in pulse rate, blood pressure, ESR, CRP, or DAS28 were seen during the study.
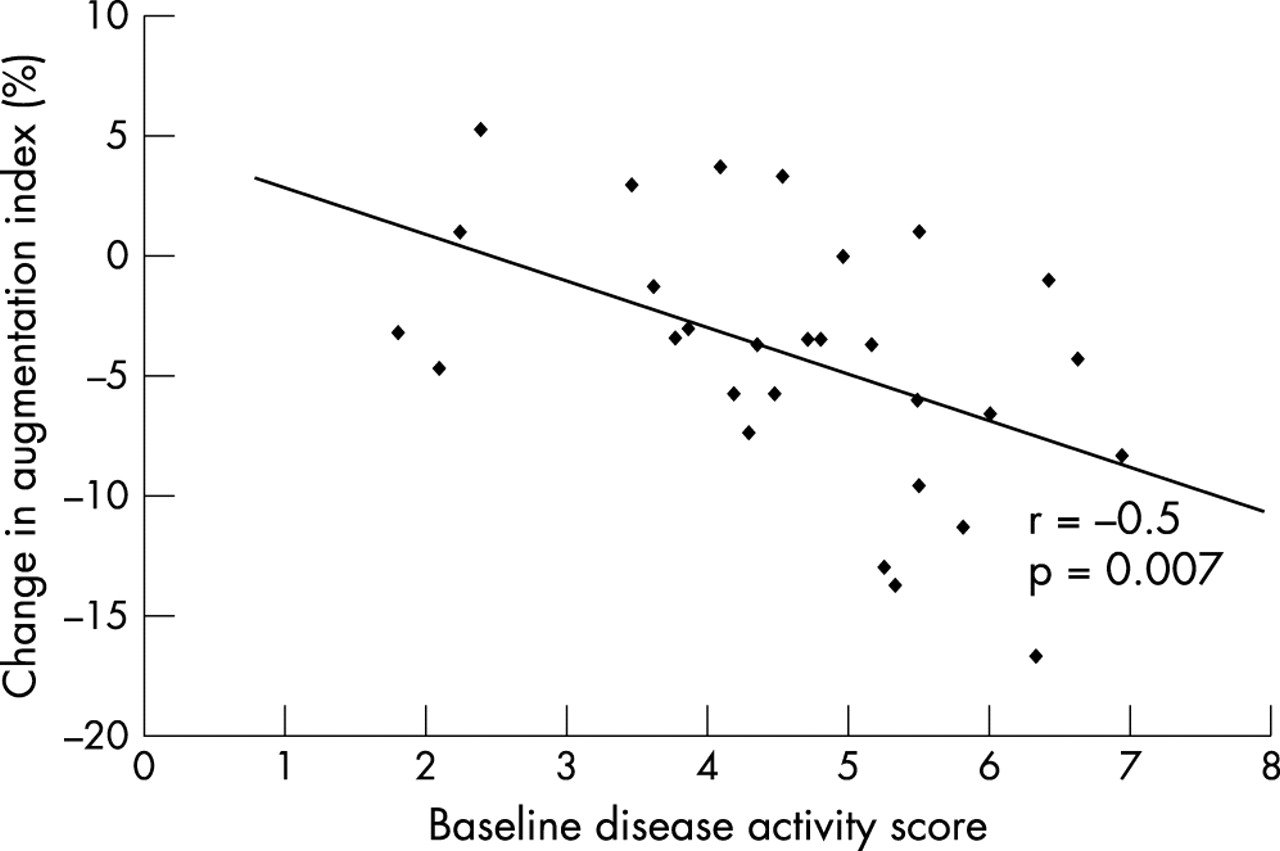
After 6 weeks of atorvastatin the AIx improved significantly from 34.1 (11.6) to 30.6 (11)% (p = 0.0002). A further minor improvement in AIx was seen at week 12 (AIx 29.9 (11)%; p = 0.0002 for comparison with baseline). Expressed as a percentage change from baseline, this is equivalent to a 12% reduction in arterial stiffness after 12 weeks of atorvastatin treatment. There was a significant correlation between the change in AIx and the baseline DAS28, with the greatest reductions in AIx occurring in those subjects with the highest DAS28 (r = −0.5, p = 0.007; fig 1). There was no correlation between the change in AIx and other baseline variables or changes in lipid levels or DAS28.

{kind=link}
Relationship between baseline DAS28 and change in AIx with atorvastatin.
Arterial stiffness
At baseline there were significant correlations between AIx and age, pulse rate and height, which are known determinants of arterial stiffness (table 3). No relationship was demonstrated between baseline AIx and blood pressure, ESR, CRP, lipid levels, or DAS28.
Multiple regression analysis for determinants of baseline AIx
DISCUSSION
This is the first study to examine the effect of statin treatment on arterial stiffness in RA. We found that 6 weeks of atorvastatin treatment significantly reduced arterial stiffness in these patients with RA. Arterial stiffness is a marker of vascular dysfunction and is an independent risk factor for cardiovascular disease.4 Increased arterial stiffness has been demonstrated in association with vascular risk factors such as smoking, hypertension, hypercholesterolaemia, and diabetes,19–22 has been correlated with the presence of atherosclerosis,23 and has been shown to predict cardiovascular events and mortality in hypertensive subjects.24–26 Arterial stiffness therefore appears to be a promising surrogate marker of cardiovascular disease in patients with RA.
The determinants of arterial stiffness are not fully understood, but may include structural and functional components. The endothelium, elastin, and collagen fibres within the intimal medial layers and arterial wall smooth muscle cells all contribute to arterial stiffness.27 Greater proportions of collagen as occur in more peripheral arteries, or degeneration of elastin fibres as occurs with age, result in increased arterial stiffness.28 Hypertrophy of smooth muscle cells or increased smooth muscle tone, or both, increases arterial stiffness.27,29 The endothelium, mainly through production of nitric oxide (NO), exerts an important functional influence on arterial stiffness. A number of investigators have demonstrated that inhibition of NO synthesis, by infusion of N(G)-nitro-l-arginine methyl ester (l-NAME) or l-N(G)-monomethyl arginine (l-NMMA), increases arterial stiffness in healthy volunteers.30–32 These data indicate that arterial stiffness is influenced, in part at least, by NO bioavailability and therefore that arterial stiffness reflects both the structural composition of the artery wall and endothelial cell function. Heart rate and blood pressure are also known determinants of arterial stiffness and, importantly, these remained stable throughout the study.
The relatively rapid reduction of arterial stiffness in these patients with RA suggests that improved endothelial function, as a result of lower serum cholesterol levels, may be the predominant mechanism. Reduction of serum cholesterol by a single LDL apheresis rapidly improves endothelial function,33 and improved endothelial function was seen as early as 1 month with simvastatin treatment.34 However, statins also act directly to improve endothelial function by increasing endothelial NO synthase expression and activity35–38 and inhibiting endothelin-1 production.39 In an earlier study we found no evidence of endothelial dysfunction (as measured by flow mediated dilatation) in patients with RA who had relatively late and well controlled disease and were free from traditional cardiovascular risk factors.5 In contrast, other investigators have demonstrated endothelial dysfunction in patients with early, untreated RA.40,41 In an uncontrolled study, treatment of 11 patients with RA with active disease with infliximab significantly improved endothelial function.42 Taken together, the results of these studies suggest that patients with RA with untreated or very active disease may have impaired endothelial function, which can improve with effective disease control.
Structural changes within the vessel wall can occur early in statin treatment and may also have contributed to the observed reduction of arterial stiffness in our study. In experimental models of atherosclerosis, reductions in atheroma size, lipid content, and macrophage numbers have been found after 8 weeks of statin treatment.43,44 Statins also have a number of immunomodulatory effects on vascular wall cells which may modify the progression of atherosclerosis or arteriosclerosis, or both, and thereby affect arterial stiffness. These include inhibition of macrophage recruitment and LDL accumulation,45,46 smooth muscle cell migration and proliferation,36,47–49 matrix metalloproteinase expression and secretion,46,50–52 monocyte and endothelial cell adhesion molecule expression, and local production of proinflammatory cytokines.53–55 The role of these effects in protecting against cardiac events and reducing arterial stiffness remains unknown, but may be especially important in patients with RA who have systemic immune activation and may also have subclinical vasculitis.3
We demonstrated a 12% reduction in mean arterial stiffness in patients with RA after 12 weeks of atorvastatin treatment, a result that is comparable to improvements reported by other investigators. In a group of 36 hypercholesterolaemic patients, 2 years of treatment with atorvastatin 20 mg/day reduced aortic stiffness by 14%, as measured by transthoracic echocardiography.56 Treatment of 22 patients with isolated systolic hypertension and normal cholesterol levels with 80 mg daily of atorvastatin improved systemic arterial compliance by 24%, as measured by carotid applanation tonometry and Doppler velocimetry of the ascending aorta.57 Six months of fluvastatin treatment (20 mg/day) in 22 patients undergoing haemodialysis with type 2 diabetes mellitus and normal serum lipid levels reduced pulse wave velocity from 1991 (162) to 1709 (134) cm/s (a 14% reduction).58 These studies differ in their patient population, type and dose of statin, and method of measuring arterial stiffness, but do provide consistent evidence that statins reduce arterial stiffness. Whether this reduction in arterial stiffness translates into improved long term clinical outcomes has yet to be demonstrated. However, measurement of AIx in a number of large, prospective cohort studies is currently underway and will provide valuable prognostic data.59
The greatest reductions in AIx were seen in those patients with RA with the highest disease activity scores. Other investigators have also reported greater clinical benefit from statins in the presence of inflammation.10,11 In the Cholesterol and Recurrent Events (CARE) trial of secondary prevention, the proportion of recurrent coronary events prevented by pravastatin was 54% for those with increased CRP levels as compared with 25% for those with low CRP levels.10 In the AFCAPS/TexCAPS primary prevention trial the efficacy of lovastatin in subjects with low LDL levels but increased CRP levels was similar to that seen in subjects with high LDL levels (numbers needed to treat (NNT) for 5 years to prevent one event were 43 and 47, respectively).11 In subjects with low LDL and low CRP, however, lovastatin was ineffective (NNT = 983).11 These intriguing data suggest that the immunomodulatory effects of statins may be an important component of their cardioprotective properties, especially in subjects with relatively normal cholesterol levels. Statins are known to reduce serum CRP levels60,61 and this may be one mechanism of the beneficial effect. In our group of patients with RA, however, treatment with atorvastatin did not reduce CRP levels. This may relate to relatively high disease activity and baseline CRP levels in our patients despite concurrent treatment with anti-inflammatory and immunosuppressant drugs or inadequate numbers, or both.
This study was designed as an exploratory pilot project. Although the reduction in arterial stiffness was clear and similar in magnitude to findings reported by other groups, our data now need to be confirmed in a randomised, placebo controlled study. The primary outcome measure in this study was arterial stiffness and thus the study was not powered to detect changes in serum markers or clinical measures of inflammation as a result of atorvastatin treatment. Greater numbers, longer treatment duration, and/or higher statin doses will be required to evaluate this possibility fully. Our findings provide a strong rationale for such a study.
CONCLUSIONS
Cardiovascular disease is a major cause of mortality and morbidity in RA. The present study provides important new evidence that atorvastatin improves arterial stiffness in patients with RA and that the vascular benefit of atorvastatin is greater in those patients with more active disease. It has recently been shown that statin treatment significantly reduces the incidence of major coronary events in diabetic subjects even in the absence of increased cholesterol levels, and statin treatment has been recommended in this patient group.8 Likewise, statin treatment may be advisable in patients with RA (and indeed other patients with chronic systemic inflammation) even in the absence of hyperlipidaemia. Whether the observed reduction in arterial stiffness with statins translates into improved cardiovascular outcomes for patients with RA requires further study.
Acknowledgments
Supported by the National Health and Medical Research Council and Pfizer Australia.