Article Text

Abstract
Objective To assess the costs and benefits of a partnership between health services, police and local government shown to reduce violence-related injury.
Methods Benefit-cost analysis.
Results Anonymised information sharing and use led to a reduction in wounding recorded by the police that reduced the economic and social costs of violence by £6.9 million in 2007 compared with the costs the intervention city, Cardiff UK, would have experienced in the absence of the programme. This includes a gross cost reduction of £1.25 million to the health service and £1.62 million to the criminal justice system in 2007. By contrast, the costs associated with the programme were modest: setup costs of software modifications and prevention strategies were £107 769, while the annual operating costs of the system were estimated as £210 433 (2003 UK pound). The cumulative social benefit-cost ratio of the programme from 2003 to 2007 was £82 in benefits for each pound spent on the programme, including a benefit-cost ratio of 14.80 for the health service and 19.1 for the criminal justice system. Each of these benefit-cost ratios is above 1 across a wide range of sensitivity analyses.
Conclusions An effective information-sharing partnership between health services, police and local government in Cardiff, UK, led to substantial cost savings for the health service and the criminal justice system compared with 14 other cities in England and Wales designated as similar by the UK government where this intervention was not implemented.
Statistics from Altmetric.com
Introduction
Violence imposes a substantial cost on health services, criminal justice systems and society at large. In 2003/2004, the cost of violence recorded by the police in England and Wales was an estimated £14 billion, which includes costs to health services, criminal justice system and physical and psychological impact on victims.1 Interventions that reduce violence could yield substantial reductions in these costs. Although there are few effective violence prevention interventions available at the community level, one such intervention is the Cardiff Violence Prevention Programme (CVPP), a unique anonymised information-sharing arrangement in a partnership between the hospital emergency department (ED), police and local government. This programme is based on the sharing and use of anonymised information about violent incidents that is captured electronically in the ED by reception staff.2 The data collected include location (name of bar, nightclub, school, park, precise street location, etc), time, day and weapon type. This information is stripped of personal identifiers and shared by hospital information technology (IT) personnel with the partnership crime analyst who combines data with police intelligence to generate regularly updated maps of violence ‘hotspots’ and summaries of weapon use and violence type (classified as ‘stranger’, ‘acquaintance’ and ‘domestic’ to fit with national crime survey categorisation). Integrated violence prevention is then based on this combined, continuously updated information rather than, as in comparison cities, only on police intelligence.
The partnership (now the statutory UK approach to crime prevention) met approximately every 6 weeks and, based on the combined data, introduced and sustained a range of strategies designed to address specific risks and patterns observed in the data. These strategies comprised repeated adjustments to the routes of police patrols and moving police resources from suburbs to the city centre at weekends to ensure that police were present and able to intervene at specific locations and times identified by the data, targeting problematic licensed premises (by police and city government officials responsible for alcohol licensing), and informing public space closed circuit television (CCTV) deployment. The CVPP data and partnership also contributed to other prevention strategies not directly related to policing, including pedestrianising sections of a city centre street at weekends where bars and nightclubs are mainly concentrated, enhanced alcohol licensing regulations, which included mandatory use of plastic barware in selected licensed premises, and, for a short time, more frequent late-night public transport services at weekends. There were no other major changes in law enforcement or emergency or trauma services in the intervention city during the study period, throughout which the city was served by the same, single ED.3
This model has recently been evaluated in an experimental study and time series analysis that demonstrated a 42% reduction in hospital admissions relative to comparison cities, a 32% comparative reduction in woundings recorded by the police and a 38% comparative increase in violence not causing injury (‘common assaults’).3 While the CVPP was found to reduce woundings, the programme imposed costs to the health service and criminal justice systems in terms of staff time and other resources. Given the limited resources available to both these public services, it is important to examine whether the CVPP produced sufficient benefit to each service, and to society at large, to justify the expenditure of these additional resources. In order to address this question, the study reported here sets out the monetary costs and benefits of this partnership from the perspective of the National Health Service (NHS), the criminal justice system and society.
Methods
Effectiveness study
The effectiveness study used monthly data on serious (woundings) and minor (common assaults) violence recorded by the police from January 2001 to April 2007.3 The intervention took place in Cardiff, Wales. The comparison cities in the evaluation were identified from a Home Office list of ‘most similar cities’ selected using a cluster analysis based on demographic, economic and social characteristics associated with crime rates.3 The effect of the CVPP was measured by estimating a negative binomial regression model with controls for each city's unemployment rate and police force strength, the calendar month and year and a separate intercept for each city to control for remaining unobservable differences between the cities. Regression models were estimated for both recorded serious and minor violence, and effects were estimated for each year after implementation. These patterns of effects (table 1) demonstrate two important consequences of the intervention. First, the impact of the programme increased over time; second, the programme was associated with a substantial reduction in serious violence, but an increase in minor violence (ie, violence not resulting in injury) recorded by the police.
Adjusted incidence rate ratio (AIRR) estimates of Cardiff Violence Prevention Programme (CVPP) effects and predicted change in annual number of assaults
For the purposes of this economic evaluation, it was necessary to convert these effects into the predicted change in the number of cases. This was done by multiplying the adjusted incidence rate ratio by the baseline mean number of common and wounding assaults in Cardiff in the 2 years before the CVPP was implemented.3 Since all costs and benefits of the CVPP are calculated on an annual basis, the monthly numbers were multiplied by 12. The estimated impact of the CVPP was an annual reduction in woundings ranging from 352 in 2003 to 849 in 2007, but an annual increase in common assaults ranging from 528 in 2003 to 295 in 2007. It has been suggested that the increase in recorded common assaults was a systematic consequence of the intervention facilitating earlier police intervention in violence, thereby reducing the severity of many assaults while increasing the extent to which minor violence was ascertained by police.3 The net impact of changes in serious and minor violence was valued in monetary terms and comprised impact on the NHS, the criminal justice system and wider societal impact (physical and psychological impact on victims and victim services).
The economic impact of violence
The unit costs of woundings and common assaults, based on a Home Office report,1 are reproduced in table 2. This report provides the ‘unit costs’ of woundings and common assaults. Because violence, unlike unintentional injury, results in costs to the criminal justice system as well as health services, estimates of specific costs are provided separately. The full programme cost was used to calculate the benefit-cost ratio for each service, in part, to make the most conservative estimate of the benefit-cost ratio, but also because the share of programme cost between health service and criminal justice systems could change when the programme is replicated in other settings.
Estimates of the unit cost of violence in England and Wales, 2003 UK pounds*
Given the evolving nature of the programme impacts over time, the benefits and costs were estimated on an annual basis. All monetary units were adjusted for inflation.4 For the overall costs and benefits, all monetary values are discounted to 2003 UK pounds using the 3.5% discount rate.5
Physical, psychological and health service costs
In the Home Office study,1 physical health impacts of non-lethal violent crime were measured based on responses to the authoritative, annual British Crime Survey (BCS). The BCS relies on responses from a representative sample of approximately 45 000 adults in England and Wales about their experience of crime in the last 12 months. Respondents are asked in detail about any injuries they suffered as a result of violence.
The psychological impact of violence was derived from a variety of studies of these outcomes.6 ,7 The duration of both physical and psychological outcomes was derived from the findings of the Global Burden of Disease study,6 which provides estimates of the prevalence of various health states. With reference to published unit costs of health and social care and the NHS cost manual for surgical and other procedures, these estimates were translated into health service costs associated with a defined range of health states resulting from UK violence.1
The costs associated with reductions in physical and psychological well-being were estimated by calculating the reduction in quality adjusted life years (QALY) lost for the harm sustained in woundings and common assaults8 and using a monetary QALY value to assign a value in UK pounds (£80 620; 2003 UK pounds). The duration and disability weights for all reported injuries were derived from the Global Burden of Disease study.6 Longer-term impacts of wounding were weighted using the EQ5D health state index.9 Once a reduction in the number of QALYs was calculated, it was then multiplied by the monetised value of a QALY to produce the cost estimate.10 The Home Office study also estimated costs due to time lost at work. However, since it is unclear if these costs are also accounted for in the QALY-related costs, these were excluded to avoid potential double counting.
Criminal justice costs
Criminal justice costs included police, court, probation and prison costs associated with responses to each type of violence. The Home Office study1 includes information for all police forces in England and Wales comprising estimates of the total amount of police time allocated to crime and non-crime-related activities. The proportion of police time allocated to crime-related activity was then applied to the overall police budget to give the total costs of crime-related police activity. The unit cost was calculated by dividing this number by the number of crimes of each type. Other crime and justice service costs were estimated using sentencing data on average length of sentences by crime type. The unit costs of sentences were estimated from various Home Office sources, and the total cost of sentences was calculated by multiplying the unit costs by the total number of persons sentenced. The cost per crime was then calculated by dividing total spending by the estimated number of crimes.
Programme costs
All resource inputs for the development, implementation and continued operation of the CVPP were included as programme costs. These costs included: staff salary and labour time for health service,11 police12 and local government staff. Wherever possible, overhead costs and non-monetary staff benefits were included. When overhead costs were not available, these were estimated at 47% (matching the overhead rate for a police chief inspector). Development of the hospital (ED) information technology to support information sharing required software adjustments to incorporate additional questions (see effectiveness study for details).3 In addition to the costs of the development and operation of the CVPP, costs were also included for the implementation and operation of all prevention strategies applied as a result of CVPP recommendations. The resources used were identified by performing a review of the CVPP meeting's minutes from the period of the study.
Results
Programme costs
Software programming, testing and refinement required 148 h of hospital information technology staff time and 15 h of review by IT management staff. Three hours of IT staff time were required to produce software that compiled and anonymised data for the monthly reports shared with key partners. Total software set-up costs were £1929 (table 3).
Unit and total costs of Cardiff Violence Prevention Programme (CVPP) implementation and operation
Other health service costs reflected additional staff time involved in collecting the data. Collecting the violence data took an average of 2 min per patient. In 2006, there was an average of 51 violence-related ED attendances in Cardiff per week (102 min per week: 7.3 h per month). This time was valued at the hourly rate for receptionists. Once the data had been collected in the (existing) Patient Management System, information staff collated, formatted, anonymised and emailed the resulting datasets to the programme partners. These tasks occupied approximately 32 h per year.
While the programme required no changes to police personnel levels, additional time was required for a police analyst to produce weekly and quarterly reports; additionally, multiple police personnel attended CVPP meetings and assisted in developing partnership recommendations. The annual time commitment for these personnel are reported in table 3. A maxillofacial surgeon contributed 104 h per year to lead and sustain the programme; this entailed chairing partnership meetings, managing the information-sharing process, and advocating violence prevention from a health perspective, based on information derived from the ED and from police intelligence. One further health professional, an ED consultant, attended CVPP meetings. Personnel from other social services also participated in the partnership, including an alcohol establishment licensing officer, a victim support manager and a night-time economy coordinator. The annual time commitment for these various personnel is reported in table 3.
Over the course of the partnership, several recommendations for strategies to reduce violence in the city's main entertainment district were developed. At the outset of the partnership in 2003, data from the ED was used to inform the location of four additional CCTV cameras to the existing city centre CCTV network. The costs for these four additional cameras, including initial capital costs for purchase and installation, as well as maintenance and monitoring costs, were derived from a Home Office report that estimated the costs and benefits of CCTV for crime prevention.13 These costs are reported in table 3. For the purposes of the benefit-costs analysis below, these costs were amortised across the years of the study (2003–2007).
A second recommendation by the partnership was to pedestrianise the street through the main entertainment district on weekend nights. This involved purchasing removable barriers and signage and having personnel (council workers in table 3) set up and dismantle the barriers around weekend evenings. The recommendation was implemented in January 2004 and continued for the duration of the study period.
The CVPP recommended that all establishments open until 4:00 use plastic barware after 23:00. Starting in 2005, these 20 establishments were required to stock half their barware inventory as polycarbonate ‘glasses’. The costs for this requirement were estimated using the difference in the per-unit costs of polycarbonate barware and traditional glass barware. Costs were obtained from a member of the Cardiff Licensees Forum. It was estimated that each required establishment would carry an inventory of 300 such plastic glasses, and that the inventory was replaced on an annual basis. The costs for this additional barware are reported in table 3.
Finally, the CVPP also recommended that the local transit service extend bus operating schedules six services per weekend. This recommendation was implemented in 2003, but was discontinued after 2 years due to underuse. It was not possible to estimate the costs of the extended bus schedule. This shortcoming of the costing of the partnership will be addressed in the sensitivity analysis.
Programme benefits
Estimates of total programme benefits are presented in table 4. Despite an increase in common assaults, the decrease in the more costly woundings after 2003 resulted in net benefits. Furthermore, the benefits grew substantially after 2003, exceeding £5 million per year until 2007, when the annual benefits exceeded £6 million. The discounted value of the total societal benefits was over £23 million.
Calculation of total benefits, programme costs, net benefits and benefit-cost ratios, by year and total
Benefit-cost ratio
While the benefits generated by the reduction in woundings were very large, the cost of the programme was modest. In the initial year, when the effect on wounding was lowest and cost of the programme was highest, the total benefit-cost ratio was 44. In subsequent years when the programme had larger impacts on wounding, the benefit-cost ratios were larger (range 76–98). When the discounted value of benefits and costs over the course of the experiment were considered, the overall total benefit-cost ratio was 82.
There were also large benefit-cost ratios from the perspective of the health and criminal justice services, individually. For both services, the programme produced benefits that exceeded programme costs in all years after implementation. Over the course of the study period, the health service benefit-cost ratio was 14.8 and the criminal justice system benefit-cost ratio was 19.1.
Sensitivity analysis
The results presented above are subject to several potential sources of variability that were examined by calculating a ‘pessimistic case’ for the programme effects, where the increase in common assaults was set at the upper end, and the decrease in woundings was set at the lower end of the 95% CIs (table 1). The programme benefits and benefit-cost ratios were then recalculated with this larger increase in common assaults and lower decrease in woundings. For example, given this ‘pessimistic case’, in 2003 the increase in common assaults was 906.10, and the decrease in woundings was 101.11. The estimated benefits and benefit-cost ratios in this case are given in table 5. Overall, the programme benefits in the pessimistic case were slightly more than half the benefits estimated at the point estimate of the programme effects. The overall total and criminal justice benefits were negative in 2003, but the health service benefits remained positive. From all three perspectives, the net annual benefits after 2003 remained positive and the benefit-cost ratios were well above 1. The cumulative benefit-cost ratios also remained well above 1, and the programme was cost saving from the perspective of both health and criminal justice services, even with this pessimistic estimate of programme effects.
Calculation of 'pessimistic case’ total benefits, programme costs, net benefits and benefit-cost ratios, by year and total
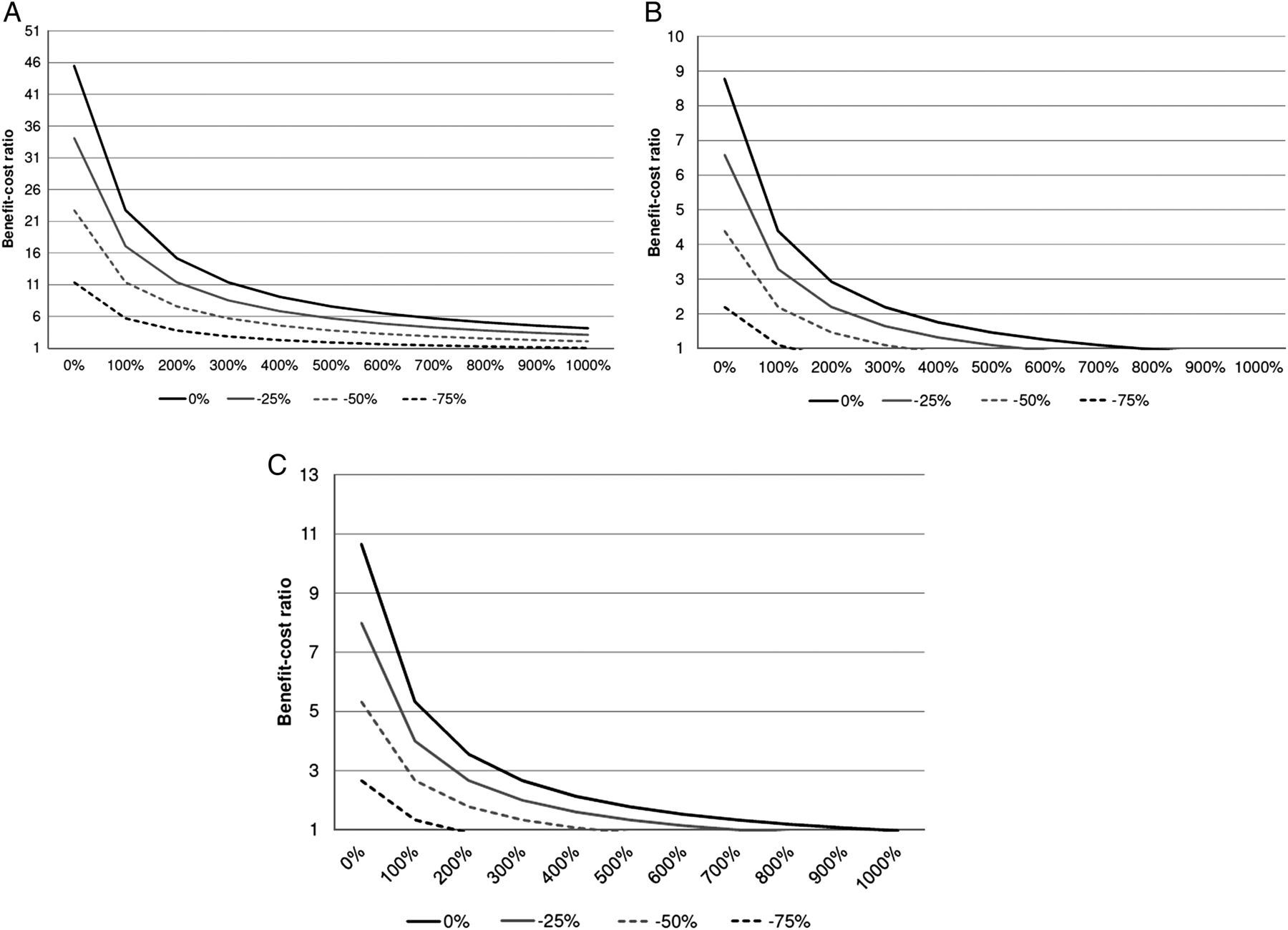
Benefit and cost variability is also likely with regard to the cost of crime and the costs of the programme. The costs of crime used here were derived from a complex set of estimates. The costs of the programme were calculated by members of the study team, but costs for the extended transit service hours were not available and other costs may have been missed. Also, the types and costs of prevention strategies could vary substantially in other settings. In order to address both these sources of variability succinctly, a set of two-way sensitivity analyses was conducted. Benefit-cost ratios were recalculated assuming a reduction in programme benefits of 25%, 50% and 75%, and an increase in programme costs of 100–1000%. The resulting benefit-cost ratios were then plotted against the increase in programme costs for each reduction in programme benefits. This sensitivity analysis was conducted using the pessimistic estimate of programme benefits to demonstrate the further reduction of benefits or increase in costs that would be necessary for the benefit-cost ratios to fall below 1.
The results from the two-way sensitivity analysis for the pessimistic case are illustrated in figure 1A–C. These results present the strongest challenge to the conclusion that the benefits exceed programme costs because they incorporate lower programme effects together with reduced benefits and increased costs. However, the benefit-cost ratios remained greater than 1 across a wide range of possible scenarios. In the case of total benefits, the benefit-cost ratio was 1.03 even when benefits were reduced by 75% and costs increased by 1000%. The health service and criminal justice benefit-cost ratios remained above 1 until benefits were decreased 75% and costs increased by 200%.

{kind=link}
(A) Sensitivity of benefit-cost ratio to variation in Cardiff Violence Prevention Programme (CVPP) costs and benefits: pessimistic case. (B) Sensitivity of health service benefit-cost ratio to variation in CVPP costs and benefits: pessimistic case. (C) Sensitivity of criminal justice benefit-cost ratio to variation in CVPP costs and benefits: pessimistic case.
Overall, therefore, sensitivity analyses demonstrated that the estimated positive benefit-cost ratios for the CVPP were robust. While the estimates of programme benefits and costs are subject to uncertainty, these estimates suggest that even across a very wide range of possible variability, the programme produced net benefits to society and was cost saving from the perspective of the health and criminal justice services.
Discussion
After taking into account the costs associated with implementation, the CVPP led to a substantial reduction in costs associated with violence, for health services, criminal justice and society at large. The overall benefit-cost ratio for the CVPP was 82. There was no dedicated funding for the violence prevention activities implemented in Cardiff; prevention strategies, including ongoing adjustments to police routes and targeted locations; deployment of CCTV cameras, traffic flow and public transportation alterations; and the changes to alcohol-serving licenses and other policies, were all carried out using existing funding.
This study relied on existing estimates of the costs of violence. The strength of this approach is that decisions regarding the calculation of these estimates were made prior to, and independent of, the current study. The limitation is that all the data necessary to fully quantify the benefits of CVPP were not available. For example, it was not possible to identify the costs of the temporary extended bus services. Also, some of the costs used for the implemented strategies, such as the CCTV installation, were derived from previously published economic evaluations.
WHO report, Economic Dimensions of Interpersonal Violence,14 describes the enormous costs associated with violence globally and the need for economic evaluations of prevention strategies; lack of benefit-cost analyses is a barrier to bringing prevention strategies to scale.15 The study reported here builds on a growing literature showing that violence-prevention strategies can provide a substantial return on investment, and demonstrates the benefits of multiagency information-sharing partnerships to guide violence-prevention planning, policies and activities. Moreover, the fact that the reduction in woundings and the benefit-cost savings were documented at the community level underscores the public health significance of the CVPP model. Current economic realities mean that limited resources are available for prevention, making collaboration across sectors, including health and law enforcement as well as transportation, education, social services and others, a necessity.
Rigorous evaluation has identified prevention strategies that result in significant and sustained reductions in violence and risk for violence, including strategies which are also cost-effective.16 ,17 The CVPP model, the implementation of which is a UK government commitment (currently applied in over 130 hospitals in England and Wales), is being piloted in Scotland, Amsterdam and South Africa. The generalisability of the current results for the CVPP partnership will depend on the ‘problem-oriented’ solutions to violence implemented in other locations and the resources required. Future research will increase knowledge about how this dynamic approach is being adapted, and the effects on violence in diverse settings, including in low-income and middle-income countries. Together, the findings of effectiveness and economic evaluations provide communities with a new, low cost, low technology model for making data-driven decisions about violence prevention, the application of which has the potential to bring about substantial reductions in violence-related harm and costs to a range of major public services.
What is already known on the subject
-
A substantial proportion of violence that results in treatment by doctors is not known to the police.
-
Organised continuous sharing and use of anonymised data about violence and the involvement of clinicians in partnership work are important contributions to achieving safer communities.
-
Anonymised information derived from patients injured in violence can, when combined with police intelligence, be used to prevent violence to a greater extent than is achievable using police intelligence alone.
What this study adds
-
The cost of developing and maintaining information-sharing partnerships between police, local government and health services is low compared with the individual and societal costs of violence.
-
Anonymised information sharing for violence prevention can produce substantial cost savings to health services and the criminal justice system.
Fire and rescue services in the UK
The latest half-year statistics show the continuation of a downward trend in housefires in the UK. The total from April to September 2012 was 37% lower than in the same period in 2011. Over the longer term, the reduction is even greater such that in 2011–2012 the number was 60% lower than the average in the 1980s. (noted by IBP).
Google glass tester ticketed
A California woman was ticketed for driving while wearing Google Glass. Her citation was dismissed for lack of proof that the device was operating at the time. The legal issues aside, the important question is how Google Glass-driving wearers will be dealt with when it is obvious they have been distracted by the small screen. The driver after being ticketed stated: ‘I believe we have to start experimenting with devices like this. As a hands-free device, it is safer than a cell phone.’ That remains to be seen. (http://my.chicagotribune.com/#section/-1/article/p2p-78918730/) (noted by IBP).
Buying a gun in US pharmacies
David Lawrence forwarded a link from the Atlantic Monthly with an article noting that in the USA some pharmacists are permitted to sell guns! A large US chain of pharmacies has decided to stop selling tobacco products, but the author found many chains and independent pharmacies with Federal Firearms Licenses. One in Georgia even has a permit to sell machine guns. Editor’s note: In Montreal, the only place I know that sells guns is a counter tucked away in the back of a kitchen supply store! (noted by IBP).
Acknowledgments
We thank Linda Dahlberg (Centers for Disease Control and Prevention) for helpful comments on an earlier draft of this article. The findings and conclusions in this report are those of the authors and do not necessarily represent the official position of the Centers for Disease Control and Prevention.
Footnotes
-
Contributors CF, JS, IB and TRS designed the analyses and wrote the manuscript. CF conducted the statistical analyses. IB collated the data and conducted the data review. JS conceived the original hypothesis and initiated the programme, data sharing arrangements, and the prototype community partnership (which he convened and chaired throughout the period of the study). All authors saw and approved the final version of the manuscript. JS is guarantor.
-
Funding The development of the prototype partnership was funded, in part, by a grant from the Home Office targeted policing fund. The effectiveness study (not the benefit-cost analysis) was funded in part by the Wales Office for Research and Development in Health and Social Care (WORD), grant No R/98/037.
-
Competing interests None.
-
Provenance and peer review Not commissioned; externally peer reviewed.