Article Text

Abstract
Background The suicide rate is a macro indicator of the population's psychosocial wellbeing and an evaluation criterion of the effectiveness of suicide prevention strategies. A high level of injury deaths of undetermined intent (UD) is usually discussed in connection with the validity of suicide statistics. An effort is made to develop a criterion to characterise the quality of suicide statistics.
Methods Standardised rates of suicides (X60–X84) and UD (Y10–Y34) by the International Classification of Disease version 10 as an average for the past five available years were taken from the WHO European mortality database. Rate ratios were computed by dividing rates of UD by suicide rates.
Results There is considerable variation in suicide and UD rates among countries. The highest overall rates of UD were registered in Russia, Ukraine and Belarus, and the lowest in Greece, Spain and Italy. The EU-15 average UD rate of 1.97 and the rate ratio of 0.194 UD to suicides were combined into a ‘2-20 benchmark’, in which the primary indicator is 2.0 UD cases per 100 000 and the secondary indicator is the proportion of UD to suicides 0.20 (20%), which enables countries to be clustered according to the quality of suicide statistics. The following countries satisfied the benchmark: Greece, Norway, Spain, The Netherlands, Luxembourg, France, Austria, Italy, Romania, Hungary, Ireland and Finland.
Conclusion This study used the developed ‘2-20 benchmark’ in Europe to assess suicide registration quality in a particular country, to compare the relative position of countries, and to set a target for those European countries that have not yet achieved the benchmark.
- Attitudes
- epidemiology
- open verdict
- public health
- reliability
- suicide
- suicide/self-harm
- undetermined death
- validity
Statistics from Altmetric.com
- Attitudes
- epidemiology
- open verdict
- public health
- reliability
- suicide
- suicide/self-harm
- undetermined death
- validity
The validity of suicide statistics and the comparability of national suicide rates are important issues in the fields of epidemiology and public health. A country's suicide rate is a macro indicator of the population's psychosocial wellbeing, and it has been applied as an evaluation criterion of the effectiveness of suicide prevention strategies and intervention programmes.1–4
According to the latest official figures released by the WHO,5 suicide rates in European countries differ widely, and overall downward linear time trends in suicide mortality have been observed in most countries.6 ,7 However, variations in suicide rates can be real or can be caused by misclassification.6 ,8
The ‘injury death of undetermined intent’ (UD) diagnosis is usually discussed in connection with the validity and comparability of suicide statistics.6 ,7 ,9–12 Various causes of suicide misclassification have been identified. The main potential sources of error are registration procedures,6 ,13–15 varying quality in diagnostics and mortality statistics,16 ,17 families' dissimulation (hiding of suicides), and political motives, as described by Wasserman and Värnik18 in relation to the former USSR and, more recently, by Pridemore.19 The coronial system of injury death registration, in which coroners have to adhere to the ‘beyond reasonable doubt’ rule in determining if there is convincing evidence for the verdict of suicide, favours higher levels of UD diagnosis.20
Different researchers disagree on the extent to which variations in suicide rates can be explained by variations in the rates of UD. A consistent finding has been that suicides may be underreported,9–11 ,14 and some individual-level studies have revealed that UD may reduce the reported suicide rate by approximately 10%.10 ,21 When the national suicide prevention strategy was formulated in the UK, for example, UD were added to suicide deaths.22 Chishti and colleagues6 disagreed with the assertion that misclassification was a reason for the differing suicide rates for most of the EU-15 member states. Lester23 found that adding the rate of UD to the suicide rate did not greatly change the relative rankings of national suicide rates in the 15 countries studied. According to O'Carroll,14 it is unlikely that major conclusions based on suicide statistics are erroneous as possible errors are random. Nevertheless, some researchers argue that UD should be included in epidemiological studies on suicide.11 ,24 ,25
Only a few studies have extended the investigation of UD (International Classification of Disease version 10 (ICD-10) codes Y10–Y34) beyond the suicide category (X60–X84). Although UD is the most common verdict in cases of probable suicide,6 other subcategories of death from external causes, ie, accidents (V01–X59) and homicides (X85–Y09), may also be misclassified as ‘undetermined’ in some situations.13 ,16 ,26 ,27 Moreover, chapter XX of ICD-10, ‘external causes of morbidity and mortality’, is not the only source of possible suicide misclassification. In chapter XVIII, ‘ill-defined and unknown causes of mortality’ (R96), ‘other sudden death, cause unknown’ (R98), ‘unattended death’ (in circumstances in which the body of the deceased is found and no cause is identifiable) and ‘other ill-defined and unspecified causes of mortality’ (from unknown causes, R99) may all hide suicides. Among deaths in which no distinction between suicide and accidental death can be made as well as those categorised as caused by ‘mental and behavioural disorders due to psychoactive substance use’ (ICD-10 F10–F19), some may be suicides.28
Suicide underreporting has key implications for policy development, research funding and the evaluation of preventive programmes. To develop adequate public health strategies, policy makers need reliable epidemiological and demographic research findings.29 Knowing the magnitude of UD and what proportion of deaths from external causes is masked by it is, therefore, essential.
The aim of the current study was to make an attempt to develop one possible approach for dealing with the problem of ‘hidden’ suicides proposing a benchmark suitable for assessing the validity of suicide statistics in Europe in relation to UD.
Materials and methods
The following subcategories defined in chapter XX of ICD-10 (‘external causes of morbidity and mortality’) were taken from the WHO's European mortality database:5 suicides (X60–X84) and UD (Y10–Y34). The data refer to age-adjusted mortality rates by gender per 100 000 of population. The raw mortality data are submitted by the WHO European member states to the WHO. WHO data are compiled, validated and processed in a uniform way in order to improve the international comparability of statistics. Standardised UD rates for Russia, which were not available in the WHO database, were obtained through a personal contact (A Nemtsov). All European countries for which data were available were included in the study (listed in figure 1).

Suicides and injury deaths of untermined intent (UD) in European countries.
Data for the past five available years were used to calculate average rates per 100 000 over this period. The most recent 5-year period available was chosen to reduce the possibility of being influenced by a particular year that may have had special characteristics in some countries and would therefore result in misleading findings. Rate ratios were computed by dividing rates of UD by suicide rates.
In addition to examining the data of all European countries, a subset of countries—EU-15 (Austria, Belgium, Denmark, Finland, France, Germany, Greece, Ireland, Italy, Luxembourg, The Netherlands, Portugal, Spain, Sweden, UK), which comprises those western European welfare states that joined the European Union before 2004, was used in analysis. The average rate of UD and the rate ratio of UD to suicides in these countries was used for setting the benchmark.
Results
The general view of the suicide rate and the rate of UD in European countries is given in figure 1. The male suicide rate is taken as the basis for ranking countries. The registration of both male and female UD has the same general pattern within a country, although female rates are much smaller—the correlation between male and female UD rates by studied countries is 0.99. Therefore, later in the study gender-specific analysis was omitted and only data for the total population were used.
The overall rate of UD is by far the largest in six European countries, which were part of the Soviet Union before 1991. The Slavic republics of Russia, Ukraine and Belarus lead the list and form a group of their own with a rate of UD of over 20.0 per 100 000; the group of Baltic countries—Lithuania, Latvia and Estonia—has rate levels slightly below 10.0. In Portugal, Poland and Slovakia, the rate of UD is 5.0 or slightly over.
It is apparent that adding UD to suicides does not significantly change the rank order among countries—rank order correlation between the suicide rate and the suicide plus UD rate by studied countries is 0.96.
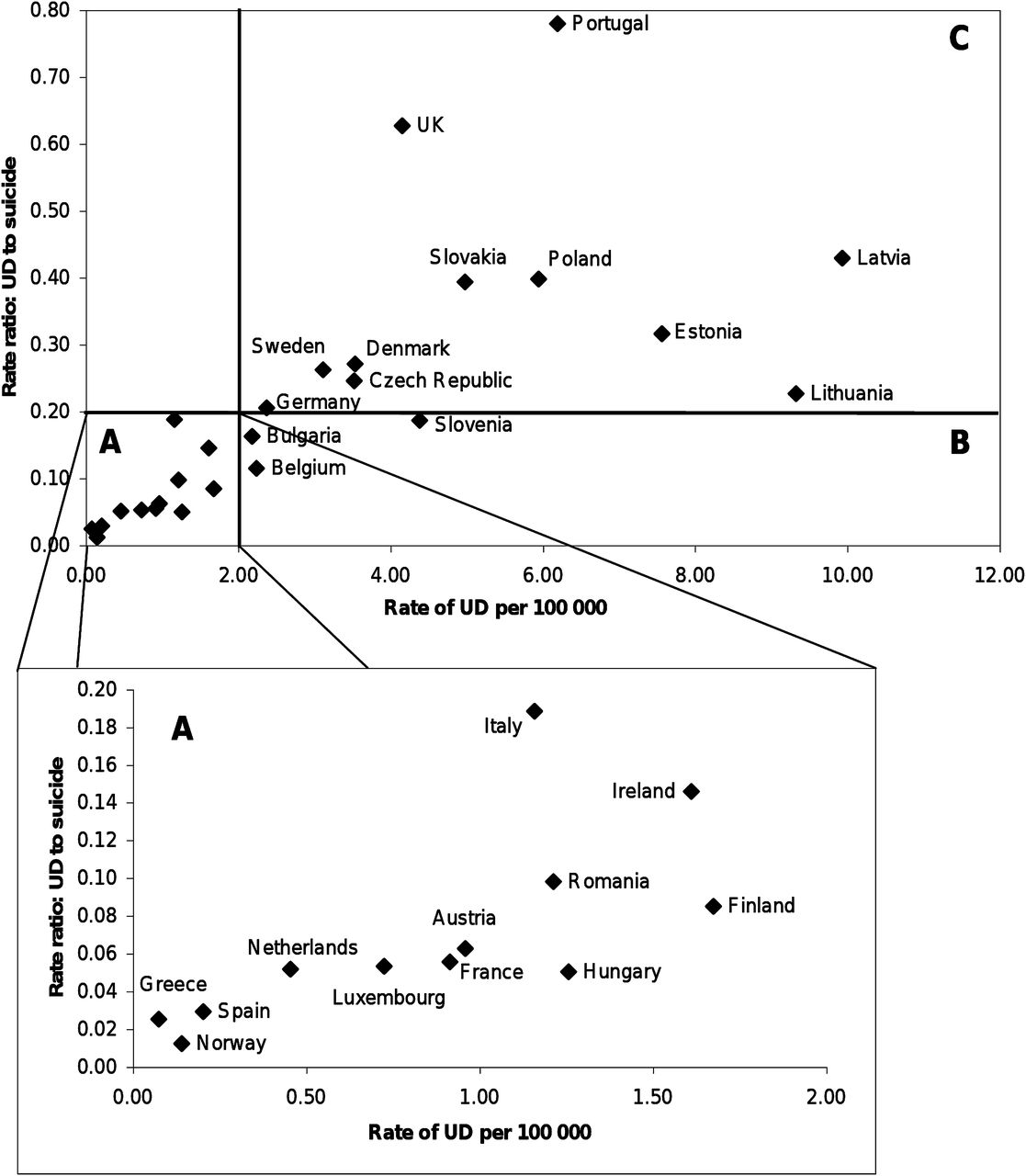
Another indicator to characterise the quality of suicide statistics—the rate ratio of UD to suicides—was combined with the overall rate of UD. In figure 2, the distribution of countries is given on the XY plane, in which the rate of UD is on the X-axis and the rate ratio of UD to suicides is on the Y-axis. The smallest rate ratio of 0.01 was found in Norway, while Portugal had a rate ratio of 0.78 and the UK 0.63. Latvia, Poland and Slovakia all had rate ratios of approximately 0.40.
{kind=link}
{kind=link}
Injury deaths of undetermined intent (UD) according to data from five last available years in European countries. CIS Slavic countries (not shown in the figure 2 because of extreme values) have the following x-axis values: Russia (33.50; 0.99); Ukraine (21.52; 0.97); Belarus (19.48; 0.61).
The EU-15 average suicide rate per 100 000 was 10.15 and the average UD rate per 100 000 was 1.97 during 1997–2006. Therefore, the rate ratio of UD to suicides was 0.194. For purposes of convenience of use the numbers were rounded up to 2 and 0.20 (ie, 20%), respectively.
Discussion
The quality of injury mortality statistics depends on various country-specific circumstances such as: (1) routines for registering suicides and other external causes of deaths;15 ,25 ,29 (2) the economic situation, which determines the resources available for medical and legal inquest into causes of death (autopsy, forensic autopsy, police/prosecutor investigation);15–17 (3) the strictness of and adherence to regulations concerning statistical data about causes of death;12 ,13 (4) varying proportions of suicide methods (hanging and jumping, which are usually easy to diagnose as suicides, versus drowning, using street drugs, or traffic accidents, in which the intent is more difficult to determine);30 (5) cultural issues (stigma and denial at the family level);31 (6) financial implications for relatives, depending on life insurance regulations and practices;32 ,33 (7) the sociopolitical situation, which may bring forth wishes of the government to suppress one diagnosis of death at the expense of another.16 ,17
All of the above combine to affect the final statistical outcome, although the strength of particular circumstances may vary widely across countries. The level of UD is positively correlated with the level of suicides over time, although the differences among countries are considerable.6 ,9 To describe the situation of the countries studied, it was deemed necessary to set benchmark figures using two indicators—the rate of UD and the rate ratio of UD to suicides. EU-15 countries were chosen for constructing the benchmark because due to much higher gross domestic products per capita it was assumed that the availability of resources for death investigation in general should not be a limiting factor in these countries. Also these countries have been structurally more stable in the long term, while only some transitional countries of eastern Europe are showing signs of gaining stability.
The average rate of UD in the EU-15 countries is slightly below 2.0 per 100 000. A benchmark figure has to be easy to understand and remember while being achievable, initially by some countries and eventually by all countries to which it is applied. While the ideal target is set at no UD, it may be unachievable due to the inherent incompleteness of available data to forensic experts in some cases of death. There is genuine worry about levels of diagnosed UD being too high in many countries. The rate of 2.0 is thus considered to be a good benchmark at this point in time.
The benchmark for the rate ratio of UD to suicides is derived from the UD rate benchmark. The rate ratio is not a new measurement as it has been used before.12 ,15 ,18 ,27 Moreover, this indicator is easy to understand because the quantity of UD is primarily associated with the validity of suicide statistics. The average suicide rate in the EU-15 countries during the studied years is very close to 10.0, so the appropriate benchmark is 0.20 (2.0 divided by 10.0). As it also depends on the level of suicides: a higher suicide rate ‘allows’ for the rate of UD also to be somewhat higher and still be below the rate ratio component of the benchmark. When the suicide rate is low, the rate of UD also has to be very low to satisfy the benchmark.
The resulting composite indicator is the ‘2-20 benchmark’ for measuring suicide registration quality. When countries are classified according to this benchmark, the following picture appears.
Sector ‘A’ in figure 2 includes countries that fare better against both benchmarks. This includes Norway, Greece, Spain, The Netherlands, Luxembourg, France, Italy, Austria, Romania, Hungary, Finland and Ireland. Most have belonged to this sector for a long time but some like Finland and Ireland have only achieved this quite recently.
Sector ‘B’ includes the countries Belgium, Bulgaria and Slovenia. These meet the rate ratio 0.20 benchmark but have a rate of UD over 2.0.
Sector ‘C’ includes the countries that do not meet the benchmark criteria for either indicator—Germany, Sweden, Czech Republic, Denmark, UK, Slovenia, Slovakia, Poland, Portugal, Estonia, Lithuania and Latvia. While some are close to benchmark levels, others are still quite far from these. Belarus, Ukraine and Russia also belong to this sector but have been left out of figure 2 because their very high rates of UD would dwarf the indicators of the other countries. It should be noted that in these countries verdicts of UD may mask fewer suicides and more homicides than in other studied countries, therefore the reduction in UD does not fully reflect an improvement in suicide data.
The letters ‘A’, ‘B’ and ‘C’ identifying the sectors can be understood and used as grades for the countries in terms of the quality level of their suicide registration. When efforts to reduce verdicts of UD begin to pay off, countries will gradually move from sector ‘C’ towards sector ‘A’.
Limitations and implications
The ‘2-20 benchmark’ does not make statistics more valid. It cannot be used to improve past statistics because proposing a universal estimation quota for adjusting suicide rates according to the level of possible ‘hidden’ suicides is impossible if only aggregate-level data are available. To affirm with certainty how many UD should be reclassified as suicides needs an individual-level approach, for example, critical evaluation of a sample of death certificates issued.
The ‘2-20 benchmark’ does, however, give an understanding of the level of validity of suicide statistics and sets alarm bells ringing for countries in which benchmark criteria are not met. It is a general performance benchmark to be achieved.
It should be borne in mind that the numeric value of the benchmark is constructed on the basis of current levels of suicide and UD in Europe, it may be not directly applicable in the distant future or in completely different cultures.
Conclusions
Two indicators have been developed to measure the situation regarding the handling of UD in Europe. The level of two cases per 100 000 inhabitants per year is the primary benchmark. The secondary indicator is the proportion of UD to suicides during the same period for which a coefficient of 0.20 is the benchmark. It is recommended to use the ‘2-20 benchmark’ for measuring suicide registration quality, assessing the relative position of countries, and for setting a target for those countries that have not yet achieved the benchmark.
What is already known on the subject
-
The problem of ‘hidden suicides’ under the diagnosis ‘injury death of undetermined intent (UD)’ is an issue constantly challenging researchers in the field of epidemiology, demography and public health, usually discussed in connection with the reliability and comparability of suicide statistics.
-
Several researchers combine suicide rates and the rates of UD for suicide research purposes.
-
Our previous study about the structure of UD in ex-USSR Baltic and Slavic countries (P Värnik, 2010) has shown that undetermined deaths do not hide suicides alone, but also accidents and homicides could sometimes be diagnosed as undetermined.
What this study adds
-
In the current study the ‘2-20 benchmark’ has been worked out and is recommended for use in Europe to measure the quality of suicide statistics, for setting a target for those countries that have not yet achieved the benchmark and clustering countries accordingly.
-
The level of two cases of UD per 100 000 inhabitants per year is the primary indicator.
-
The secondary indicator is the proportion of UD to suicides during the same period for which a coefficient of 0.20 (20%) is the benchmark.
-
The rationale behind these indicators is based on the exploration of the EU-15 average figures.
Policy implications
-
Reliable suicide reporting has key implications for policy development, research funding and the evaluation of preventive and intervention programmes.
Acknowledgments
The authors would like to thank Professor Alexander Nemtsov (Head of the Department of Informatics and System Investigations of the Moscow Research Institute of Psychiatry, Russian Federal Ministry of Public Health) for his help in collecting the data for Russia. Thanks are also due to Delaney Skerrett for his thorough linguistic and stylistic revision of the manuscript.
References
Footnotes
-
Funding The research reported in this paper has received funding from the European Community Seventh Framework Programme (FP/2007–2013) OSPI-Europe under grant agreement no 223138, and from the Estonian Ministry of Social Affairs.
-
Competing interests None.
-
Provenance and peer review Not commissioned; externally peer reviewed.
-
Data sharing statement The study is based on publicly available data and previously published sources.