Article Text

Abstract
Objective: To appraise the published epidemiological evidence quantifying the risk of falls associated with acute and usual alcohol consumption among young and middle-aged adults.
Design: Systematic review.
Methods: Data sources: searches of electronic databases (eg, Medline, EMBASE, CINAHL, PsycINFO, Scopus), websites of relevant organisations, major injury journals, reference lists of relevant articles, and contact with experts in the field. Inclusion criteria: epidemiological studies with an English language abstract investigating alcohol use as a risk factor (exposure) for unintentional falls or related injuries among individuals aged 25–60 years. Studies were critically appraised using the GATE LITE tool. Meta-analysis was not attempted because of the heterogeneity of the eligible studies.
Results: Four case–control, three cohort and one case–crossover study fulfilled the inclusion criteria. The studies showed an increased risk of unintentional falls among young and middle-aged adults with increasing exposure to alcohol use. However, the magnitude of this risk varied considerably across studies with most estimates being relatively imprecise. Modest evidence of a dose–response relationship with acute alcohol use was observed. The association between usual alcohol use and fall risk was inconclusive, and evidence of a gender difference was inconsistent.
Conclusions: Alcohol use appears to be an important risk factor for falls among young and middle-aged adults. Controlled studies with sufficient power that adjust effect estimates for potential confounders (eg, fatigue, recreational drug use) are required to determine the population-based burden of fall-related injuries attributable to alcohol. This can help inform and prioritise falls prevention strategies for this age group.
Statistics from Altmetric.com
Injury prevention strategies targeting the harmful effects of alcohol use on road traffic crashes are well established. While serious falls are a leading cause of injury-related morbidity worldwide,123456 the evidence base for determining if fall prevention strategies should target alcohol use has received relatively little attention. A number of major reviews have examined the role of alcohol in non-traffic injuries.78910 However, only one review, published by Hingson and Howland in 1987, has specifically examined the link between alcohol and falls.11 This review found an association with acute alcohol use and risk of fall, but concluded that more case–control studies were required to establish the magnitude of the risk. Over a decade later, Smith et al found that alcohol was an important contributor to serious falls in a review of non-traffic fatal injuries.12 The aggregated proportion of fall cases determined to be intoxicated was 32.2%, comparable to 32.8% of motor vehicle crash victims. These authors also noted a lack of case–control and prospective cohort studies investigating the relationship between alcohol use and fatal non-traffic injuries.
The aim of this study was to quantify the magnitude of fall risk associated with both acute and usual alcohol use among young and middle-aged adults, including the research published in the 20 years since the paper by Hingson and Howland. This review will help to establish the evidence base for targeted fall prevention strategies in this age group.
Methods
Inclusion criteria
We included epidemiological studies examining the association between alcohol use and the occurrence of unintentional falls or fall-related injury. The exposure of interest was defined as either usual alcohol use, or the acute consumption of alcohol in a defined period immediately prior to the event (or reference period). Study inclusion required the following criteria to be met: study population to include young and middle-aged adults defined for the purposes of this study as 25–60 years (or a sub-group within this age range), information regarding alcohol use, and an English language abstract.
Studies including subjects in residential care, work-related falls, or studies of injuries limited to a specific body region (eg, hip fracture, traumatic brain injury, maxillofacial injuries) were excluded. Given the focus of the review, data specific to unintentional falls were extracted from studies focusing on injury more generally; if this was not possible the study was excluded.
Data sources and search terms
Research published from 1983 to 2007 was reviewed. The review period included the only case–control study13 in the Hingson and Howland review. Bibliographic computerised searches using the Ovid search engine of the following databases were undertaken: Medline, EMBASE, CINAHL, PsycINFO, and Scopus. Main medical subject heading (MeSH) and text words search terms included: accidental falls; accidents, home; alcohol, ethyl; BAC; and alcohol drinking.
Additional strategies utilised to identify potentially relevant studies included: examination of reference lists of retrieved articles and proceedings of applicable conferences; hand-searching of the table of contents of journals (Injury; Injury Prevention; Journal of Safety Research; Journal of Trauma; Journal of Trauma, Injury, Infection and Critical Care; Alcohol and Alcoholism; and Alcohol); electronic media searches of internet sources, websites of institutions involved in research and policy in the areas of falls or alcohol, particularly focusing on publication lists; and contact with key researchers in the field.
Quality assessment
The quality of studies fulfilling the inclusion criteria was assessed using GATE LITE (www.epiq.co.nz), which is an abbreviated form of the GATE frame—a visual framework used to appraise epidemiological studies.14 Evidence tables for included studies were developed, and included information regarding participants, comparison group, exposure, confounders considered, outcomes, results, and appraisals of study quality and biases of the research. The identified studies were heterogeneous in many respects and were not considered sufficiently robust to quantitatively combine.
Results
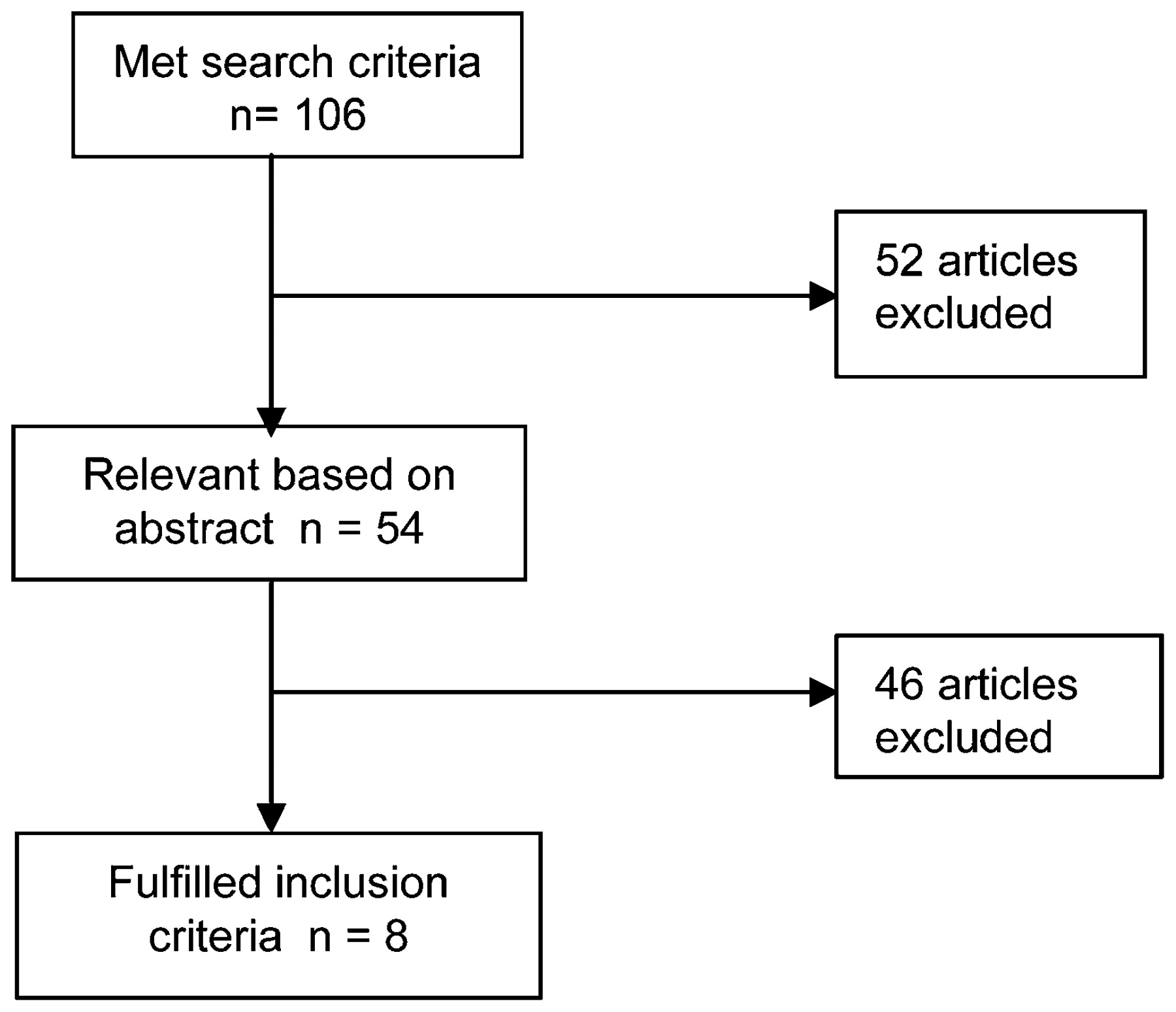
Of the 106 studies identified from the search strategy, 54 were considered potentially relevant based on the title or abstract and the full text retrieved for detailed evaluation. Eight studies from the United States,15161718 Finland,1319 Sweden,20 and Canada,21 published between 1983 and January 2005, fulfilled the review inclusion criteria (fig 1).

{kind=link}
Inclusion and exclusion flow chart for risk factor studies.
Study characteristics
The primary focus of four of the studies was falls.13171921 The remaining four were general injury studies where data on falls could be identified as a sub-group (table 1).15161820 Three studies were explicitly population based.161920 Participants in the other studies were identified from selected emergency departments (EDs) and hospitals in four,13151718 and a medical clinic in one.21 The research designs included four case–control studies,13151617 three cohort studies,192021 and a case-crossover study.18 The individual sample sizes ranged from 118 to 19 582. The overall mean age of patients in the four studies providing information was 47.4 years.
Alcohol consumption and the risk of fall injury among young and middle-aged adults: summary of epidemiological evidence
The proportion of fall subjects who had been drinking within six hours of the event (where data was reported) ranged from 14% to 53%.131518
The outcome measures included self-reported falls (injurious and non-injurious),21 ED visit or admission to hospital for a fall-related injury,1315181920 death as a result of a fall-related injury,1620 and fractures as a result of falls.17 While two studies described the circumstances of the falls in limited detail,1719 neither reported if the association with alcohol varied in different contexts.
Selection biases
The identification and recruitment of study cases from hospital ED and admission records may have introduced selection biases due to the unreliability of the coding of fall injury,2223 and to referral patterns and access issues that result in some cases attending ED while others seek care from alternative providers or not at all.2425 Moreover, trauma studies based only on admitted patients may be more likely to include intoxicated minor injury cases, due to the difficulty of initial clinical assessment among intoxicated patients which can result in biased estimates of association between alcohol and injury risk.25
In the seven studies reporting response rates, these ranged from 65% to 96%.13151617181920 Studies with unreported or low response rates are more likely to yield biased effect estimates as respondents may be systematically different from non-responders with regard to exposure measures. A cohort study of individuals with traumatic brain injury, found subjects lost to follow-up were more likely to be those who were intoxicated at the time of injury and those with a history of substance abuse.26
The selection of non-injured patients17 and patients injured by other mechanisms15 as controls in two studies meant that these controls may not have represented the same populations generating the cases.242728 Previous studies have found non-injured patients to be more frequent heavy drinkers than the general population,29 potentially resulting in conservative estimates of the effect of alcohol on injury.
Information biases
The measurement of exposures and outcomes commonly relied on self-report, raising the possibility of recall bias and socially desirable responses. The latter may have resulted in an underestimate of effect in some studies.30 Follow-up periods for two of the cohort studies exceeded 10 years,1920 and it is likely that drinking patterns changed within that period.
The alcohol use measures investigated were self-reported volume of alcohol consumption in the preceding 4–6 hours,151718 blood alcohol concentration (BAC),13 breath alcohol concentration,1315 self-reported level of drunkenness,15 and usual alcohol consumption.151617192021 ED records were used in two studies to identify BAC.1315 These data are commonly incomplete,233132 potentially resulting in missing exposure or confounder information.
Confounding
The effect of recreational drug use and fatigue on the relationship between alcohol and falls appears to have been considered in only two studies.2021 These variables may have a relationship with both alcohol use and risk of fall, and could have distorted the risk estimates of interest.30 Previous research has found that the association between acute alcohol consumption and injury risk can be confounded by usual patterns of drinking, risk-taking behaviours and the use of other substances.33 Although age, gender, and socioeconomic status could have an association with both alcohol use and risk of falls,33 it was unclear if their potential confounding effects were adequately considered in one study.21
Effect estimates
Two1517 of the four studies13151718 investigating the association between acute use of alcohol and fall risk found statistically significant increases in risk. The first of these, a case–control study15 examining ED presentations for falls compared with presentations for injuries from animal bites, recreational “accidents” or workplace “accidents”, reported odds ratios (OR) of 3.45 (95% CI 1.23 to 9.66) for breathalyser readings of ⩾10 mg/100 ml compared with ⩽9 mg/100 ml; OR = 6.73 (95% CI 1.54 to 29.34) for self-reported consumption of 101–2000 ml of alcohol in the previous six hours compared to abstainers; and OR = 5.70 (95% CI 1.96 to 16.56) for those self-identifying as “drunk” compared with abstainers.15 As alcohol could also have influenced the injuries experienced by the control group, these estimates may be biased and result in an underestimation of the risk.
A subsequent case–control study of hospital presentations (inpatient and outpatient) for fractures attributed to falls compared with presentations for other conditions found the fracture group had a threefold greater risk of exposure to alcohol use in the previous four hours (OR = 3.1; 95% CI 1.6 to 6.0).17 However, the generalisability of these findings is limited by the particular type of fall injury investigated.
The remaining two studies that examined acute alcohol use found an increased fall risk, but the precision of these estimates was of concern.1318 The first of these was a case–control study examining BAC levels among ED presentations following a fall in a public place compared with controls randomly selected from the incident site.13 While the authors report an increased fall risk associated with BAC of ⩾60 mg/100 ml, information regarding the precision of these estimates was not provided. The second was a case–crossover study of ED fall injury presentations which found that alcohol use in the preceding six hours was associated with an OR = 3.0 (95% CI 0.54 to 30).18 These findings are equivocal as the CI was extremely wide.
There was some evidence of a dose–response relationship with acute alcohol use and fall risk reported in two of the studies reviewed.1315 The case–control study by Honkanen et al reported relative risk (RR) of around 3 for BAC of 60–100 mg/100 ml, RR = 10 for BAC of 101–150 mg/100 ml, and RR = 60 for BAC of ⩾160 mg/100 ml compared to BAC of 0 mg/100 ml.13 While this study indicates a dose–response relationship, information regarding the precision of these estimates was not reported. Another case–control study of fall-injury requiring hospitalisation reported an OR of 2.09 (95% CI 0.66 to 6.56) for breath alcohol levels of ⩽100 mg/ml compared with abstainers, increasing to OR 6.73 (95% CI to 1.54 to 29.34) for 101–2000 mg/ml.15 Despite the imprecision of the estimates in this study, the direction of the relationship is clear.
While three161920 of six studies found that usual alcohol use increased fall risk, others did not find a significant association.151721 Two cohort studies1920 examining usual alcohol intake per month compared with abstainers reported statistically significant relative risks of around 2.0 for consumption of ⩾500 g of alcohol per month. The more robust of these two studies showed a dose–response relationship, with increased usual alcohol consumption correlating with an increase in risk of fall.19 Compared to abstainers, relative risks increased from 1.43 (95% CI 1.13 to 1.82) for those consuming 100–499 g of alcohol per month to RR = 3.05 (95% CI 2.05 to 4.55) for consumption of ⩾1000 g per month. A case–control study investigating drinking history and risk of fatal injury found current drinkers (at least 12 drinks in the last year of life) were at increased risk of death from falls compared with abstainers and prior drinkers (OR = 1.38; 95% CI 1.05 to 1.82).16
Two case–control studies examining usual alcohol consumption and fall risk found no significant relationship.1517 Gray et al, in a cohort study of self-reported falls, found a non-significant increase in fall risk associated with the consumption of one or more drinks per day compared to less than one drink (OR = 1.85; 95% CI 0.73 to 4.67).21
No studies reported statistically significant gender differences in fall risk associated with acute alcohol use, and the evidence relating to usual alcohol consumption was inconsistent. One study found a significantly increased risk for women (aged 20–59 years) with high usual alcohol consumption (⩾500 g/month) of fall-related hospitalisation or death, after controlling for confounders, while the risk was only marginally significant for men of the same age.20 However, another study using similar cut points but examining consumption by age group, found men aged 20–44 years consuming 500–999 g/month had a threefold increase in risk (RR = 3.00; 95% CI 1.45 to 6.19) of hospitalisation or death resulting from falls, after controlling for confounders, compared with women of the same age (RR = 0.77; 95% CI 0.10 to 6.03).19 This pattern was reversed in the older age group (45–64 years), with women consuming ⩾500 g/month having almost double the risk of their male counterparts (RR = 4.57; 95% CI 1.68 to 12.45 cf. RR = 2.75; 95% CI 1.58 to 4.79). A study investigating fatal falls found similar risks among men and women who were current drinkers compared with abstainers.16
Discussion
Several studies have investigated the association between alcohol consumption and fall risk since the last substantive review by Hingson and Howland in 1987.11 Studies examining associations between acute alcohol use and risk of non-occupational unintentional falls among young and middle-aged adults have found a consistent relationship, although the estimates of risk varied with respect to magnitude and precision. There was some evidence of a dose–response relationship with acute alcohol use, though again the estimates lack precision. Evidence of any gender difference is inconsistent.
There is inconclusive evidence of an association between usual alcohol use and fall risk among young and middle-aged adults. Confounding was not adequately considered in a number of studies. Some studies were compromised by the delay between measurement of alcohol consumption and measurement of outcomes, and gross measures of usual alcohol use, resulting in potential recall and other measurement biases. The wide range of measures used to characterise usual alcohol consumption highlights the need for a consistent measure that can be used across countries.
With these caveats, the findings of this review are consistent with those from Hingson and Howland’s review and provide additional support for the contention that acute alcohol use increases the risk of unintentional falls.11 The findings also support some of the Bradford Hill criteria used to assess if an association is consistent with a causal relationship. Specifically, the temporal and statistically significant relationship between alcohol and falls is plausible and coherent, and there is some evidence of a dose–response effect. However, the magnitude of this risk among young and middle-aged adults remains subject to several sources of systematic error and imprecision. Moreover, there is insufficient evidence to conclude that there is an important association between usual alcohol use and fall risk in this age group.
Publication bias arising as a result of a number of factors—including studies with significant findings being more likely to be published,3435 and computerised databases being less likely to index non-English language published research, research undertaken by low-income countries, or research in the grey literature3637—can threaten the validity of systematic reviews.34 Threats to this review from publication and language biases were reduced by implementing a broad and comprehensive search strategy and by making contact with experts in the field. Acknowledging these strengths and limitations, it is noteworthy that all eligible studies were conducted in high income countries in North America and Europe. Yet the burden of falls is disproportionately borne by low and middle-income countries,38 indicating an important gap in context-based evidence.
The heterogeneity in research designs, variable definitions and study context made the meta-analyses of pooled data inappropriate in the present review. Instead, recommended criteria were used to critically appraise and synthesise the evidence.143940
The primary focus of this review was to use well recognised criteria to evaluate the evidence regarding the magnitude of unintentional fall risk associated with both acute and usual alcohol consumption among young and middle-aged adults. Therefore we did not include studies limited to study populations with injuries in specific regions of the body (eg, traumatic brain injury, maxillofacial injuries, and hip fracture). These studies may have provided insights regarding the role of alcohol in these particular types of injuries, not all of which may be generalisable to falls.
The studies selected for this review were case–control, case–crossover or cohort studies, methodological designs suited to investigate the aetiology of injury.24272841 While our inclusion criteria were relatively strict with regard to eligible study designs, the quality of the included studies was quite variable. The lack of primary analytical studies with a population focus is a major limitation identified in this review. A number of studies drew participants from specific emergency departments, hospitals or clinics, introducing a number of selection biases.22234243
The use of non-population based controls was a limitation in a number of the studies reviewed and may have resulted in differential ascertainment of exposure among cases and controls.242844
Several studies were compromised by the lack of objective measures of acute alcohol exposure. Research by Cherpitel et al indicates that only about 50% of US trauma centres routinely obtain blood alcohol on injury patients.45 In addition, clinician detection of acute alcohol intoxication is unreliable and screening for alcohol intoxication is undertaken inconsistently.464748 Those with severe injuries may also be less likely to have BAC estimated in a timely fashion due to other clinical management priorities.3049 In some situations the consumption of alcohol may have taken place after the injury event, an argument for complementing BAC levels with self-report data on when—in relation to the injury—alcohol was consumed.30
The use of abstainers as the reference group for the calculation of risk estimates for alcohol use was common.1619 Concerns previously identified regarding the use of self-identified abstainers as a control group include their potential heterogeneity, measurement error, and representativeness of the underlying study populations.5051 Abstainers may be lifetime abstainers, long-term abstainers or former drinkers. Rehm et al estimate that inconsistencies in self-report of lifetime abstention from alcohol can result in the underestimation of alcohol-attributable all-cause mortality by 2–17%.50
Other factors with a transient effect on fall risk, such as recreational drugs and fatigue, were seldom considered as potential confounders in the studies reviewed. Information on the type and circumstances of falls was not reported in most studies. This information is required to identify whether the relationship differs in different contexts (eg, home, public places) and by type of fall (eg, stairs, ladder, slips and trips).
This review excluded work-related falls. Smith et al identified that falls at work and other settings such as the home are likely to share many common characteristics.5253 Opportunities exist to explore injury prevention strategies aimed at reducing alcohol related harm that transcend the boundaries of workplace and home. Specific interventions to reduce the risk of fall injuries among young and middle-aged adults could include strategies aimed at screening for alcohol abuse and brief interventions for hazardous drinkers in the emergency department and primary care settings.5455
In conclusion, this review has been unable to precisely quantify the risk associated with acute alcohol use and unintentional falls among young and middle-aged adults. However, the findings of the review suggest that alcohol increases the risk of falls, although the magnitude of this risk remains uncertain. Sufficiently powered population-based studies conducted in settings that encompass a range of socioeconomic contexts are required to enable estimation of the fall injury burden attributable to alcohol. The multifactorial nature of falls requires the consideration of other potential contributing causes, confounders, and consideration of interactions between alcohol and factors such as fatigue and recreational drug use.
What is already known on this subject
An association between acute alcohol and risk of fall among adults has been noted, but previous reviews have identified a gap in epidemiological evidence regarding the magnitude of the risk.
REFERENCES
Footnotes
Funding This research was funded and supported by the Accident Compensation Corporation (ACC), Wellington, New Zealand. Views and/or conclusions in this article are those of the authors and may not reflect the position of ACC.
Competing interests None.
Ethics approval Ethics approval was obtained.
Contributions: BK carried out the search, selected included papers, critically appraised the papers, developed the evidence tables, and wrote the initial draft of the paper. RJ and SA were reviewers for included critically appraised papers and contributed substantially to the interpretation of study findings and writing the paper.
Provenance and Peer review Not commissioned; externally peer reviewed.