Article Text

Abstract
Objective—This study describes epidemiologic patterns of mortality due to suicide, homicide, and war for the world in order to serve as a benchmark against which to measure future progress and to raise awareness about violence as a global public health problem.
Setting—The world and its eight major regions.
Method—Data were derived from The Global Burden of Disease series and the US National Center for Health Statistics to estimate crude rates, age adjusted rates, sex rate ratios, and the health burden for suicide, homicide, and war related deaths for the world and its eight major regions in 1990.
Results—In 1990, an estimated 1 851 000 people died from violence (35.3 per 100 000) in the world. There were an estimated 786 000 suicides. Overall suicide rates ranged from 3.4 per 100 000 in Sub-Saharan Africa to 30.4 per 100 000 in China. There were an estimated 563 000 homicides. Overall homicide rates ranged from 1.0 per 100 000 in established market economies to 44.8 per 100 000 in Sub-Saharan Africa with peaks among males aged 15–24 years old, and among females aged 0–4 years old. There were an estimated 502 000 war related deaths with peaks in rates for both sexes among people aged 0–4, 15–29, and 60–69 years old.
Conclusion—The number of violence related deaths in the world is unacceptably high. Coordinated prevention and control efforts are urgently needed.
- violence
- homicide
- suicide
- war
- cross cultural comparison
Statistics from Altmetric.com
If we are to envision a less violent world, we must first understand how violent the world is. The extent of global violence, however, has never been fully described. But now, with the availability of reliable estimates, it is possible to examine the impact of violence world wide. Such an analysis is timely, because violence has emerged as a global public health priority.
In 1996, the World Health Assembly declared violence a leading global public health problem.1 This declaration acknowledges the necessity of implementing a global strategy to address violence as a health issue that can be prevented. The first step toward building the foundation necessary to control and prevent violence is describing the magnitude and nature of the problem.2
This study describes, for the first time, epidemiologic patterns of violence related mortality (including homicide, suicide, and war) for the world and its major regions. Archival data from The Global Burden of Disease series3 are used to generate global estimates of age and sex specific and age adjusted rates of homicide, suicide, and war related deaths.
Most cross national research on homicide and suicide has relied upon data from countries with complete vital registration systems, which are primarily developed countries.4–12 Consequently little is known about the patterns of violence related mortality in countries with developing economies. Moreover, although war makes a substantial contribution to the global burden of health, there is little cross national epidemiologic research on the subject.13–15 The findings presented in this paper are intended to highlight epidemiologic patterns in violence related mortality across all regions of the world and raise awareness of violence as a global public health problem.
Methods
DEFINITIONS
We analyzed four categories of violence related deaths including suicide, homicide, war, and overall violence. Violence can generally be defined as the threatened or actual use of physical force or power against another person, against oneself, or against a group or community, that either results in or has a high likelihood of resulting in injury, death, or deprivation.16 The definitions of the categories of violent death used in this study were based on those described in volume one of The Global Burden of Disease series3 our primary data source. The first category is suicide (E950–E959), defined as fatal self inflicted injuries specified as intentional.17 The second category is homicide (E960–E969), defined as fatal injuries inflicted by another person with intent to injure or kill, by any means.17 This category also includes unintentional firearm related deaths (E922). Unintentional firearm related deaths are traditionally analyzed separately from homicide but were included with homicide in our study because that is how the category was defined in The Global Burden of Disease series. However, the number of unintentional firearm related deaths is small compared with that of homicides. For example, there were 82 465 homicides compared with 3733 unintentional firearm related deaths in 36 high and upper middle income countries during a one year period.18 The third category is war related deaths (E990–E999), defined as fatal injuries to military personal and civilians caused by war and civil insurrections and occurring during the time of war and insurrection.17 The fourth category is overall violence including suicide, homicide, and legal intervention (E960–E978), unintentional firearm related deaths, and war. Legal intervention (E970–E978) is defined as fatal injuries inflicted by law enforcement agents in the course of duty and legal execution.17
DATA SOURCES
The data used in this study were derived from The Global Burden of Disease series.3 This series provided archival information on numbers of deaths by age, sex, and cause as well as population estimates for eight regions of the world in 1990. Regions were classified as established market economies (EME), formerly socialist economies of Europe (FSE), India, China, other Asia and islands (OAI), Sub-Saharan Africa (SSA), Latin America and the Caribbean (LAC), and the Middle Eastern crescent (MEC) (appendix 1).
The methods used to estimate mortality data for each region are fully explained in volume one of The Global Burden of Disease series.3,4 Because of differing availability of vital data on mortality, varying methods were utilized to calculate mortality data.4 Estimates for EME and FSE were obtained from vital registration data. However, estimates for China and India were calculated using sample registration data. In China, the sample registration data are based on a single monitoring system of causes of death in a representative sample of counties called disease surveillance points covering 10 million people in rural and urban areas. Unlike China, the sample registration data used in India are from two separate systems used in urban and rural areas. For remaining regions, reliable mortality data were limited and not considered representative of the entire population. To address this limitation, cause-of-death structures were used to estimate distribution of causes by age and sex for areas within these regions for which valid death registration data were unavailable (that is, the residual areas). The first step was to estimate the total mortality rate in residual areas using the Lorenz curve method (an equation that can be used to estimate the cumulative proportion of a population as a function of the cumulative proportion of deaths). The Lorenz curve was used to estimate the population covered by areas with registration systems by inputting the percentage of regional deaths recorded in these areas. The deaths and population in each residual area was then determined by subtracting the estimated deaths and population for the registration areas from the regional totals for deaths and population. The all-cause mortality rate for each age and sex group in residual areas of each region was then calculated using these death and population estimates. Once total mortality rates were estimated, probability models of cause-of-death structure were used to determine mortality for broad categories of causes for residual areas (that is, communicable, maternal, perinatal, and nutritional conditions; non-communicable diseases; and injuries). The predicted estimates from the cause-of-death structure for residual areas were adjusted to reflect the deviation between the predicted and observed mortality patterns for registered areas. To obtain more detailed information on causes of mortality, the distribution of deaths for age and sex specific causes within each of the broad categories were assumed to be the same as in registered areas.
Information presented on the United States was drawn from two sources. The National Center for Health Statistics19 and the United States Census Bureau.20
DATA ANALYSIS
We calculated crude and age adjusted rates of death per 100 000 for each region for suicide, homicide, war, and overall violence. Age adjusted rates were calculated using the standard world population.21 For each region, age and sex specific rates of death per 100 000 were calculated. Sex rate ratios were also calculated for each region by dividing mortality rates for males by rates for females. Because violence related deaths in the United States have been described to differ from other high income countries,12 we examined rates in the United States separately from other EME. To calculate United States rates we subtracted the number of deaths and population in the United States from EME estimates. Except where indicated, all rates were age adjusted.
Results
In 1990, there were an estimated 1 851 000 violence related deaths (35.3 per 100 000) in the world (table 1 and fig 1). Overall rates of violence related deaths ranged from 12.5 per 100 000 in EME excluding the United States (−US) to 101.0 per 100 000 in SSA. Rates of violence related deaths were highest in SSA, MEC, and FSE and lowest in EME (−US). In 1990, an estimated 3.7% of all deaths in the world were violence related (table 2). Suicide was the most frequent form of violent death followed by homicide and then war related deaths. The global risk of suicide was 1.7 times that of war related deaths and 1.4 times that of homicide. Violence accounted for a greater proportion of total deaths in SSA than in any other region of the world (table 2).
Numbers* and rates† of violent related deaths by type of violence and region, world, 1990
Percentage of all deaths that are violence related, 1990
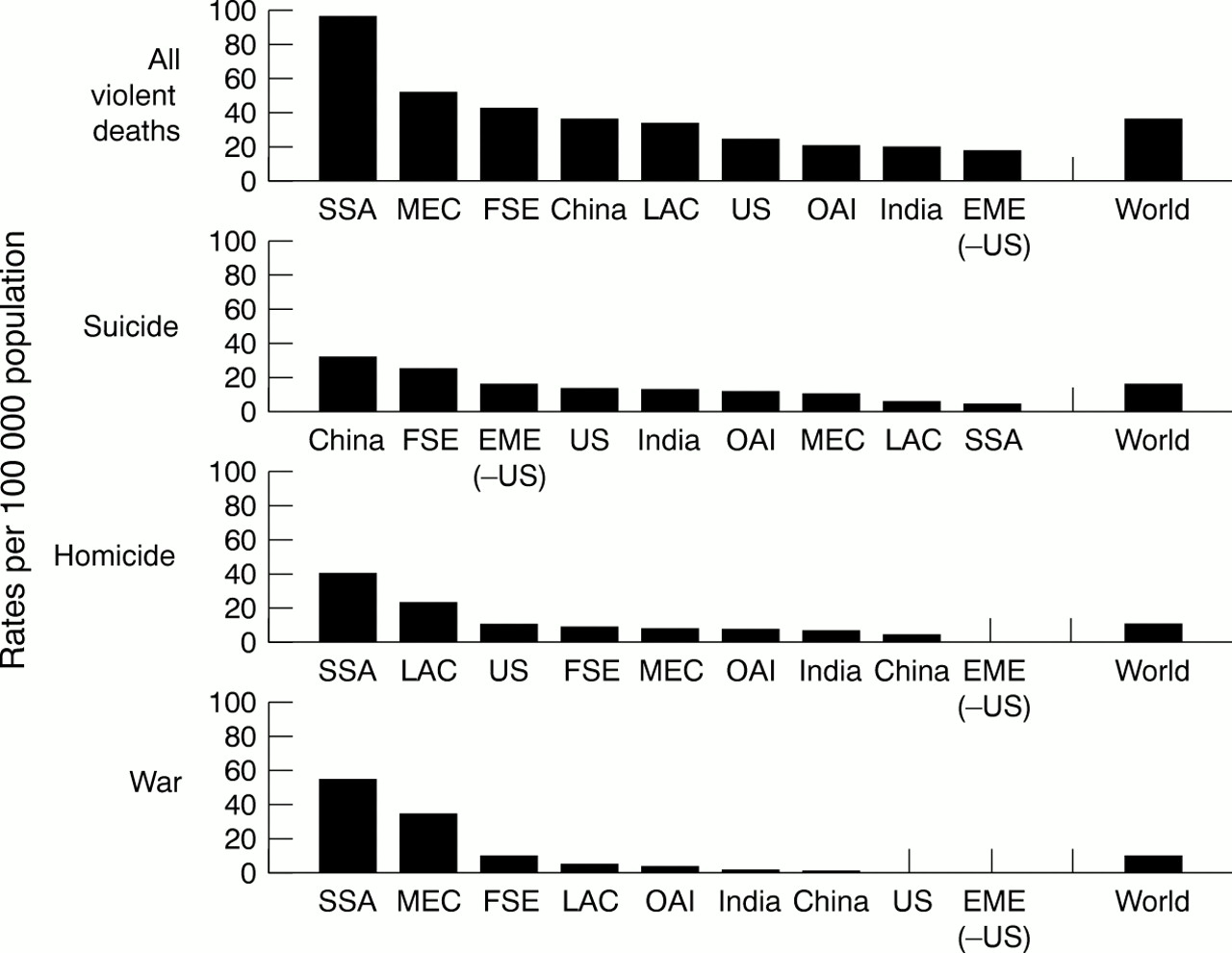
Rates of violence related deaths by region, 1990 (EME (−US) = established market economies excluding the United States; FSE = formerly socialist economies; LAC = Latin America and the Caribbean; MEC = Middle Eastern crescent; OAI = other Asia and islands; SSA = Sub-Saharan Africa).
SUICIDE
In 1990, there were an estimated 786 000 suicides (15.5 per 100 000) in the world (table 1). Overall suicide rates ranged from 3.4 per 100 000 in SSA to 30.4 per 100 000 in China. Suicide rates were highest in China and FSE and lowest in SSA and LAC.
The male to female ratio of suicides in the world was 1.5. Sex ratios for suicide were greatest in SSA (4.7), FSE (4.3), and United States (4.3) and lowest in India (1.2) and China (0.9). China is the only region where the rate of suicides was higher for females than males.
Patterns in age specific suicide rates varied by sex and across regions (fig 2). For example, the age specific suicide rate for females in the world was highest for 70+ year olds (40.0 per 100 000). The suicide rates for these elderly females were highest in China (136.4 per 100 000) and FSE (31.3 per 100 000). In addition to high suicide rates among the elderly, peaks were observed among females 15–29 years of age in China, India, OAI, and SSA. Suicide rates for females in childbearing years were highest in China (44.2 per 100 000) and India (22.5 per 100 000). In fact, the suicide rates among females in childbearing years in India, OAI (14.3 per 100 000), and SSA (3.0 per 100 000) were higher than the suicide rates in other age categories.

{kind=link}
{kind=link}
Rates of violence related deaths by sex, age group, and region, 1990 (EME (−US) = established market economies excluding the United States; FSE = formerly socialist economies; LAC = Latin America and the Caribbean; MEC = Middle Eastern crescent; OAI = other Asia and islands; SSA = Sub-Saharan Africa).
The age specific suicide rate for males in the world was highest for 70+ year olds (68.3 per 100 000). The highest suicide rates among these elderly males were in China (155.6 per 100 000) and FSE (85.7 per 100 000), the same regions that had the highest suicide rates among elderly females. In contrast to the peak in suicide rates for females in their childbearing years, male suicide rates generally increased with age.
HOMICIDE
In 1990, there were an estimated 563 000 homicides (10.5 per 100 000) in the world (table 1). Overall homicide rates ranged from 1.0 per 100 000 in EME (−US) to 44.8 per 100 000 in SSA. Homicide rates were highest in SSA and LAC and lowest in EME (−US). The male to female ratio of homicides in the world was 3.4. Sex ratios for homicide were greatest in LAC (7.8), SSA (6.2), OAI (4.9), and United States (3.8) and smallest in China (1.3), India (1.4), and EME (−US) (1.4).
Patterns in age specific homicide rates varied greatly by sex and across regions (fig 2). For example, the age specific homicide rate for females in the world was highest for 0–4 year olds (8.7 per 100 000). Among females, homicide rates for 0–4 year olds (that is, infanticide rates) were highest in China (15.5 per 100 000), MEC (15.0 per 100 000), and India (12.3 per 100 000). In addition to the high infanticide rates, there were sharp peaks in female homicide rates for 15–29 year olds in SSA (19.4 per 100 000), LAC (9.5 per 100 000), and the United States (6.9 per 100 000). Among the elderly, a unique pattern was observed in SSA where the female homicide rate was highest for women older than 70 years of age (20.0 per 100 000).
In contrast to the homicide patterns observed for females, the age specific homicide rate for males in the world was highest for 15–29 year olds (28.3 per 100 000). Among males between the ages of 15–29 years, the highest rates were in SSA (156.7 per 100 000), LAC (68.8 per 100 000), and the United States (34.1 per 100 000). In LAC, however, the peak remained high for men between the ages of 30 and 44 (67.5 per 100 000). Although male infanticide rates were generally not high in comparison with those in other age categories, the male infanticide rate in China (8.3 per 100 000) and EME (−US) (3.6 per 100 000) were higher than homicide rates in the other age categories.
WAR
In 1990, there were an estimated 502 000 war related deaths (9.3 per 100 000) in the world (table 1). Overall rates of war related deaths ranged from 52.9 per 100 000 in SSA to no deaths in the United States, EME (−US), and China. Rates of war related deaths were greatest in SSA, MEC, and FSE. The male to female ratio of war related death rates in the world is 1.3. Sex ratios for war related deaths are not vastly different for those regions experiencing war: FSE (1.3), OAI (1.5), SSA (1.4), LAC (1.5), and the MEC (1.3).
Patterns in age specific war related death rates do not vary greatly by sex in regions experiencing war (fig 2). There were an estimated 211 000 and 291 000 war related deaths among females and males, respectively. The war related death rate for females in the world was highest for 0–4 year olds (16.2 per 100 000). The highest war related death rates for these children were in SSA (57.5 per 100 000), the MEC (42.5 per 100 000), and FSE (23.1 per 100 000). War related death rates for children in MEC, FSE, LAC (7.1 per 100 000), and OAI (4.8 per 100 000) were higher than war related death rates in the other age categories. In addition to the high war related death rates for children, there were sharp peaks for women 15–29 and 60–69 years of age.
Similar to females, war related death rates for males peaked in 0–4, 15–29, and 60–69 year olds. The war related death rate for males in the world was highest for 15–29 year olds (16.7 per 100 000). The highest war related death rates for males 15–29 years of age were in SSA (97.0 per 100 000) and MEC (58.6 per 100 000). These death rates were also high for males 0–4 year olds, especially in SSA (57.5 per 100 000) and the MEC (41.5 per 100 000).
Discussion
This study describes the impact of violence related mortality on children, women, and men around the world. To our knowledge this is the first study to estimate rates of suicide, homicide, and war related deaths for the world and its major regions. The data in this paper provide an important benchmark against which to compare future global estimates of violence related mortality. These data also help to place epidemiologic patterns from national and cross national studies of violence related mortality in a global perspective by allowing us to contrast such patterns with those for the world and it's major regions. In 1990, there were an estimated 1 851 000 violence related deaths in the world, or on average 5000 people died daily as a result of violence. Suicides represented approximately 42.5% of the total violence related deaths in the world while homicide and war related deaths constituted the remaining 30.4% and 27.1%, respectively.
Suicide is predominantly a problem of older males throughout the world. The primary risk factor for suicide, particularly among older males, is depression.22 Unipolar major depression was estimated to be the fourth leading cause of disability adjusted life years lost in the world in 1990.23 Although depression is widely recognized as a risk factor, other factors such as social isolation, hopelessness, access to lethal weapons, and alcoholism play a part.22
In most regions of the world, the problem of suicide is greater for males than females. However, in China and India suicide rates among males and females were much more similar than in other regions. In fact, China was the one region of the world where the female suicide rate exceeded that of males. In China, female suicide rates peaked among women in childbearing years and elderly women, while in India suicide rates peaked in women in childbearing years. Female suicide rates may be influenced by a combination of factors including gender roles, culture, religion, and societal views toward suicide.24 The high suicide rate among females in China and India may be causally associated with gender inequality. In some regions of the world, gender inequality is reflected in cultural practices that maintain sexual, economic, and political subordination of women.25 For example, gender inequality in India may contribute to the prevalence of arranged marriages, disputes over dowries, and conflicts and domestic abuse by in-laws that, in turn, may increase the risk of suicide among females.26–28 However, although gender inequality exists in other regions of the world such as the MEC,25 female suicide rates were low. In the MEC, the Islamic religion, which strictly prohibits suicide, may mitigate the possible effects of gender inequality on the risk of female suicide.29,30 In addition, in regions where suicide is strictly prohibited, suicide may be under-reported.
In regions where the homicide rate was highest, such as SSA, LAC, and the United States, its impact was greatest for young males. Variations in these regional homicide rates may be attributed to many factors, including socioeconomic inequalities, availability of lethal weapons, and cultural beliefs and attitudes.5,31 The vulnerability of male adolescents and young adults to homicide victimization appears to be a universal phenomena.32
A troubling pattern that is perhaps related to regional variations in cultural beliefs and attitudes is our finding that the homicide rate for females was greatest for 0–4 year olds. The problem of female infanticide was greatest in China, the MEC, and India, where boys continue to be more valued than girls.25 For example, in China, the preference for sons, particularly in rural areas, where traditional cultural beliefs continue to have a strong hold,25 and the one child policy may contribute to female infanticide.33
Our findings showed that the number of war related injuries resulting in death were similar for females and males. In addition, we found that in regions where wars have occurred, children and females constitute a large proportion of war related deaths. These results are consistent with the literature which indicates that war has devastating health effects on civilians.34–37 War also impacts the health of children, women, and men by decreasing access to food, water, adequate shelter, and transportation and damaging the health infrastructures that protect populations from other negative health outcomes.34,36–38 War related death rates for specific regions and nation states may vary greatly from year to year given changes in the political climate and circumstances. Consequently, the regional patterns of war related death evident in these data for 1990 may differ greatly from those we will see in the future.
Different forms of violence may have common underlying risk factors. For example, female infanticide and suicide among females in childbearing years may be driven by the same underlying risk factors, such as gender inequality. In addition, in studies of developed countries greater availability of lethal weapons has been found to be associated with both higher homicide and suicide rates.31,39 Therefore, prevention efforts addressing common underlying risk factors have the potential to simultaneously decrease different forms of violence.
One type of violence may also be a risk factor for other forms of violence. For example, one theory suggests that war causes socialization for aggression and that socialization for aggression causes high rates of homicide.40,41 In addition, weapons remaining in war stricken regions are associated with mortality and injuries even after wars are over.42 Many of the weapons used during the wars in Mozambique, Angola and Namibia, for example, are now in the hands of criminals.43 These and other theories may help explain why in regions like SSA rates of both homicide and war related deaths are high. Prevention efforts directed at one type of violence may consequently decrease risk for other forms of violence.
Understanding of why violence related mortality rates are low in certain regions of the world can also provide clues to prevention. For example, it is important to better understand the low suicide rates observed in both SSA and LAC and the low homicide rate observed in EME (−US). Cross national research should be directed towards identifying cultural factors, aspects of social organization, and regulations or policies that may protect populations from high rates of violence.
There are several limitations that need to be carefully considered in interpreting the findings of this study. First, the sensitivity of the methods used to estimate the magnitude and impact of violence related deaths differs from one region to another. Greater confidence can be placed in data for those regions that have complete vital registration systems (the United States, EME (−US), FSE), followed by data from regions in which sample vital registration systems were used to generate estimates (China, India), and the lowest confidence placed in estimates derived from the remaining regions where complete or sample registration was not available (OAI, SSA, LAC, the MEC). The accuracy of the estimation procedures used to generate mortality data for this study should be carefully coinsidered.44 Where comparisons can be made mortality estimates from The Global Burden of Disease study agree reasonably well with previously reported estimates.44 It is difficult to assess, however, the magnitude and direction that the estimation procedures used may bias the estimates of violence related mortality reported here given the paucity of research on violence related mortality in those regions that lack complete or sample registration data. Furthermore, we lack the information necessary to place confidence limits or minimum and maximum boundaries on these estimates. Second, misclassification of causes-of-death may occur for reasons other than technical characteristics of the reporting systems. That is culture, religion, and politics may influence cause-of-death reporting. For example, misclassification of suicide is especially likely to occur in regions of the world where it is considered a cultural or religious taboo to commit suicide.45 In war stricken regions, homicides may have been misclassified as war related deaths or vice versa. Third, using global regions as the unit of analysis masks the considerable variation in the magnitude and patterns of violence related mortality that exists between nation states within regions. For example, the magnitude of homicide rates in LAC varies by at least as much as fourfold across specific nation states (for example, Argentina 4.5 per 100 000 in 1994 v Mexico 17.6 per 100 000 in 1994).11 Consequently, violence related surveillance systems are needed at a much lower level of aggregation than global regions to be useful as a guide for program and policy development at the level of the nation state.
This study was also limited in that we lacked important information about the demographic characteristics and circumstances of violent death that would have allowed for a more complete and informative description of these events. For example, the data we analyzed were not available by race/ethnicity and the age categories available for analysis did not allow us to distinguish adolescents from adults. Furthermore, circumstantial information such as whether violent deaths were associated with political persecution or terror were not available for analysis. We also lacked comparable information on non-fatal injuries associated with violence. Deaths represent only a small fraction of the injuries associated with violence and a complete description of the global problem of violence requires an understanding of the magnitude and characteristics of nonfatal violence as well. These limitations in the availability of key information also points to the need for broader implementation of surveillance systems for violent death and injury.
The contribution of violence to the global burden of health is predicted to increase unless substantial efforts are taken to remediate this problem.46 Therefore, nation states and prominent organizations across the world need to develop a global strategy to address the premature and unnecessary deaths and disabilities associated with this problem. These strategies would include: (1) implementing surveillance systems to monitor the incidence and prevalence of violence related health outcomes; (2) establishing an international network to share information and resources on prevention research and programs; (3) developing a global agenda to identify and prioritize research needs; (4) conducting cross national research to better understand risk and protective factors for violence; and (5) implementing interventions and policies that reduce the risk of exposure to violence and promote non-violence. History has shown us that humankind can reach across geographic boundaries to solve health problems. A collective effort is needed to ensure a more peaceful world for future generations.
Key points
-
In 1990, an estimated 1 851 000 people died from violence (35.3 per 100 000), representing 3.7% of all deaths occurring in the world that year.
-
Suicide was the most frequent form of violent death followed by homicide and then war related deaths.
-
Suicide rates were highest in China and formerly socialist economies, homicide rates were highest in Sub-Saharan Africa and Latin America/Caribbean, and war related death rates were highest in Sub-Saharan Africa and the Middle Eastern crescent.
-
Limitations in available data point to the need for broader implementation of surveillance systems for violent death and injury.
-
A global strategy is needed to address the premature and unnecessary deaths and disabilities associated with violence.
Appendix 1. States or territories by demographic region*
DEMOGRAPHICALLY DEVELOPED REGIONS
Established market economies (EME)
Andorra, Australia, Austria, Belgium, Bermuda, Canada, Channel Islands, Denmark, Faeroe Islands, Finland, France, Germany, Gibraltar, Greece, Greenland, Holy See, Iceland, Ireland, Isle of Man, Italy, Japan, Liechtenstein, Luxembourg, Monaco, Netherlands, New Zealand, Norway, Portugal, San Marino, Spain, St Pierre and Miquelon, Sweden, Switzerland, United Kingdom, United States.
Formerly socialist economies of Europe (FSE)
Albania, Belarus, Bosnia and Herzegovina, Bulgaria, Croatia, Czech Republic, Estonia, Hungary, Latvia, Lithuania, The Former Yugoslav Republic of Macedonia, Moldova, Poland, Romania, Russian Federation, Slovakia, Slovenia, Ukraine, Yugoslavia.
DEMOGRAPHICALLY DEVELOPING REGIONS
India
China
Other Asia and islands (OAI)
American Samoa, Bangladesh, Bhutan, Brunei Darussalam, Cambodia, Cook Islands, Federated States of Micronesia, Fiji, French Polynesia, Guam, Hong Kong, Indonesia, Johnston Island, Kiribati, Democratic People's Republic of Korea, Republic of Korea, Lao People's Democratic Republic, Macao, Malaysia, Maldives, Marshall Islands, Mauritius, Midway Island, Mongolia, Myanmar, Nauru, Nepal, New Caledonia, Niue, Northern Mariana Islands, Palau, Papua New Guinea, Phillippines, Pitcairn Island, Reunion, Seychelles, Singapore, Solomon Islands, Sri Lanka, Taiwan, Thailand, Tokelau Island, Tonga, Tuvalu, Vanuatu, Vietnam, Wake Island, Wallis and Futuna Islands, Western Samoa.
Sub-Saharan Africa (SSA)
Angola, Ascension, Benin, Botswana, Burkina Faso, Burundi, Cameroon, Cape Verde, Central African Republic, Chad, Comoros, Congo, Cote d'Ivoire, Djibouti, Equatorial Guinea, Eritrea, Ethiopia, Gabon, Gambia, Ghana, Guinea, Guinea-Bissau, Kenya, Lesotho, Liberia, Madagascar, Malawi, Mali, Mauritania, Mayotte, Mozambique, Namibia, Niger, Nigeria, Rwanda, Sao Tome and Principe, Senegal, Sierra Leone, Somalia, South Africa, St Helena, Sudan, Swaziland, Tanzania, Togo, Tristan da Cunha, Uganda, Zaire, Zambia, Zimbabwe.
Latin America and the Caribbean (LAC)
Anguilla, Antigua and Barbuda, Argentina, Aruba, Bahamas, Barbados, Belize, Bolivia, Brazil, British Virgin Islands, Cayman Islands, Chile, Colombia, Costa Rica, Cuba, Dominica, Dominican Republic, Ecuador, El Salvador, French Guiana, Grenada, Guadeloupe, Guatemala, Guyana, Haiti, Honduras, Jamaica, Martinique, Mexico, Montserrat, Netherlands Antilles, Nicaragua, Panama, Paraguay, Peru, Puerto Rico, St Kitts and Nevis, St Lucia, St Vincent and the Grenadines, Suriname, Trinidad and Tobago, Turks, and Caicos Islands, Uruguay, US Virgin Islands, Venezuela.
Middle Eastern crescent (MEC)
Afghanistan, Algeria, Armenia, Azerbaijan, Bahrain, Cyprus, Egypt, Former Spanish Sahara, Georgia, Islamic Republic of Iran, Iraq, Israel, Jordan, Kazakhstan, Kuwait, Kyrgyzstan, Lebanon, Libyan Arab Jamahiriya, Malta, Morocco, Oman, Pakistan, Qatar, Saudi Arabia, Syrian Arab Republic, Tajikistan, Tunisia, Turkey, Turkmenistan, United Arab Emirates, Uzbekistan, West Bank and Gaza Strip, Yemen.