Article Text

Abstract
Background Psychological consequences such as post-traumatic stress disorder (PTSD) are currently neglected in burden-of-injury calculations.
Aim To assess the disease burden of PTSD due to unintentional injury and compare this health loss with physical injury consequences.
Methods From literature sources, the prevalence of PTSD at four follow-up periods (<3 months, 3–6 months, 7–12 months and >12 months) was estimated. The uncertainty of the estimated PTSD prevalence was modelled by a Bayesian approach. The prevalence rates were then linked to national data on unintentional injury, disability weights and duration to estimate the incidence and disability-adjusted life years (DALY) resulting from PTSD in addition to physical injury consequences.
Results The data suggest that PTSD prevalence among injury victims decreases over time. The average PTSD prevalence at <3 months follow-up was 21% (90% credibility interval (CI) 17% to 24%) for patients presenting at the emergency department and 30% (90% CI 27% to 33%) for patients who were hospitalised, tapering down after 12 months to 4% (90% CI 3% to 5%) and 6% (90% CI 4% to 10%), respectively. These estimates translate into 191 000 (90% CI 161 000 to 222 000) cases of PTSD per year in the Dutch population (1.2%) due to unintentional injury. Including PTSD increases the non-fatal burden of disease of unintentional injuries by 53% (from 116 000 to 178 000 DALYs (90% CI 150 000 to 217 000)).
Conclusions Ignoring PTSD in burden-of-injury studies results in a considerable underestimation of the burden of injury. This may affect resource allocation and the identification of important prevention priorities.
- Disability
- psychological
- public health
- sequelae
Statistics from Altmetric.com
Introduction
Following the 1996 Global Burden of Disease study, injury researchers have used the disability-adjusted life year (DALY) in burden-of-disease and injury studies to facilitate effective and efficient policy-making on injury prevention and surveillance.1 The DALY is a metric that integrates the effect of mortality and morbidity and disability so that they can be considered at the same time. This simplifies comparison of health outcomes between subgroups of a population. A prerequisite for comparison is that the burden of disease or injury comprises a complete assessment of the health effects due to a certain cause. In previous burden-of-injury studies, long-term injury consequences such as permanent disability have been included, but with important restrictions as pointed out by Lyons et al.2 In their paper, Lyons et al present a framework that comprises the injury burden across individual, family and societal domains, including psychological consequences. So far, only physical consequences have been accounted for, whereas psychological consequences such as post-traumatic stress disorder (PTSD), depression and other maladaptive syndromes—undisputed consequences of high impact once they occur—have not previously been considered. Many studies have revealed a high prevalence of disabling psychological consequences among injury victims, and neglecting them leads to underestimation of the injury problem by health policy makers, affecting resource allocation and identification of important prevention opportunities.3–8
A common psychological problem causally related to the injury event is PTSD. PTSD may result from any event that involves an injury or threatened or actual death (of others). PTSD meets the definition of an injury sequela—that is, a pathological condition resulting from a prior injury, disease or attack. Along with its high prevalence among injury victims of all severity levels,9–12 its large effect on health-related quality of life, and the usually long-term presence of psychiatric consequences, PTSD following injury might contribute a substantial burden that is currently neglected in estimates of the burden of injury.
In this study, we aimed to:
Assess the prevalence of PTSD among patients with injury from all unintentional causes;
Estimate the disease burden in DALYs resulting from PTSD due to unintentional injury in the Netherlands and compare the resulting health loss with physical injury consequences.
Methods
Study design
A literature review was conducted to obtain data on the prevalence rate of PTSD among injury patients. In order to include patients with injuries of minor and major severity, we focused on follow-up studies of samples treated at an emergency department (ED) and/or admitted to hospital. Follow-up period is defined as the time between treatment at the ED/admission to hospital and measurement of PTSD symptoms. To estimate the prevalence of PTSD at various follow-up periods, the reported data of the studies were subdivided into four groups: <3 months, 3–6 months, 7–12 months and >12 months. PTSD prevalence was calculated for each of these follow-up periods. The uncertainty of the estimated PTSD prevalence at these four follow-up periods was modelled by using a Bayesian approach.13 The PTSD prevalence was considered as a binomial fraction in which the uncertainty was modelled as a Beta (s,f) distribution. Here, s is the number of persons who developed PTSD, and f is the number of persons who did not. Using this approach, the 90% credibility interval (CI) is similar to that estimated by conventional means, with the advantage that a full uncertainty distribution can be simulated.
As a next step, the number of patients who visited the ED due to unintentional injury in the Netherlands was obtained from registry systems. The estimated prevalence with uncertainty by follow-up moment was multiplied by the number of injury cases in order to estimate the incidence of cases of PTSD in the Netherlands. The burden of PTSD following injury was then estimated by combining these prevalence estimates with appropriate disability weights and estimates for the duration of PTSD.
Literature review
To obtain data on the prevalence of PTSD among injury patients, a literature review was conducted of published studies to date that explored PTSD among injury patients. This literature review comprised a search of the databases, Medline and PsycInfo, that was restricted to articles published in English from and including 1990 through March 2010, using the following search terms: post-traumatic stress disorder, injury, follow-up, psychiatric, psychological, incidence and prevalence. Excluded were review articles and articles on combat-related injury—injury caused by (natural) disaster or war, criminal violence, partner violence and sexual assault. The resulting articles were screened to identify those that met the predefined selection criteria. Reference lists of the included articles were also examined to identify cited articles not captured by Medline and PsycInfo. Finally, full-text articles that met the selection criteria were scrutinised to assess methodological quality. We only included studies that addressed:
Adult injury patients of all ages, both male and female;
Injury patients treated at the ED and/or admitted to hospital;
Injuries of all causes (traffic, occupation, home and leisure, sports and violence);
All types of injuries.
These studies were supplemented by further analysis of unpublished data from a published Dutch follow-up study, which measured PTSD among 1781 injury patients 24 months after visiting an ED of a hospital.14
Burden-of-disease calculation
The incidence of injury patients aged 15 years or older treated at the ED was derived from the Dutch Injury Surveillance System, a continuous registry of intentional and unintentional injuries of 17 hospitals in the Netherlands.14 Registered patients are victims of intentional and unintentional injury. This study was deliberately restricted to victims of unintentional injury (home and leisure, traffic, occupational and sport). The sustained injuries varied from minor to severe, single and multiple, and hospitalised and non-hospitalised. The estimated incidence of PTSD was calculated by combining the incidence of injury and the calculated mean prevalence of PTSD.
We calculated the mean prevalence of PTSD for patients treated at the ED and hospitalised patients separately. These were subsequently used to calculate the burden of disease due to PTSD, expressed in DALYs, in these two groups.
The DALY aggregates mortality, expressed in years of life lost (YLL), and morbidity, expressed in years lived with disability (YLD). Regarding PTSD, the mortality component of the DALY is not taken into account, as it is not associated with increased mortality. To calculate YLD resulting from PTSD, the incidence of PTSD was combined with a disability weight and duration of the condition. The disability weight is a value anchored between 0 and 1 that is assigned to living with the condition. This value reflects the impact of a specific health condition on health-related quality of life and it is commonly based on the preferences of a panel of judges. We adopted the PTSD disability weight derived from an empirical disability weights study,15 a Dutch study performed in 2006 that derived disability weights for 44 health states from a panel of laymen (n=107) recruited from the general population. The 44 health states included health states related to infectious disease, work-related health states and psychiatric health states. The procedure that was followed to derive disability weights for these health states was similar to that in the study performed in 2004 that derived disability weights for 45 permanent and temporary consequences of injury.16 The health state descriptions, or vignettes, included the disease label, disease-specific information concerning the symptoms, functional health status in generic terms, and information regarding the duration of the symptoms. The panel of laymen evaluated these vignettes using the time trade-off evaluation technique. In this study, a renewed methodology was applied that focused especially on obtaining and improving disability weights for functional losses of a temporary and complex nature. The procedures used to derive the panel study disability weights of the 2004 (injury) and 2006 (non-injury) disability weights studies have been described in detail previously.15 16 The population panel evaluated several PTSD health states, with a duration varying from 3 months, 6 months and 1 year. Some patients may have symptoms for more than a year, and, to calculate the YLD due to PTSD in this group of patients, information is needed on the maximum duration of the symptoms. The few longitudinal studies that have investigated the course of PTSD in injury patients reported a mean duration of PTSD symptoms of 6–8 years.17 18 In this study, we assumed that the group of patients with long-term PTSD symptoms (>1 year) will experience PTSD symptoms for on average 5.5 years, with a minimum duration of 3 years and maximum duration of 8 years.
The existing YLD for short-term and long-term physical consequences of injury were calculated using incidence data from the Dutch Injury Surveillance System and the set of 45 annual profile disability weights for permanent and temporary consequences of injury.16 This approach was used in the National Public Health Forecast of the Netherlands,19 which has so far neglected the impact of psychological consequences of injury on population health. This is because estimates of the prevalence of PTSD following injury and PTSD disability weights tailored to the prevalence data were not yet available when this Dutch policy document was released.
Results
Literature review
We found 125 studies that investigated the incidence of PTSD among injury patients. Of these, 101 were restricted to specific subgroups of patients, namely those who sustained injury from a specific cause (eg, traffic injury or violence), those with specific injuries (eg, burns or brain injury), specific groups of injury patients (eg, children, older or male patients) or patients with very severe injuries (eg, admitted to the intensive care unit). One study did not report PTSD prevalence. Seven studies reported on PTSD in the same sample of injury patients as other studies included in our literature review.
Sixteen studies investigated adult injury patients presenting at the ED and/or hospitalised due to unintentional injury of all unintentional causes. In addition, we were able to analyse unpublished data from a published Dutch follow-up study which measured PTSD 24 months after a visit to ED (resulting in either hospitalisation or discharge home). This brings the total number of studies to 17. Follow-up periods in these studies ranged from 1 week to 24 months, and PTSD prevalence ranged from 2% to 50%. Table 1 presents an overview of the findings of these 17 follow-up studies.
Study characteristics and methodological aspects of the 17 studies included in the review of injury patients (aged >15 years, all causes) treated at the emergency department and/or admitted to hospital and post-traumatic stress disorder
PTSD prevalence
ED treatment
The average PTSD prevalence at <3 months follow-up was 21% (90% CI 17% to 24%). At 3–6 months, 7–12 months and >12 months, the PTSD prevalence for patients treated at the ED was 12% (90% CI 10% to 14%), 9% (90% CI 8% to 12%) and 4% (90% CI 3% to 5%), respectively. Comparison of the PTSD prevalence with that of the subsequent follow-up period indicated that this decrease was significant (comparison of <3 months and 3–6 months PTSD prevalence rate: z=3.9, p<0.001; 3–6 months and 7–12 months: z=1.9, p=0.23; 7–12 months and >12 months z=5.0, p<0.001).
Hospitalisation
The average PTSD prevalence for patients admitted to hospital at <3 months, 3–6 months, 7–12 months and >12 months follow-up was 30% (90% CI 27% to 33%), 24% (90% CI 22% to 25%), 19% (90% CI 18% to 20%) and 6% (90% CI 4% to 10%), respectively. The data suggest that this decrease was significant (comparison of <3 months and 3–6 months, PTSD prevalence rate: z=2.4, p<0.001; 3–6 months and 7–12 months: z=3.8, p=0<0.001; 7–12 months and >12 months: z=15.5, p<0.001).
The PTSD prevalence for hospitalised patients was significantly higher in the first year after injury than for non-hospitalised patients (comparison <3 months: z=3.1, p<0.001; 3–6 months: z=7.0, p<0.001; 7–12 months: z=5.6, p<0.005; >12 months z=1.2, p=0.24). Figure 1 shows calculated PTSD prevalence with uncertainty limits per follow-up period.

Prevalence rate of post-traumatic stress disorder (PTSD) following unintentional injury treated at the emergency department (ED) and resulting in admission to hospital.
Burden-of-disease calculation
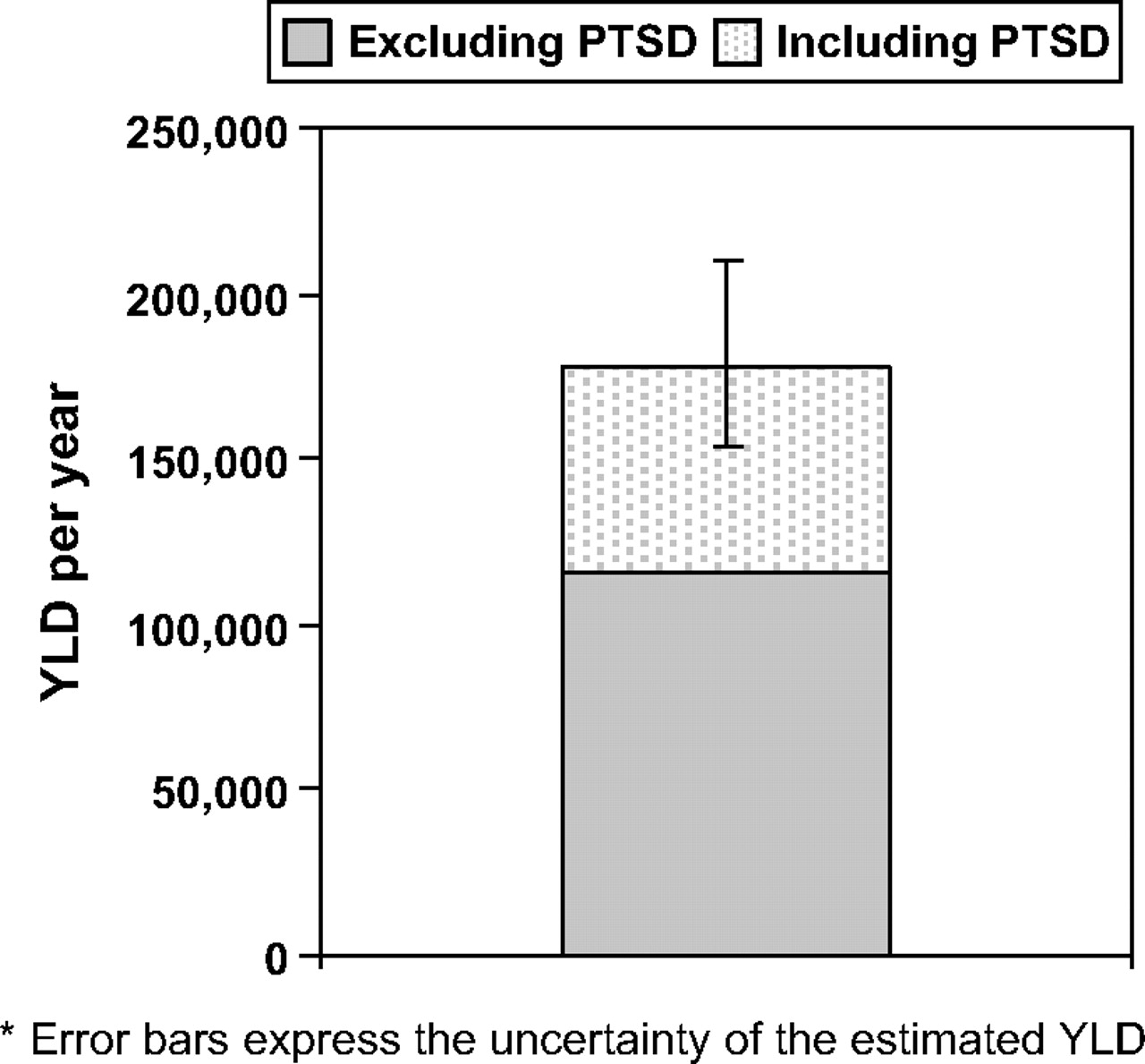
The data sources showed that, in 2007 in the Netherlands (population 16.4 million), 870 000 patients visited the ED due to unintentional injury (ie, 5% of the Dutch population).14 Of these patients, 105 000 were admitted to hospital. An estimated 191 000 (90% CI 161 000 to 222 000) of these injury patients attending the ED and/or admitted to hospital would have developed PTSD. The estimated number of YLD lost due to PTSD following unintentional injury is shown in table 2. The disease burden of PTSD following unintentional injury is in total an estimated 61 936 YLD (90% CI 34 369 to 100 759), increasing the non-fatal burden of unintentional injury in the Netherlands by 53% from 116 092 to 178 028 YLD (90% CI 150 461 to 216 851; figure 2).
Prevalence, duration and disease burden of post-traumatic stress disorder (PTSD) following unintentional injury treated at the emergency department (ED) and/or admitted to hospital (most likely estimates)
{kind=link}
{kind=link}
Total disease burden (in years lived with disability (YLD) due to physical consequences and post-traumatic stress disorder (PTSD) following unintentional injury treated at the emergency department and/or resulting in admission to hospital.
Discussion
From literature sources, we estimated that the mean PTSD prevalence at <3 months follow-up was 21% (90% CI 17% to 24%) for patients presenting at the ED and 30% (90% CI 27% to 33%) for patients who were hospitalised, tapering down after 12 months to 4% (90% CI 3% to 5%) and 6% (90% CI 4% to 10%), respectively. These estimates translate into 191 000 (90% CI 161 000 to 222 000) cases of PTSD following unintentional injury (1.2% of the Dutch population). Including PTSD as an injury burden in addition to physical consequences increases the non-fatal burden of disease of unintentional injuries by more than 50%.
Previous studies have suggested that PTSD is common among injury victims, having a large effect on health-related quality of life.10 20–23 Our study integrated these aspects using the DALY to gain insight into the disease burden associated with PTSD following unintentional injury. For this integration, little information on key aspects, such as PTSD prevalence among injury patients treated at the ED and/or admitted to hospital, the course of PTSD, and the maximum duration of PTSD symptoms, was available. Conservative assumptions about these aspects were made using the international literature. The uncertainty incurred by these assumptions was made explicit by statistical simulation.
The limited information on these three key aspects (ie, PTSD prevalence, course and maximum duration) may have affected our results. Firstly, the data used in the present study to estimate the occurrence of PTSD were retrieved from existing literature. Several follow-up studies were used for this purpose, and many of these studies used self-report questionnaires, such as the Impact of Event Scale (IES), to identify cases of PTSD. Self-report questionnaires are not designed to diagnose mental disorders according to the DSM-IV (the fourth edition of the Diagnostic and Statistical Manual for Psychiatric Disorders). As a result, cases identified with post-traumatic stress symptoms indicative of PTSD may not meet the DSM-IV criteria of clinical PTSD, and conversely. If we restrict the literature review to studies that used structured clinical interviews to identify cases of PTSD, the PTSD prevalence at <3 months, 3–6 months and 7–12 months would be 22%, 18% and 10%, respectively (hospitalised and non-hospitalised combined). These prevalences are lower than those based on studies that use self-report and structured clinical interview (<3 months, 27%; 3–6 months, 21%; 7–12 months, 18%). This implies that, by including studies that use self-report questionnaires to identify PTSD, we may have overestimated the number of cases of PTSD and consequently the burden of disease of PTSD following unintentional injury.
Secondly, regarding the duration of PTSD among injury victims, a long-term follow-up study among patients with motor vehicle traffic injury showed that the PTSD prevalence remained more or less the same at 3 months, 1 year and 5 years after the injury; five years after exposure, 10% of the subjects had persistent PTSD symptoms.24 This suggests that our assumption of a maximum PTSD duration of 8 years may be on the cautious side, underestimating the actual burden of PTSD.
We did not take into account that PTSD symptoms fluctuate over time and that, in cases of long-term PTSD, the symptoms may not have existed since day one. To allow correction for such fluctuations, detailed epidemiological follow-up data of injury patients are needed. It was not possible to correct for these fluctuations in PTSD symptoms in the present study, because some studies included in the review did not report details of the dynamics of PTSD symptoms in their study population.
Furthermore, in this study, PTSD prevalence rates derived from the literature were applied to cases seen in the Dutch Injury Surveillance system to estimate the number of PTSD cases following injury in the Netherlands. However, there are possible differences, such as severity of the injury, between cases seen in the Dutch Injury Surveillance system and the smaller number of cases included in studies from the literature. These differences may affect the risk of developing PTSD after injury. Therefore, applying the estimated PTSD prevalence rates derived from literature to cases from the Dutch Injury Surveillance may have overestimated or underestimated the number of cases of PTSD. To avoid this, we calculated PTSD prevalence and disease burden for hospitalised and non-hospitalised patients separately.
When comparing the total disease burden due to injury (YLL and YLD) with that of diseases in the Netherlands, home and leisure injuries and traffic injuries rank at number 11 and 17, respectively. Cardiovascular disease tops the list, with 339 700 DALYs, and dementia ranks number 10 with 101 500 DALYs. If PTSD is included in the burden-of-injury calculations, home and leisure injury rises in ranking to number 8, with 127 000 DALYs, and traffic injury rises to number 13, with 78 000 DALYs.
Ranking of injury among major causes of health loss would change even more if this study was not restricted to PTSD, as other psychological consequences such as depression and travel anxiety are also common consequences of injury.6 11 25 26 These findings suggest that our burden-of-injury estimates are still conservative and emphasise the importance of including psychological consequences to improve burden-of-injury estimations as well as other outcomes associated with injuries.30
However, PTSD and other psychiatric disorders that may be caused by injuries are highly prevalent in the general population.27 28 In the Netherlands, the estimated prevalence of current PTSD in the total population is 3.8%.27 This means that the estimated cases of PTSD following unintentional injury are approximately a third of the total estimated prevalence of PTSD in the Netherlands. However, new evidence has revealed that approximately half of the injury patients diagnosed with PTSD experienced symptoms before the injury.29 To unravel the intricate combinations of factors that cause PTSD and to aid in the attribution of its disease burden, more insight into the relation between injury and psychological disorders is needed. If this aspect is not addressed, the disease burden of PTSD cases may be attributed to multiple causes and consequently double counted in burden-of-disease studies.
Regarding the burden-of-injury calculation, the method used to assess disability weights is also an issue of importance. Several burden-of-injury studies used disability weights that were assessed with generic health status measures such as the EQ-5D.2 31 32 These measures allow patients to describe their health state by choosing a functional level for each generic health domain. The reported health state is then converted into a disability weight, which by definition fits within the 0–1 range. In the EQ-5D, the health profile is determined from five attributes: mobility, self-care, usual activities, pain/discomfort and anxiety/depression. If patient-reported data are used for the assessment of disability weights, the disability weights may already include (part of) the impact of PTSD. We decided to use panel-derived disability weights, which involves a layman panel evaluating health state descriptions, or vignettes. The use of these disability weights avoids the issue of double counting that arises when disability weights derived with generic health status measures are used.
Furthermore, it should be noted that, in the present study, it was assumed that PTSD prevalence rates are consistent across countries. However, there is evidence that they differ widely across countries.33 Such differences have also been found regarding PTSD among injury patients across countries. In Switzerland, Japan and Australia, low PTSD prevalence has been found, whereas in the USA much higher rates have been reported, even though the same methodology was used.6 8 23 34
Conclusions
We conclude that PTSD is a common sequela of injury and that the burden of PTSD is considerable compared with other outcomes of injury. The PTSD prevalence among injury patients declines over time, but in some patients it remains persistent. Ignoring PTSD in burden-of-injury estimates results in a large underestimation of the burden of injury. To satisfy the aspirations of burden-of-disease studies—namely identifying priorities in medical resource allocation and targeting interventions—sequelae of injury, such as PTSD, should be included, given that the evidence on the association is conclusive. Our disease-burden estimates are likely to be conservative, which further emphasises the importance of including psychological consequences to improve burden-of-injury estimations.
Implications for prevention
The burden-of-disease concept is used increasingly for priority setting in healthcare and prevention. However, calculations of the burden of injury have important restrictions, because they focus on physical outcomes only, whereas injury is associated with a range of outcomes, including psychopathological consequences such as PTSD. This study shows that neglecting psychological consequences in burden-of-injury estimations leads to a major underestimation, and this may affect resource allocation and the identification of important prevention priorities.
What is already known on this subject
The burden-of-disease concept is used increasingly for priority setting in healthcare and prevention.
Current burden-of-injury studies are restricted to physical outcomes and do not include psychological consequences of injury such a post-traumatic stress disorder.
What this study adds
Post-traumatic stress disorder is common among injury patients treated at emergency departments and/or admitted to hospital.
Including post-traumatic stress disorder in the calculations increases the number of disability-adjusted life years from non-fatal injury by more than 50%.
Neglecting psychological consequences leads to a major underestimation in burden-of-injury estimations. This may affect resource allocation and the identification of important prevention priorities.
References
Footnotes
All authors contributed to the article.
Competing interests None.
Provenance and peer review Not commissioned; externally peer reviewed.