Article Text

Abstract
Background: In New Zealand (NZ), 20% of adults report a disability, of which one-third is caused by injury. No prospective epidemiological studies of predictors of disability following all-cause injury among New Zealanders have been undertaken. Internationally, studies have focused on a limited range of predictors or specific injuries. Although these studies provide useful insights, applicability to NZ is limited given the importance of NZ’s unique macro-social factors, such as NZ’s no-fault accident compensation and rehabilitation scheme, the Accident Compensation Corporation (ACC).
Objectives: (1) To quantitatively determine the injury, rehabilitation, personal, social and economic factors leading to disability outcomes following injury in NZ. (2) To qualitatively explore experiences and perceptions of injury-related outcomes in face-to-face interviews with 15 Māori and 15 other New Zealanders, 6 and 12 months after injury.
Setting: Four geographical regions within NZ.
Design: Prospective cohort study with telephone interviews 1, 4 and 12 months after injury.
Participants: 2500 people (including 460 Māori), aged 18–64 years, randomly selected from ACC’s entitlement claims register (people likely to be off work for at least 1 week or equivalent).
Data: Telephone interviews, electronic hospital and ACC injury data. Exposures include demographic, social, economic, work-related, health status, participation and/or environmental factors.
Outcome measures: Primary: disability (including WHODAS II) and health-related quality of life (including EQ-5D). Secondary: participation (paid and unpaid activities), life satisfaction and costs.
Analysis: Separate regression models will be developed for each of the outcomes. Repeated measures outcomes will be modelled using general estimating equation models and generalised linear mixed models.
Statistics from Altmetric.com
Introduction
The overall purpose of the proposed Prospective Outcomes of Injury Study (POIS) is to (a) determine factors leading to disability following injury in New Zealand (NZ) and (b) qualitatively explore with injured New Zealanders their “lived experiences” and perceptions of injury outcome. Results will have implications for (1) improved targeting of injured people at increased risk of experiencing poor outcomes, (2) improved health and social services for people following injury, and (3) improvement of national strategies to better address barriers to, and facilitators of, good outcomes identified by injured people.
The international burden of injury
Globally, injury accounts for 9% of deaths.1 However, “…deaths due to injury represent only the tip of the injury iceberg” (p112).23 Of great importance to injured people, whānau (families) and communities is the daily experience of life after injury. After injury some people will experience a complete resumption of life as it was before injury; others will experience a life lived differently. A life lived differently is not necessarily a poorer life. Some people report life-enhancing opportunities arising as a consequence of their injury, such as the attainment of occupational or educational goals previously not available to them, or an increased sense of self-worth and belonging.4 However, others experience primarily adverse outcomes following injury and encounter barriers to living a “good life”.
The concept of disability
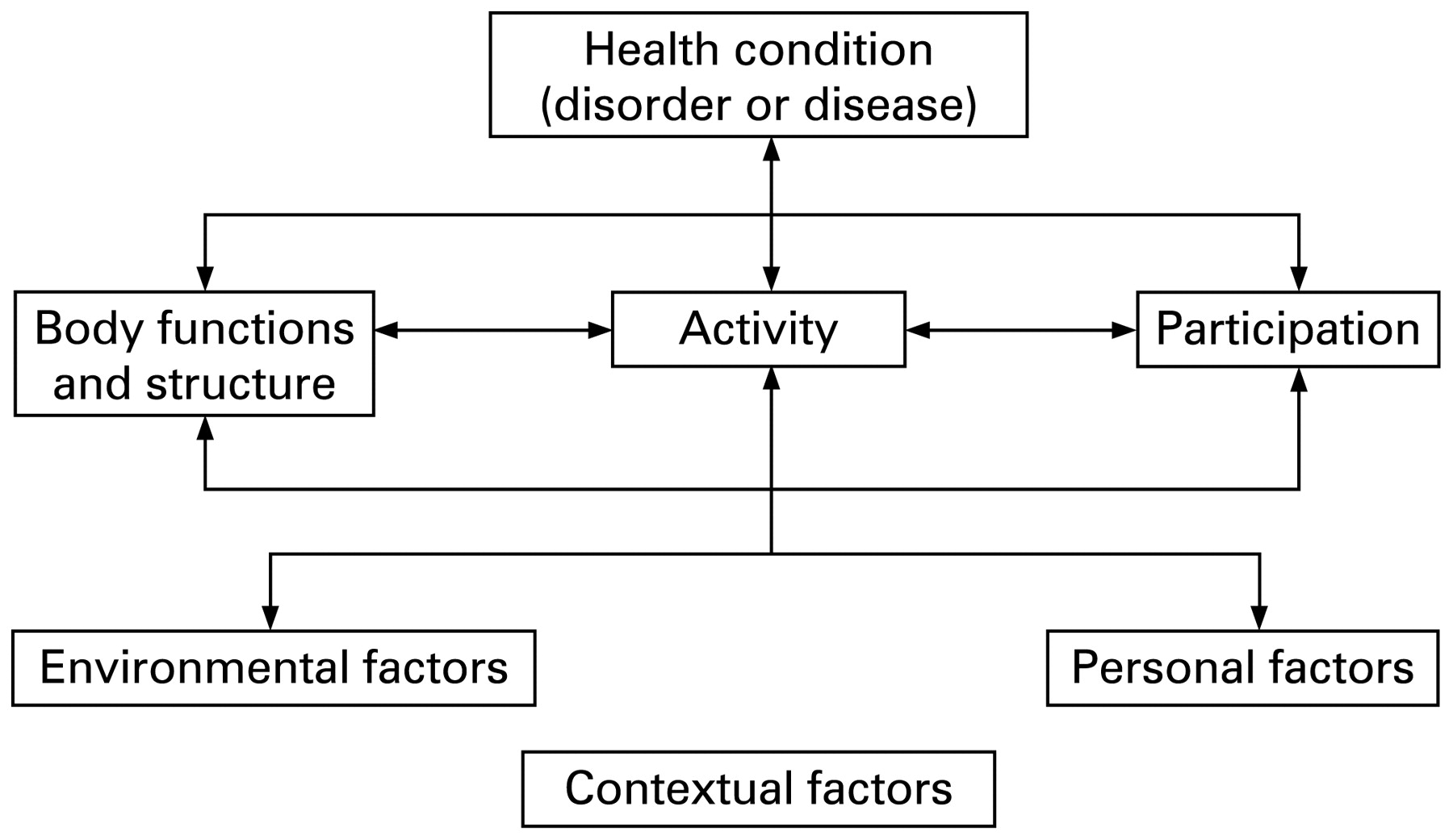
Conceptualising and measuring pre-injury “life as it was” and the “life lived differently” is complex. For injury outcome research, current concepts of “disability” provide an appropriate focus. Definitions and understanding of disability have been, and are, contested.567 In NZ, “For most of the 20th century, disability was thought to be a problem inherent in individuals” (p8).8 From the 1960s, disability was seen to arise from “…environmental barriers and attitudes that specifically discriminate[d] against people with impairments”.91011 People with disabilities helped to develop an internationally accepted model, published by the World Health Organization (WHO) in 2001—the International classification of functioning, disability and health (ICF)12 (fig 1).
{kind=link}
The World Health Organization International classification of functioning, disability and health (ICF) model.
The ICF provides a biopsychosocial health and disability framework, depicting functional impairments, activity limitations and participation restrictions influenced by the health condition (in our project’s case—injury), personal and environmental factors.13 The ICF dimensions have guided the selection of predictor and outcome measures for our project’s quantitative structured interviews and electronic data, and also themes to be explored in the in-depth qualitative interviews.
Although the ICF has been internationally commended,9131415 and increasingly used by researchers,1617 limitations have been identified. For example, the ICF does not sufficiently consider subjective experiences or quality of life.151819 In NZ it has been noted that “…Many consequences [of injury] are unable to be measured directly …, such as the loss of intimacy between spouses, or the breakdown of a family unit…”.20 To deliver important and innovative outputs, our project also includes measures of concepts beyond the ICF, such as happiness, life satisfaction and autonomy.21 And the qualitative component explores in greater depth with injured people, including Māori, their self-reported experiences, barriers and facilitators to good outcomes. Because the concept of disability is not fixed, the term “disability outcomes”, rather than “disability”, is used throughout this application.
Disability in NZ
Results from the 2006 New Zealand Disability Survey (NZDS) are not yet available; however, in 2001, the NZDS estimated that 743 800 New Zealanders (20%) were living with a disability.22 Injury was the reported cause of one-third of this disability (34%).22 This survey was cross-sectional, producing point prevalence estimates. It does not provide estimates for the number of people with ongoing disability after injury (eg, 6 months or 1 year). At a personal and family level, Statistics New Zealand and Ministry of Health surveys reveal differences in household composition, income, employment status and educational attainment between people with a disability and the general NZ population.22
Financial costs of injury
Injury is costly at both personal and societal levels; however, few studies have undertaken economic analyses of injury costs to individuals and society. Where these have been undertaken, they have tended to focus on the health system/insurer costs only23 or on specific injury types, eg, traumatic brain injury,24 or have short follow-up periods.25 Nilsen et al26 reviewed 12 cost-of-illness (COI) studies from eight different countries and found wide variation across the studies. Further, COI studies have been criticised for not taking into account intangibles such as pain and quality of life.26 One NZ study investigated the total documented costs for 15 ill or injured workers, and their families and workplaces, and found the costs since injury were $1 167 472 (average of $77 831) excluding both the loss of income borne by individuals and families and future costs to the Accident Compensation Corporation (ACC).20 ACC is NZ’s no-fault compulsory accident insurance scheme which accepts personal injury claims for physical injury and mental injury arising from a physical injury. ACC covers the cost of treatment and compensates for loss of earnings and permanent impairments. Entitlement claims largely exclude injuries resulting in less than 1 week’s incapacity or primary healthcare treatment-only claims. Entitlement claimants do not tend to be people with injuries requiring one or two visits to a primary healthcare professional only. ACC entitlement claims are for injuries serious enough to qualify for: earnings-related compensation (if too injured for paid employment for more than 1 week), home help, transportation support, or lump sum payments, etc (regardless of employment status). Referrals to ACC come from ACC-approved referrers including general practitioners, medical specialists, physiotherapists and other approved allied health professionals. (NB, ACC also insures visitors to NZ who are injured here—but visitors are not eligible to participate in our prospective project.)
In the 2004/05 year, ACC spent $1.36 billion for 164 120 entitlement claimants. Most of this ACC expenditure (67%) supported one-third of claimants with ongoing problems resulting from “old” injuries of 1 year or more.27 Of course, ACC expenditure represents only one aspect of the costs of disabling injury. Nevertheless, alone these costs provide sufficient evidence that longer-term disability following injury is a most significant issue in NZ.
Injury-related disability outcome research in NZ
In NZ, researchers and policy-makers have not been oblivious to injury-related disability. They have investigated differences in injury morbidity and disability concepts for Māori,2829 return-to-work for paid employees after injury,30 workplace injury and illness consequences,20 relationships between disability severity and work participation,3132 injury-specific outcomes,3334 and barriers to accessing appropriate services for New Zealanders with intellectual disabilities.35 Although this research has highlighted important aspects of the personal and familial costs and inequitable outcomes for injured people, it has also tended to focus on very specific issues or injury groups and is therefore not generalisable to all injury types. Alternatively, research has been cross-sectional and unable to identify causal relationships between risk factors for poor disability outcomes.
To our knowledge, only one epidemiological study of injured people has been undertaken in NZ. An Auckland case–control study followed 218 serious car crash survivors and compared their outcomes with 254 non-crash drivers after 18 months.36 Importantly, they found poorer health outcomes for crash drivers compared with non-crash drivers—even when crash drivers had not been hospitalised. However, this study used a measure of outcome (SF-36) that was not designed to measure “disability outcomes”. It was also unable, because of sample size, to consider predictors of outcome.
Injury-related disability outcome research internationally
There are a limited number of studies which have examined the factors associated with long-term outcomes after injury, time to return to pre-injury levels of functioning (eg, return to work), and effects on job and family. For example, a recent systematic review found only 10 articles on return to work after burns, despite publication of over 29 000 articles on burns in the last four decades.37 Because of space constraints, we discuss studies which (i) relate to “all” injury rather than very specific injuries (eg, spinal cord or brain injury) and (ii) identify predictors of disability outcomes.
Studies have found that ability to undertake activities, fitness and quality of life predict subsequent work ability.38 Studies have also found that younger age, more education, higher income, receipt of disability compensation, good social support, less physically demanding employment, expectations of recovery, pain, mood and sleep predict post-injury occupational outcomes.394041 These studies have all focused on paid employment outcomes. Although this is very important, there are other important dimensions of participating in society—especially for people not in paid employment. Indeed, returning to work too soon after injury can have adverse consequences for injured people.34
Few studies have considered disability outcomes outside employment.42 Studies of seriously injured people have found that sex, post-injury stress, length of stay in hospital, depression and injury characteristics predicted functional outcomes, or were associated with quality of life.43444546 Unfortunately, information about pre-injury health characteristics was limited. In Sweden, a study of 318 people with minor injuries found that self-reported recovery was predicted by educational and occupational status at the time of injury.47 A strength of this study was identification of the need to include “minor” injuries in studies of outcome; weaknesses included poor response (39%) and follow-up rates to their postal survey. A prospective study of injury outcomes has been undertaken in the Netherlands (n = 4639).48 It found that age, sex, injury, length of stay in hospital and intensive care admission were all predictors of functioning, measured by the EQ-5D 9 months after injury. This study was also somewhat limited by a poor response rate (39%) to the postal survey, failure to follow people with minor injuries, and limited measurement of pre-injury characteristics.
Summary
International studies have provided some useful insights into the potential predictors of disability following injury such as injury characteristics, health service factors, depression, stress, recovery expectations and employment characteristics. However, few studies have used comprehensive measures of disability predictors or outcomes that accord with the WHO ICF or other models of disability.49 Instead, findings have been constrained by: a focus on a narrow range of predictor and/or disability outcome variables; collection of limited pre-injury characteristics; poor rates of follow-up to postal surveys; and selective recruitment or follow-up of predominantly very serious injuries. Finally, and crucially, international research has limited applicability to NZ because of the importance of unique macro-social factors. For example, NZ has a comprehensive no-fault accident compensation scheme (ACC) to prevent injury and limit the severity of its consequences. This scheme is known to be significant in shaping injured peoples’ outcomes. This contrasts with the USA, for example, where one of the most significant determinants of return to work after injury is whether one obtains compensation or not.39 Given that acute and follow-up treatment, rehabilitation and compensation are theoretically available to all injured New Zealanders, irrespective of private insurance arrangements, the USA finding has limited significance for NZ.
POIS aims
The proposed POIS aims are: (1) to quantitatively determine the injury, rehabilitation, personal, social and economic factors leading to disability outcomes following injury in NZ; (2) to qualitatively explore peoples’ “lived experiences” and perceptions of injury-related disability outcomes.
Specific objectives
To identify injury, health and social rehabilitation, personal, social and economic predictors of disability outcomes for 2500 New Zealanders (including Māori and Pacific people)
To qualitatively explore with 30 purposively selected participants, including Māori, their lived experiences and perceptions of injury-related disability
To determine costs to individuals (n = 2500) and to society associated with injury-related disability in terms of direct and indirect costs ($) and health-related quality of life (HRQoL).
Previous research relevant to this proposal
Discussion of previous research by the applicants has been limited to injury-related disability outcomes work undertaken during a recently completed HRC Developmental Grant.
Establishing advisors to the project
Two groups of advisors have been formed: (1) “people with disability advisors” providing critical input to the project and having facilitated focus groups and pre-testing; (2) “scientific advisors” providing scientific and interpretive advice on aspects of the analysis.
Consultation with Māori
BH (Ngāti Pükenga) was an original member of the team awarded the HRC Developmental Grant. BH and SD travelled to the four regions where it is proposed to hold the study, to consult with Māori pakeke (advisors) about issues of importance for Māori regarding study design, research questions and desired outputs. It was acknowledged that injury, access to ACC and health services, and injury outcomes are problems for Māori in these regions. The potential merit of our project, making explicit the barriers to access and good outcomes, was identified. Pakeke also stressed the paramount importance of having an in-depth qualitative component running alongside the quantitative component—to get beneath the surface of key issues for Māori. There was also support for the larger quantitative component providing comprehensive empirical evidence capable of informing service providers and policy-makers—provided that sufficient Māori were recruited. To increase the Māori participation, a number of strategies were advised.
Advice: Include regions where a high proportion of the injured are Māori. Researcher response: The four regions selected will provide 20% (n = 460) Māori participants (based on last year’s regional numbers).
Advice: Pakeke-supported telephone interviews rather than postal survey for collecting information, but emphasised the need for some face-to-face interviews. Response: Budgeted for 10% of interviews to be face-to-face.
Advice: Make the interviews bilingual. Response: We will.
Advice: Appoint Māori interviewers; develop the regional workforce by appointing local Māori interviewers. Response: We will.
Provide regular meetings to support local interviewers, and where possible, appoint interviewers via Māori organisations, for additional local support. Response: We will.
Consultation with Māori is ongoing, and will be extended to other people, provider groups and organisations during the pilot study and the proposed main study.
Consultation with policy-makers and other key stakeholders
JL and SD met with officials at the Ministry of Health, Ministry of Social Development, Statistics NZ and ACC. All were supportive of the study. Personal communications from these groups stressed the need for, and value of, a high Māori participation rate and benefits of offering face-to-face interviews alongside telephone interviews.
(1) Advice: Researchers need to collect information on ethnicity according to the NZ census. Response: We will.
(2) Advice: Collect information about pre-injury disability, as people with disabilities are more prone to injury. Response: We have added questions from NZ census about prior disability to our interviews.
(3) Advice: Pacific people are also a group with access and injury outcome problems. Response: We will collect ethnicity of all participants, and have budgeted for a Pacific Masters student to descriptively analyse (with supervision) Pacific (n = 180) data. We will also appoint a Pacific interviewer.
Consultation with officials also confirmed that our project did not duplicate any current research programmes and would contribute useful data.
Focus group
SD and an advisor held a focus group (tape-recorded and transcribed) with people with injury-related disabilities. The aim of this group was to identify key issues to ask of all injured participants and to obtain advice about the method of data collection.
(1) Issue: Telephone interviews of up to 1 h are acceptable and preferable to postal questionnaires. Response: Telephone, with some face-to-face, interviews will be used to improve response rates. Interviews kept to 45 min duration.
(2) Issue: Participants need to be aware they may (i) request a postal questionnaire and (ii) that people with attention/concentration difficulties maybe interviewed in shorter “bursts” over 2 or 3 days. Response: We will.
(3) Issue: Researchers must protect participants’ confidential personal data and be able to analyse results independently. Response: We will/are.
(4) Issue: Researchers need to include questions about psychological well-being, sexuality and “positives” such as happiness/life satisfaction. Experiences with health providers, ACC and employers also need to be included. Response: We will.
(5) Issue: What about the perspectives of family/partners (also raised by pakeke)? Response: We have included open-ended questions in the interviews to allow people to raise the perceived impact on their family/whānau; and specific questions about the satisfaction with the inclusion of whānau by service providers. In-depth qualitative interviews with sub-samples of participants will allow closer exploration of this issue. Unfortunately, the cost of interviewing family/whānau of each injured participant in this first NZ prospective study of injury outcomes is prohibitive.
(6) Participants felt that motivation to participate would be increased by the offer of a $10 voucher for each completed interview. Response: We will (in line with a Cochrane Collaboration review).50
(7) Issue: Strong emphasis on the need to follow-up injured people for at least 1 year because participants reported that it is often at 1 year that support from services/organisations is reduced. Response: We will follow people for 1 year. Timeframes for data collection: 1, 4 and 12 months are also consistent with international working group recommendations for studies investigating injury outcomes.51
Support was expressed from the group for the proposed study and researchers’ interest in injured peoples’ outcomes.
Pre-testing an interview questionnaire
Interview questionnaires, informed by the developmental work and literature, were pre-tested by SD after obtaining ethical approval. Fifteen injured people participated. Despite the broad range of variables necessarily included (table 1), telephone interviews took only 40–45 min. No-one had difficulty comprehending the questions and even where individuals did not have any personal difficulty with some of the variables (eg, substance use, sexuality or psychological well-being), they reported the value of including such questions. It was suggested that participants need to be aware of support people to whom they can go if the interview raised issues for them, eg, their general practitioner or ACC case manager. Response: We will ask all participants how they are feeling at the end of the interview. We will also emphasise the importance of seeking help from professionals, family and friends if issues have been raised for people. We will have a website and 0800 number people can use to contact the researchers after the interview. Overall, people reported feeling pleased to be able to discuss their injury and related problems with an independent person, and were satisfied with the telephone interview method.
Summary measures of potential predictors and/or disability outcomes following injury
The pilot study
A pilot study is now underway; recruiting 150 recently injured New Zealanders from the four study regions to trial all the procedures for the main study. This will be completed before 1 July 2007.
Research design and methods
Design
Addressing the project aims and objectives requires a multidisciplinary research team and a pragmatic mix of research strategies. Pragmatic research accepts the “social, historical and political” context within which the research is undertaken, but does not mandate a single research epistemology.52 This project will use (quantitative) epidemiological, economic and statistical methods and analyses to identify predictors of disability following injury, and (qualitative) in-depth culturally appropriate methods and analyses to shed light on the still largely invisible “lived experiences” of injured New Zealanders. A prospective cohort design will be used for the quantitative and qualitative components. For the quantitative component, participants (n = 2500) are interviewed at 1, 4 and 12 months after injury. For the qualitative component, participants (n = 30) are interviewed in-depth 6 and 12 months after injury.
The study population
The target population is New Zealanders aged 18–64 years referred to ACC for an entitlement claim and case coordination and/or management for an acute injury (ie, excluding primary healthcare treatment-only claims). In the 2004/05 year, there were 88 068 such claimants.53
Eligibility criteria
Eligible participants will:
Have an acute injury resulting in referral to an ACC Contact Centre or Branch for case coordination or management (not including people with very minor injuries requiring primary healthcare only).
Be aged 18–64 years. (Injured children and older people are also of great interest and importance. However, to ensure a consistent set of measures and an age group where people predominantly participate in society through paid employment, we have selected this narrower age range. Also, people aged 25–64 report the greatest prevalence of disability in NZ.54)
Be NZ residents usually residing in one of four ACC regions (Gisborne, Manukau City, Otago and Southland—regions selected because of a range of rural/urban environments, ethnicities, socioeconomic status and health service providers).
People will not be eligible to participate if their injury is the result of self-harm or they are on ACC’s Sensitive Claims Register.
Recruitment
Recruitment of the 2500 participants will be from the population usually resident in one of four study regions. Participants will be recruited within 1 month of referral to ACC for an entitlement claim. Recruitment will occur over a 10-month period starting in October 2007. Recruitment via ACC is currently being piloted in our pilot study, and ACC have also offered support for recruitment to this main project. Potential (eligible) participants will be randomly selected by our research team at Injury Prevention Research Unit from a list of anonymous encrypted ID numbers sent by ACC. We will then send back to ACC the selected IDs, and ACC will send out a study information sheet to these selected potential participants on our behalf. Written informed consent from all participants will be obtained before any interviews or electronic data collection occurs.
Eligibility criteria and the method of recruitment are consistent across the POIS project’s quantitative and qualitative components. However, because the methods vary, they are presented separately.
Quantitative component methods and analysis
Primary risk factors
We will collect data about a broad range of pre-injury and post-injury risk factors likely to influence disability outcomes. In addition to considering the literature, our developmental work and consultation has identified factors of relevance to the NZ context, including access to service providers, racism and satisfaction with service providers and ACC.555657Table 1 summarises (1) WHO ICF dimensions and variables to be collected and broader concepts located outside the ICF model, (2) instruments to measure those variables and disability outcomes and (3) the method of collection (structured interview or electronic data).
We have adopted a pragmatic approach between selecting the most comprehensive measures of possible predictors and outcomes and the need to limit the timeframe to the 45 min interview. For example, we will include a brief measure of HRQoL—the EQ-5D (recommended, and increasingly used, in studies of injury outcome)485158—rather than longer measures (eg, the SF-36).
Space does not allow us to justify the inclusion of all the measures summarised in table 1 beyond the discussion of variables and specific questions outlined above. Briefly, key outcome measures include the short-form WHODAS II—a measure developed by WHO specifically to measure disability and health according to their ICF model.61 Along with the EQ-5D, the WHODAS is recommended for inclusion in studies of injury outcome by an international working group.51 As mentioned, other measures include the EQ-5D, a five-question instrument evaluating overall health status (or HRQoL), which relates to the ICF dimensions of functioning (including pain) and activities.59 The EQ-5D allows the formulation of an overall summary HRQoL (utility) “score” (from scores developed for New Zealanders, including Māori).60 Such a summary measure has certain advantages over other (longer) measures, such as the SF-36, which describe health status along distinct dimensions only. We have also included a global measure of overall self-perceived health status and health change over the past year from the SF-36. As table 1 indicates, some of the measures of “outcome” will also be included as “predictors” in our analytical models. For example, HRQoL as measured by the EQ-5D is one of the important outcomes that we will be examining. However, HRQoL will also plausibly be part of a model predicting disability as measured by the WHODAS II.
Primary research hypotheses
A number of research hypotheses will be investigated as indicated by the objectives and the factors identified by the consultation, focus group and pre-testing. The primary hypotheses to be investigated are as follows.
People with poorer pre-injury (eg, self-efficacy, health, mood, social support, socioeconomic), injury (severity and type) and immediate post-injury (eg, health and social services, socioeconomic, pain, health) characteristics are more likely to have poor disability outcomes at 4 months.
People with poor disability outcomes 4 months after injury will have an increased risk of poor disability outcomes 12 months after injury.
For people in paid employment, those with lower levels of pre-injury job satisfaction, job security, control and support, lower occupational status, and higher levels of job demands will have an increased risk of poor work-related disability outcomes after injury than people with more advantageous working conditions.
For injured Māori, variables relating to outcome will include access to services, health service providers, experience of racism,5657 and providers’ familiarity with Māori tikanga (culture).
Data collection
To minimise the research costs and loss to follow-up, quantitative data (table 1) will be collected primarily by structured telephone interviews and routinely collected electronic injury data.
Structured telephone interviews
Participants will be interviewed by trained interviewers, 1, 4 and 12 months after injury. There will be 5–10 interviewers depending on the number of interviews being completed in each year of the study. Interviewers will be located in each of the four project regions. The budget allows 10% of interviews to be undertaken face-to-face to ensure sufficient Māori participation (although this may also facilitate some Pacific and Pākehā participation). Data will be entered directly into a computer by the telephone interviewers for secure electronic transfer to a University of Otago database. Pre-testing shows the interviews will take 40–45 min. All participants will receive a $10 voucher in acknowledgement of their time for each completed interview. Table 1 summarises the key variables collected via the structured interviews. Pre-injury characteristics are collected at the baseline interview (1 month after injury) along with injury and immediate post-injury variables. Additional data about health and social service utilisation and direct costs are available from electronic injury data sources.
Electronic data from ACC
These will include the referring professional’s diagnosis, nature, cause and type of injury, date of injury, prior injuries to same or different parts of the body, nature and duration of any ACC support provided (case management, health treatments and earnings-related compensation information). Data will be collected at the end of the study follow-up period.
Electronic data from New Zealand Health Information Services (NZHIS)
These will be collected if the injured participant was admitted to hospital as a result of their injury at any time during the 12-month project follow-up period. NZHIS data will include ICD-10 diagnosis, injury-related procedure codes, and dates and length of stay in hospital. Members of the research team are extremely familiar with both electronic databases.
Data analysis
Descriptive analyses of variables of interest (eg, proportions of people in different age groups, sex, ethnicities and regions) will be performed. The main analyses will be separate linear or logistic regression analyses, undertaken for each of the outcomes of interest. These models will look at the direct effects of the postulated predictors on the outcomes, after adjustment for confounders and mediators. Predictors in these models will include variables from each of the domains that might be expected to influence the outcome, eg, socioeconomic, injury severity, personal factors, psychosocial factors, job and skill factors. It is expected that many of these variables will have different effects in subgroups of subjects, so many of these models will have interaction terms included. Some of the predictor variables will be continuous, and, if their relationship with the outcome is not linear, they will be transformed by using fractional polynomials.
When considering the outcome at more than one follow-up point, these models will be extended to cope with repeated measurements, so will be mixed models, general estimating equation models, and generalised linear mixed models depending on the exact situation. We anticipate that there will be complex pathways and interactions between some of the variables.11 Therefore, in secondary analyses we will explore some of these by examining the direct and indirect effects of variables on the outcomes using structural equation models.
We will estimate the personal, health sector and ACC costs of injury-related disability. Data on participants’ financial costs associated with their injury-related disability will be appropriately aggregated and extrapolated to derive estimates of these financial costs for NZ as a whole. Analysis will also address the acknowledged deficit of COI studies by incorporating the HRQoL burden of injury through derived estimates of HRQoL quality-adjusted life years lost and regained.60
Potential sources of error
Selection bias
There is a risk that injured people who consent to participate in the study will differ from non-participants, introducing bias. We have provisional approval from ACC to collect information about certain characteristics of the non-participants, including age, sex, region they live in, date of injury, injury site/cause and severity, and, if employed, occupation. This will enable us to compare participants and non-participants on a range of variables. In the same way, we will also assess any differences in loss to follow-up, to be accounted for in the interpretation of results. As part of our current pilot study, we are seeking advice from injured people as to how we might increase participation rates and minimise loss to follow-up.
Measurement bias
Recall bias is a potential source of error, particularly in relation to measurement of pre-injury status. We have sought to minimise this by collecting pre-injury information within 1 month of the injury event. Collection of health and disability outcomes, costs and health service utilisation data is also limited to a 30-day recall period to reduce recall bias. The prospective study design minimises recall bias for other factors. Misclassification of outcome data is a possibility, as the study has no control over coding secondary datasets (ie, ACC, NZHIS). For ACC, there are financial incentives, which help to ensure that the data are of high quality (eg, ACC would not be paying earnings-related compensation for those who return to work). Similar comments apply to NZHIS (eg, hospital reimbursements for days’ stay). Further, Injury Prevention Research Unit staff have recently completed a study which shows that the quality of NZHIS coding is high.62
Confounding
Information will be collected on possible confounders (eg, comorbidity and prior health status), and analytical methods will be used to control for these factors.
Generalisability
Significant relationships between risk factors and outcomes of interest are likely to apply to most subpopulations of injured people, and, although the size of the effects may differ, the direction of effect is likely to remain the same.
Sample size and power
To produce stable estimates of coefficients in regression, models require at least 10 cases for every included variable for linear regression and 10 cases with the outcome for logistic regression. So with binary outcomes, such as return to work or normal activities, we require 10 people not achieving this for each variable (binary or continuous) that is included in the model. It is generally accepted that about 4 times as many cases are needed to detect an interaction as are required to detect a main effect. Thus for two variables and their interaction, at least 60 cases are required for stable estimates. If we assume that 10% will not have returned to work or normal activities at any follow-up point, then the inclusion of 2000 subjects in the model (200 failures) would allow six variables and their two-way interactions to be included in the model before uncertainty arose about the estimates. We expect at least this many variables in most models. With linear regression, many more variables would be allowed in the model, and this would give more scope for examining interactions and more complex relationships. Thus 2000 people would be a minimum for many of the interesting models that will be used to give stable estimates of the coefficients. Allowing for a conservative 80% follow-up rate over 1 year means at least 2500 people need to be interviewed at baseline. We will actively follow participants (using alternative named contacts if people move and a website for study updates) and aim for a 90% follow-up rate over the 12 months. Feedback from stakeholders and the developmental focus groups indicated that the $10 voucher per completed interview would be appreciated and would help to increase participation and follow-up rates.50
On the basis of entitlement claimants in each of the study regions for the last financial year, we anticipate recruiting at least 460 Māori and 180 Pacific participants. This would give at least 80% power to detect statistically significant differences in proportions of 8% or more between Māori and non-Māori and 12% or more between Pacific and non-Pacific groups.
Qualitative component methods and analysis
The qualitative approach
As mentioned above, the aim of the qualitative component is to describe the lived experiences of New Zealanders with injury-related disability outcomes. Qualitative methods allow a more in-depth (rich) description and examination of the factors impacting on outcomes following injury. Although some research has considered the experiences and outcomes for people following injury, as with much of the quantitative research on injury-related disability outcomes, this has focused on particular service provider issues and specific types of injury and has been cross-sectional in nature or not necessarily relevant to NZ. To locate people’s experiences within a NZ context—and to be focused on the issues as experienced and “lived by” the participants—a phenomenological and collaborative story-telling approach has been selected.46364
Participants
We intend to recruit a subsample of at least 30 participants from the quantitative component of the study to participate in in-depth qualitative interviews: 15 Māori from the Ngāi Tahu takiwā (tribal region) and 15 non-Māori. (Māori participants will not necessarily be of the Ngāi Tahu iwi (tribe).) Purposive selection will ensure that we include people from a range of ages, sexes, injury types, households, geographical areas, service providers, and socioeconomic and employment status. The lived experiences and outcomes of every injured person are important. However, our particular emphasis upon the experiences and outcomes for injured Māori reflects our commitment to the Treaty of Waitangi and our understanding that a qualitative epistemology is appropriate for research with Māori. Furthermore, consultation with Māori has identified the need for rigorous empirical Māori data to support policy improvements for Māori and to improve cognisance regarding Māori perspectives towards disability concepts,29 and also to identify the particular obstacles that Māori are known to experience in accessing appropriate and timely services and attaining good outcomes.
Methods
Qualitative data will be collected from at least two in-depth face-to-face interviews, 6 and 12 months after injury. (Using the phenomenological and interpretive approach, people will be encouraged to contact the interviewers between the 6 and 12 month interviews if they have additional experiences to report.) Participants’ and, as appropriate their whānau, post-injury stories will be followed for 1 year after injury. (Feedback from Māori pakeke (advisors) is that the interview methods need to be flexible enough to include whānau members’ perspectives if the participants feel this is appropriate, meaning more than 15 Māori participants may be included.) In-depth interviews will, with participants’ consent, be tape recorded and fully transcribed.
Instead of a structured interview format, which is typically prescriptive, phenomenological story-telling allows participants to raise issues of greatest importance to them.6566 A phenomenological approach may therefore allow us to understand and describe alternative disability concepts located outside the WHO ICF model.18 However, there are certain themes we wish to explore in the qualitative interviews. If these themes are not spontaneously raised in the course of the interviews, participants will be prompted at the end of their stories. The key themes, informed by the literature and by our consultation, focus group and pre-testing include the story of the injury itself (cause, impact and trajectory), the impact on family/whānau/others, work (positives and negatives), costs (psychosocial and financial), spiritual supports, racism, ease of access to health services, satisfaction with health/ACC and social services and professionals, barriers encountered, strategies for overcoming these, and the facilitators of good outcomes.
Qualitative analysis
The analytical framework is interpretive and narrative.6467 There is debate in the literature about the advantages of exclusive adherence to participants’ verbatim accounts versus the benefits of shared (researcher–participant) interpretation, understanding and meaning. Our project will follow the approach outlined by Bishop6368 of sequential interviews and shared construction of meaning between researchers and participants. Māori and non-Māori strands of the qualitative component will be analysed separately to ensure that Māori results have primary importance to, and for, Māori.69 If important shared themes emerged across the two arms of the qualitative component, a subsequent joint analysis may be undertaken if appropriate.
POIS overall data management and storage
All personal identifiable study information will be kept in a locked filing cabinet accessible to study investigators only. Electronic data from ACC/NZHIS will be stored according to agency protocols.
Relevance to health
This project’s relevance to health is demonstrated by strong links to key NZ health strategy documents. For example, the project directly relates to the New Zealand Disability Strategy (NZDS, 2001) Objective 1 (to encourage and educate for a non-disabling society), by acknowledging that disabled people are experts of their own experience (rather than relying on perspectives of clinicians or other providers). Other examples include the project’s examination of whether or not injured people with disabilities: experience the same employment conditions, rights and entitlements as everyone else; have an adequate standard of living; receive respectful treatment from government departments; receive quality information; feel at the centre of service delivery; have timely access to services. The project also directly relates to the HRC Injury, Impairment, Rehabilitation and Disability Strategy by: (i) using the internationally accepted WHO ICF model for the study data collection, including social and environmental factors; (ii) empirically examining a crucial information gap that exists in NZ about the disability outcomes of injured New Zealanders; (iii) contributing to the identification of strategies for “eliminating or reducing the likelihood of adverse injury-related consequences”. Crucially, to identify strategies for improving post-injury outcomes, we first need to know where the barriers to good outcomes lie. This first prospective study to identify predictors of outcomes for New Zealanders will directly address this knowledge deficit—comprehensively (through the quantitative component) and in rich detail (through the qualitative component).
Relevance to Māori health outcomes
Injury is an important issue for Māori.28297071727374 Personal communication from ACC, Ngāi Tahu Research Consultation Committee and pakeke confirm that: (1) injury, access and outcomes for Māori are of concern; (2) more information on barriers to access and good post-injury outcomes for Maori is a research imperative. This project has a strong Māori component evaluating disability barriers to, and facilitators of, positive outcomes for Māori. It uses methods acceptable to Māori and includes methods for collecting participants’ perceptions about the level of inclusion of their whānau by service providers. Importantly, this study acknowledges both the Treaty of Waitangi and He Korowai Oranga (2002) by adhering to the Treaty principles (derived from the Treaty Articles) of: (1) partnership (Māori co-investigators contributing to study design, methods, data collection and analysis); (2) participation (consulting with pakeke and groups in the proposed study regions and adopting their recommendations; contributing to local workforce development by employing Māori interviewers in each region of the study); (3) protection (the research team intends results to have a positive impact on health outcomes for injured Māori and their whānau; interpretation of results for Māori undertaken by Māori investigators). The project, taking on board as it has advice from pakeke and senior Māori officials, also relates closely to Ngā Pou Rangahau Hauora Kia Whakapiki Ake Te Hauora Māori (2004) and Vision Mātauranga (2005), by providing information of direct relevance to Māori and their communities about barriers to access, examples of service and ACC provider strengths (and weaknesses), and the quality of life outcomes for Māori after injury.
Dissemination of results
An abstract from the developmental work has been submitted to a National Conference on Rehabilitation for consideration, and a paper is now being prepared for journal submission. Results from the main study will be shared with study participants by postal lay summaries and the project website. Results will also be disseminated by, and discussed with, pakeke, Māori and Pacific providers, organisations and stakeholders—by face-to-face presentations and written reports. Results will be published in national and international peer-reviewed journals and presented at conferences.
REFERENCES
Footnotes
Funding This study is funded by the Health Research Council of New Zealand and the Accident Compensation Corporation, Wellington, New Zealand.
Competing interests None.
Provenance and Peer review Not commissioned; not externally peer reviewed.