Article Text

Abstract
Objective: To investigate if child development has a role in unintentional poisoning, by describing the pattern of hospitalization due to unintentional poisoning in children aged 0–4 years in New South Wales by single year of age and then assessing the stability of the age-specific pattern found when analyzed by sex, remoteness of residence, and socioeconomic status.
Design: Retrospective descriptive study.
Setting: New South Wales hospitals from 1994 to 2005.
Participants: Children aged 0–4 years in the New South Wales Department of Health Inpatient Statistics Collection.
Main exposure: Hospitalization due to unintentional poisoning.
Main outcome measures: Hospitalization rates by single year of age and single year of age by three covariates: sex, remoteness of residence, and socioeconomic status.
Results: Children aged 1–3 years had the highest rates of hospitalization due to unintentional poisoning, and this pattern persisted over time. The same age-specific pattern was seen for both boys and girls, but rates were significantly higher for boys than girls at age 3 years (RR = 1.46, 95% CI 1.31 to 1.62). The age-specific pattern persisted when the covariates remoteness of residence and socioeconomic status were controlled for.
Conclusion: The age-specific pattern of hospitalization for unintentional poisoning by single year of age was found to be stable when analyzed over time and by sex, remoteness of residence, and socioeconomic status. This finding provides strong evidence for the role of a child’s development in an unintentional poisoning event.
Statistics from Altmetric.com
Unintentional childhood poisoning is a serious public health problem worldwide.1 Children aged 0–4 years are often analyzed together as a group for unintentional poisoning risk for statistical purposes. However, these children are quite different in terms of their physical, cognitive, and affective abilities, and treating this cohort as a homogeneous group may not be appropriate.
In terms of development, the average 13-month-old child is ∼2 ft tall, has well-developed fine-motor skills, and may already be walking well.2 He/she is also beginning to understand that an object still exists even after it is put out of sight, with complete object permanence usually developing between 18 and 24 months of age.3 Consequently, an average 1-year-old child has the physical ability to move around and manipulate objects and may have the cognitive ability to remember the location of an object.2 However, they will not be able to stop themselves from accessing it because the precursors of self-regulation do not begin to develop until around age 18 months, and the ability to self-regulate behavior (without external help) does not emerge until around age 36 months.4
In summary, many of the physical, cognitive and affective developmental phases have not begun in children <1 year of age, but should be well developed by age 4 years. As a result, children may be more or less at risk of a poisoning event, depending on their “progress” in these three areas. This suggests that children aged 0–4 years may experience different levels of poisoning risk as a result of their development.
The purpose of this paper is to investigate if child development plays a role in unintentional poisoning. This will be achieved by describing the pattern of hospitalization due to unintentional poisoning in children aged 0–4 years in New South Wales (NSW) by single year of age (SYA) and then assessing the stability of the age-specific pattern found when analyzed by sex, remoteness of residence, and socioeconomic status.
METHOD
Data sources
NSW population-based hospitalization data were obtained from the NSW Department of Health (NSW Health) Inpatients Statistics Collection for 1994 to 2005.5 The hospitalization data from January 1994 to June 1998 were coded using the International Classification of Disease, 9th Revision, Clinical Modification (ICD-9-CM)6 and from July 1998 to December 2005 using the International Classification of Disease, 10th Revision, Australian Modified (ICD-10-AM).7 Data from July to December 1998 were also back-coded to ICD-9-CM,5 and hospitalizations during this time period were analyzed by the ICD-9-CM codes assigned, for continuity with the first half of 1998.
Annual age- and sex-specific population estimates for NSW and NSW statistical local areas as at 30 June were obtained from the Australian Bureau of Statistics through NSW Health for 1994–2005.8 The 2001 estimated residential population by SYA for Australia was also obtained from the same source and used as the standard population.8
Inclusion criteria
Cases of hospitalization for unintentional poisoning in children aged 0–4 years were identified using the following criteria:
NSW resident admitted to hospital between January 1994 and December 2005;
an external cause code assigned in the ICD-9-CM range for poisoning (E850–E869.99) or the ICD-10-AM range for poisoning (X40–X49.99), indicating an unintentional poisoning;
a diagnosis code assigned in the ICD-9-CM range for poisoning (960–989.99) or the ICD-10-AM range for poisoning (T36–T50).
Records were analyzed by the date of admittance, and hospitalizations relating to transfers or statistical discharges were excluded in an attempt to partly eliminate “multiple counts”. There were 8472 unintentional poisoning hospitalization cases ultimately identified for analysis.
Data analysis
Annual hospitalization rates for 1994–2005 were calculated by SYA and by SYA and sex. Hospitalization rates for the group of years 1994–2005 were calculated for SYA and two covariates, sex and socioeconomic status. Socioeconomic status was determined using the five categories of the Socioeconomic Indexes for Areas (SEIFA) - Index of Relative Socioeconomic Disadvantage (ie, most disadvantaged, 2nd, 3rd, 4th, least disadvantaged). Hospitalization rates for the group of years 1998–2005 were also calculated for SYA by remoteness of residence, using the five categories of the Accessibility/Remoteness Index of Australia (ARIA) (ie, metropolitan, inner, and outer regional and remote/very remote (combined because of small numbers)). Further information on SEIFA and ARIA is available elsewhere.9–12
All age-standardized rates of hospitalization due to unintentional poisoning were calculated directly using the estimated Australian residential population as at 30 June 2001 as the standard population. 95% CIs were also calculated, assuming a Poisson distribution.13
Negative binomial regression analyses were used to determine the risk ratios (RRs) of the various age groups (<1, 1, 2, 3, 4) and age groups by sex, socioeconomic status, and remoteness of residence. Different models were fitted with counts of hospitalizations as the outcome variable and age group and sex, remoteness of residence, or socioeconomic status as covariates with the estimated population as the offset. A significance level of 0.05 was used for inclusion of both main effects and main effect interactions in the final models. Analysis was performed using SAS V8.02.
RESULTS
SYA and sex
Boys and girls exhibited the same age pattern for rates of hospitalization due to poisoning for 1994–2005, with rates increasing from age <1 to age 2 years and then decreasing to age 4 years (fig 1). Negative binomial regression analyses showed that the RRs increase from age <1 to age 3 and decline for age 4 years when boys are compared with girls by SYA. Only RRs for boys and girls aged 3 years exhibited statistically significant differences (RR = 1.46, 95% CI 1.22 to 1.74).
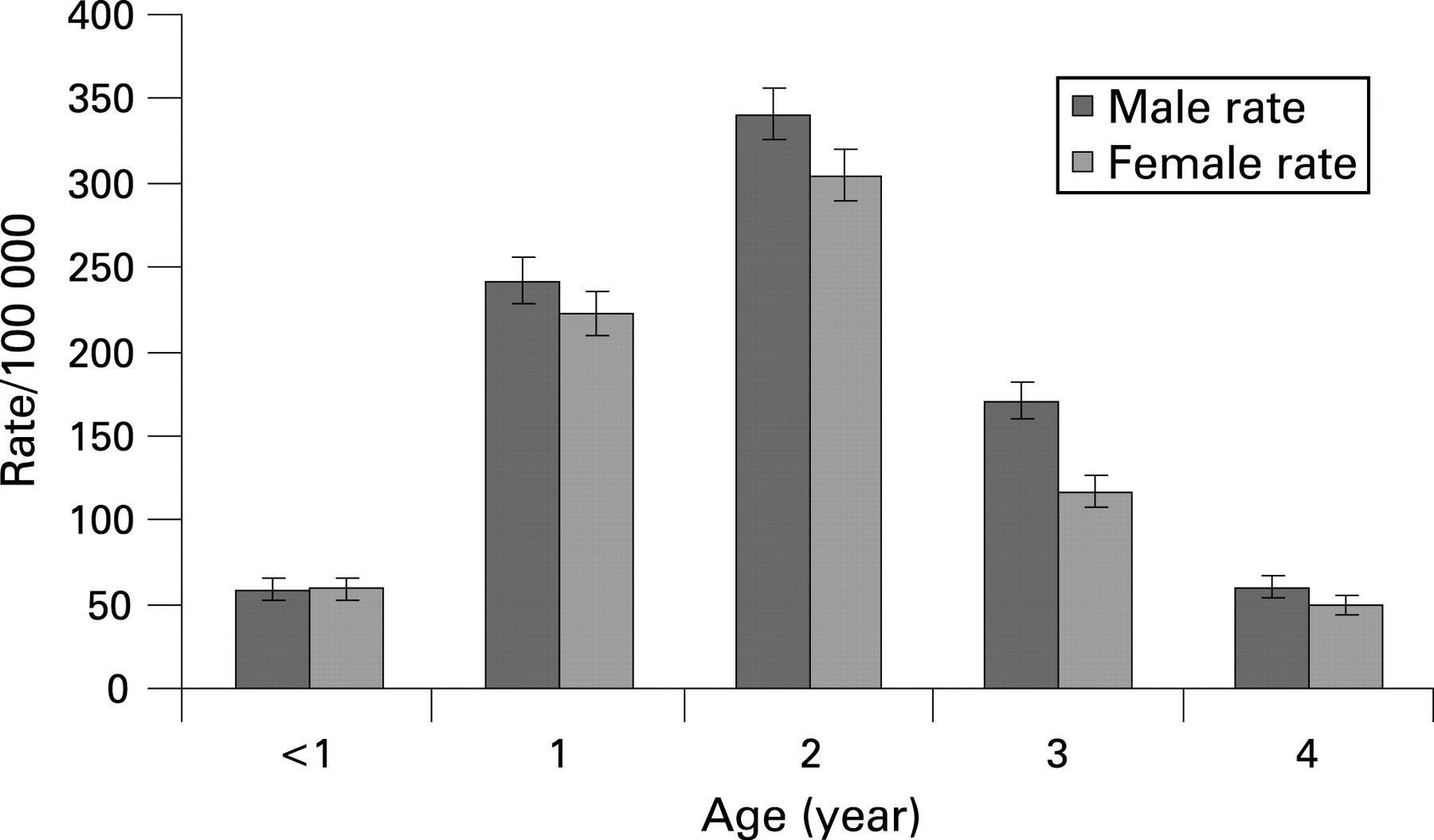
Annual hospitalization rates by SYA from 1994 to 2005 followed the same age pattern seen in fig 1. The RRs of being hospitalized for an unintentional poisoning event for children aged 1, 2 or 3 years were many times higher than for children aged <1 year and also statistically significant with 95% CIs (age 1, RR = 4.0, 95% CI 3.6 to 4.4; age 2, RR = 5.5, 95% CI 5.0 to 6.1; age 3, RR = 2.5, 95% CI 2.2 to 2.7). Children aged 4 years had a lower RR than children aged <1 year, but the RR was not statistically significant (RR = 0.94, 95% CI 0.83 to 1.06).
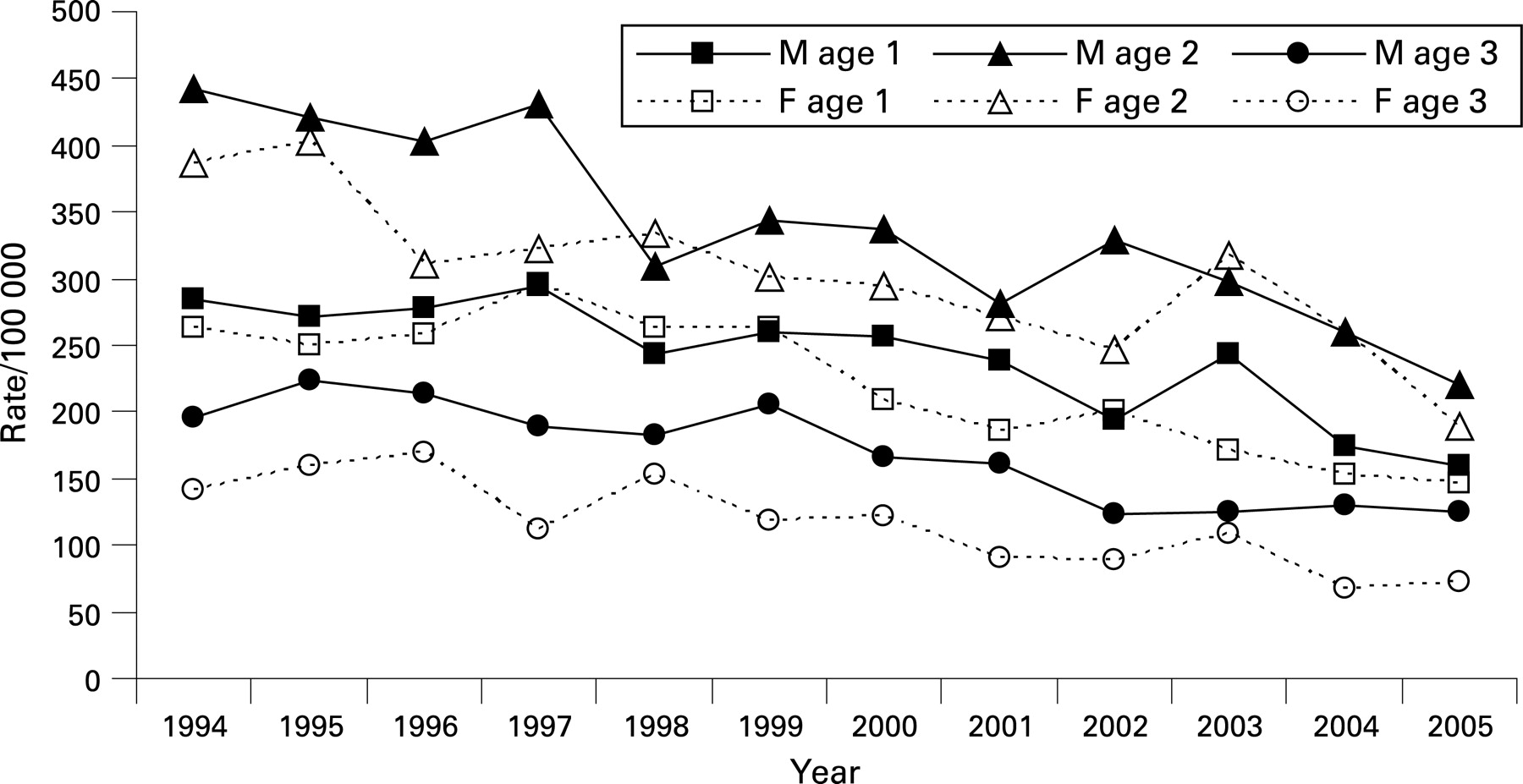
There were increasing differences in hospitalization rates over time between boys and girls aged 1, 2 and 3 years (fig 2). Children aged 1 year had similar rates of poisoning for most years from 1994 to 2005, regardless of sex (M/F age 1, RR = 1.09, 95% CI 1.00 to 1.18). Children aged 2 years showed signs of a greater difference in hospitalization rates between the sexes for most years (M/F age 2, RR = 1.12, 95% CI 1.04 to 1.20). Finally, girls aged 3 years had significantly lower hospitalization rates for poisoning than boys of the same age for all years from 1994 to 2005 (M/F age 3, RR = 1.46, 95% CI 1.31 to 1.62). In comparison, the annual hospitalization rates for girls aged 3 years were much closer to the rates for children aged <1 and aged 4 years.

{kind=link}
{kind=link}
Remoteness of residence
The age pattern for hospitalization rates due to poisoning from 1998 to 2005 was the same as in fig 1 for all ARIA categories of remoteness, with one exception. For children living in remote/very remote ARIA areas, those aged 1 year had the highest rate, but the rate was not significantly different from that for children aged 2 years. Negative binomial regression showed that children aged 1–3 years had RRs that were many times higher and also statistically significant with 95% CIs compared with children aged <1 year living in all ARIA categories of remoteness except remote/very remote areas (table 1).
Socioeconomic status
The age pattern for hospitalization rates for poisoning from 1994 to 2005 was the same as in fig 1 for all SEIFA categories of economic disadvantage. Negative binomial regression showed no association between age and SEIFA category, but there was an association between sex and SEIFA category. The RR of being hospitalized for an unintentional poisoning event for boys compared with girls was statistically significant for statistical local areas categorized as being the 2nd, 3rd, or 4th highest in terms of relative socioeconomic disadvantage.
DISCUSSION
This study found that children under the age of 5 were not a homogeneous group in terms of their risk of unintentional poisoning. Children aged <1 year and 4 years had very similar levels of risk, which were much lower than those for children aged 1–3 years. Children aged 2 years were most at risk, followed by children aged 1 year, and then children aged 3 years. The same age pattern was also found in an analysis of SYA over time, indicating that the factors that put children aged 0–4 years at increased risk of an unintentional poisoning event did not change over the time period analyzed. The stability of the age-specific pattern over time lends support to the role of developmental processes in unintentional poisoning in young children.
Given the timing of the different phases of physical, cognitive, and affective development, a young child’s motor skills are developing to an advanced level, ahead of their cognitive and affective skills.2 This disparity may be one reason why childhood poisonings occur. A child is physically capable of accessing a substance without understanding that the substance is dangerous and/or without being able to fully resist the impulse to access it. As a child ages, cognitive and affective skills develop further, possibly accounting for the decrease in the risk of unintentional poisoning in children aged 4 years.
Key points
Rates of hospitalization for unintentional poisoning were significantly higher in children aged 1–3 years than in children aged <1 year and 4 years.
The same age-specific pattern in hospitalization rates for unintentional poisoning was seen for both boys and girls, but those for boys were significantly higher than those for girls at age 3 years.
The age pattern for hospitalization due to unintentional poisoning by single year of age was found to be stable when analyzed over time and by sex, remoteness of residence, and socioeconomic status.
The age-specific pattern was also analyzed by sex, remoteness of residence, and socioeconomic status, and some differences were found. The overall age-specific pattern was the same for both sexes; however, trend analysis showed that boys and girls aged 1 year have roughly the same level of risk for unintentional poisoning, but differences in risk level start to appear at the age of 2, and are obvious (and statistically significant) by the age of 3. Differences in the rate of physical, affective, and cognitive development may explain part of the difference between the levels of risk between boys and girls as they age.2 The age/sex-specific pattern for poisoning hospitalization may be due to advanced gross motor abilities combined with slower affective development in boys than girls. It is possible that other factors previously shown to account for developmental differences between the sexes, such as socialization practices and the nature of parent-child interaction, also play a role.14–18
The age-specific pattern was also the same for analysis by all SEIFA and ARIA categories used to indicate socioeconomic status and remoteness of residence, respectively. The fact that the age pattern persisted indicates that a factor(s) other than the level of economic disadvantage and/or access to medical care and other facilities (the basis of the ARIA categories) underpin a young child’s risk of an unintentional poisoning event.
The stability of the age pattern by SYA across time, by sex and by SEIFA and ARIA categories, provides strong evidence for the role of a child’s development in an unintentional poisoning event. This may be a direct contribution on the part of the child or may be due to other factors acting either alone or in combination with a child’s development. These include the nature of interaction with caregivers, socialization practices used by caregivers, caregiver’s safety practices, or caregiver’s supervision style. For example, a less than adequate relationship between a caregiver and a child may lead to an underestimation of that child’s abilities, which may result in inadequate supervision and inadequate safety rules and safety practices in the home environment.
The limitations of this study include the admission criteria used by hospitals in NSW and the validity of the hospitalized poisoning cases. In terms of admission criteria, poisoned children who are observed in emergency departments for extended periods of time may automatically become “hospitalized” patients after a set period of time, but this time criterion may not be uniform across NSW hospitals. In terms of the validity of the poisoning cases, only children whose parents or caregivers brought them to a hospital for treatment and who were ultimately admitted to hospital are included. There may be other children who experienced an unintentional poisoning event who would have been admitted, but were never brought to a hospital for treatment. The parents or caregivers of these children may have contacted the NSW Poisons Information Centre and been referred to a general practitioner for treatment or been advised to watch the child at home.19 Given the findings and limitations of this study, the role of parent and child behavior, the utilization of the NSW Poisons Information Centre, and hospital admission policies for childhood poisoning should be investigated.
IMPLICATIONS FOR PREVENTION
Children aged 1–3 years have been identified as a high-risk group for unintentional poisoning, and a highly plausible link to the influence of developmental stages has been demonstrated. Parents and caregivers should be taught to anticipate a child’s risk of poisoning based on their current physical, affective, and cognitive abilities and to respond appropriately with increased supervision in conjunction with other protective measures (eg, child-resistant closures, lockable cabinets). Finally, organizations that produce or promote safety information and products for preventing childhood poisoning should ensure that their information and products are suitable for preventing poisoning in children aged 1–3 years.
Acknowledgments
We thank the Centre for Epidemiology and Research at the NSW Health Department for providing the NSW Inpatients Statistics Collection data from the Health Outcomes and Information Statistical Toolkit (HOIST) analyzed in this study. The authors contributed to the paper as follows. MS conceived and designed the study, acquired, analyzed, and interpreted the data, and drafted the manuscript. AW conducted a critical review of the manuscript for important intellectual content and also assisted with the design of the study, the statistical analysis, and interpretation of data. DB conducted a critical review of the manuscript for important intellectual content and also assisted with the interpretation of data. Dr Andrew Hayen assisted with the statistical analysis. Jane Pines conducted a critical review of the manuscript for important intellectual content. Dr Gary Schmertmann conducted a critical review of the manuscript for important intellectual content and also assisted with the statistical analysis.
Footnotes
Competing interests: None.
Funding: MS is supported by the NSW Injury Risk Management Research Centre, with core funding provided by the NSW Health Department, the NSW Roads and Traffic Authority and the Motor Accidents Authority. AW is supported by a National Health and Medical Research Council (NHMRC) Senior Research Fellowship.