Article Text

Abstract
Objective: To evaluate the effect of a bridge safety fence in preventing suicide.
Methods: We examined suicides from jumping off the Memorial Bridge in Augusta, Maine, from 1 April 1960 to 31 July 2005. The safety fence was installed during 1983, the mid-point of the study period.
Results: 14 suicides from the bridge were identified; all occurred before installation of the safety fence. The number of suicides by jumping from other structures remained unchanged after installation of the fence.
Conclusion: The safety fence was effective in preventing suicides from the bridge. There was no evidence that suicidal individuals sought alternative sites for jumping.
- ICD, International Classification of Diseases
Statistics from Altmetric.com
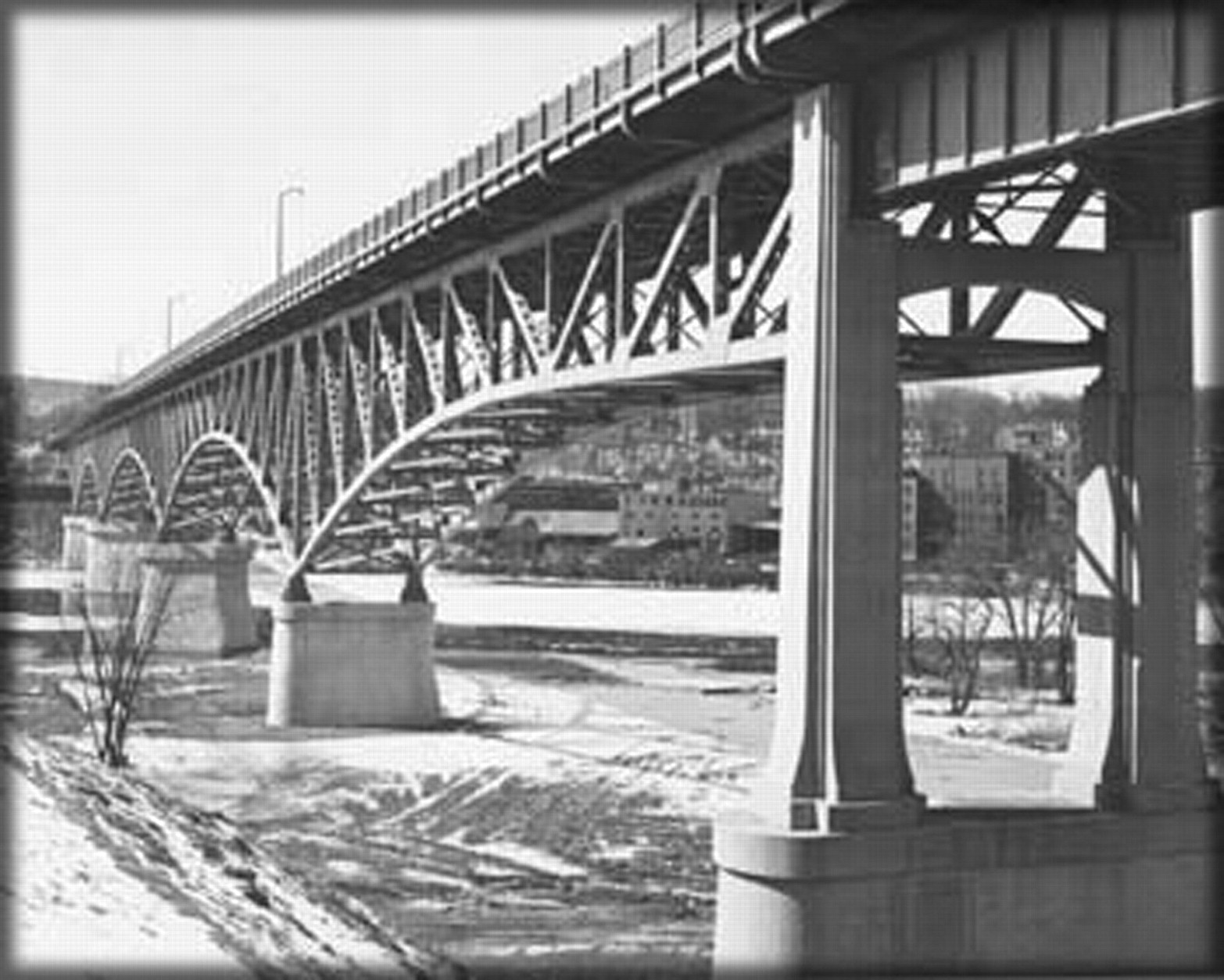
The Memorial Bridge in Augusta, Maine (population 24 511), spans the Kennebec River (fig 1). Completed in 1949, the bridge is approximately 2100 feet long and has two lanes for traffic and a sidewalk for pedestrians on each side of the roadway. The central portion of the bridge is approximately 100 feet above the river. The Memorial Bridge is located near a state psychiatric hospital. After a number of suicides involving people jumping off the bridge, an 11 foot-high safety fence was installed on each side of the bridge in 1983.

The Memorial Bridge in Augusta, Maine.
As part of a renovation, the safety fence was removed in August 2005. The community subsequently began to discuss whether the fence should be reinstalled when the bridge renovation was completed. To assist the community in making that decision, the Maine Department of Health and Human Services examined suicides involving the bridge.
METHODS
A case was defined as the death of a person by suicide from jumping off the Memorial Bridge in Augusta, Maine, from 1 April 1960 to 31 July 2005. The study period included 22 years and 2 months both before and after installation of the safety fence in June 1983. Data for 1968 were not available. Potential cases were identified by examining death certificates with International Classification of Diseases (ICD) codes for suicides in Augusta caused by jumping from a high place or drowning (ICD-7, 1960–7 (E975, E978); ICD-8, 1968–78 (E954, E957); ICD-9, 1979–98 (E954, E957); and ICD-10, 1999–2005 (X71, X80)). For each potential case identified through death certificates, additional information was sought from the archives of the Kennebec Journal newspaper, death investigations conducted by the state medical examiner and medical records of the state psychiatric hospital in Augusta. Information from these sources was used to describe the general characteristics of cases.
Data on all suicides in Augusta and in Maine during the study period were obtained from death certificates using ICD codes for suicide (ICD-7, 1960–7 (E963, E970–E979); ICD-8, 1968–78 (E950–E959); ICD-9, 1979–98 (E950–E959); and ICD-10, 1999–2005 (X60–X84, Y87)). Population data for Augusta and Maine were obtained from the US census. The Centers for Disease Control and Prevention determined that the study was exempt from institutional review board oversight because the study did not involve any living persons.
RESULTS
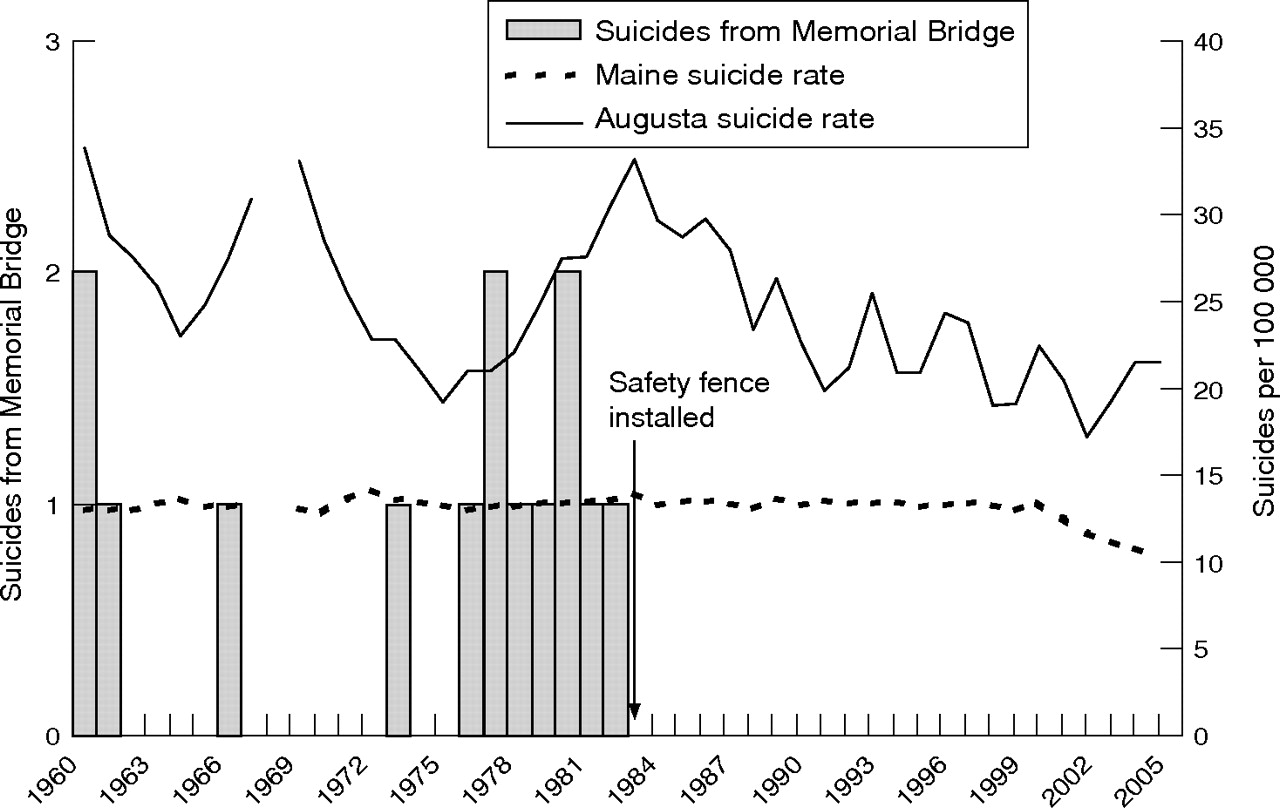
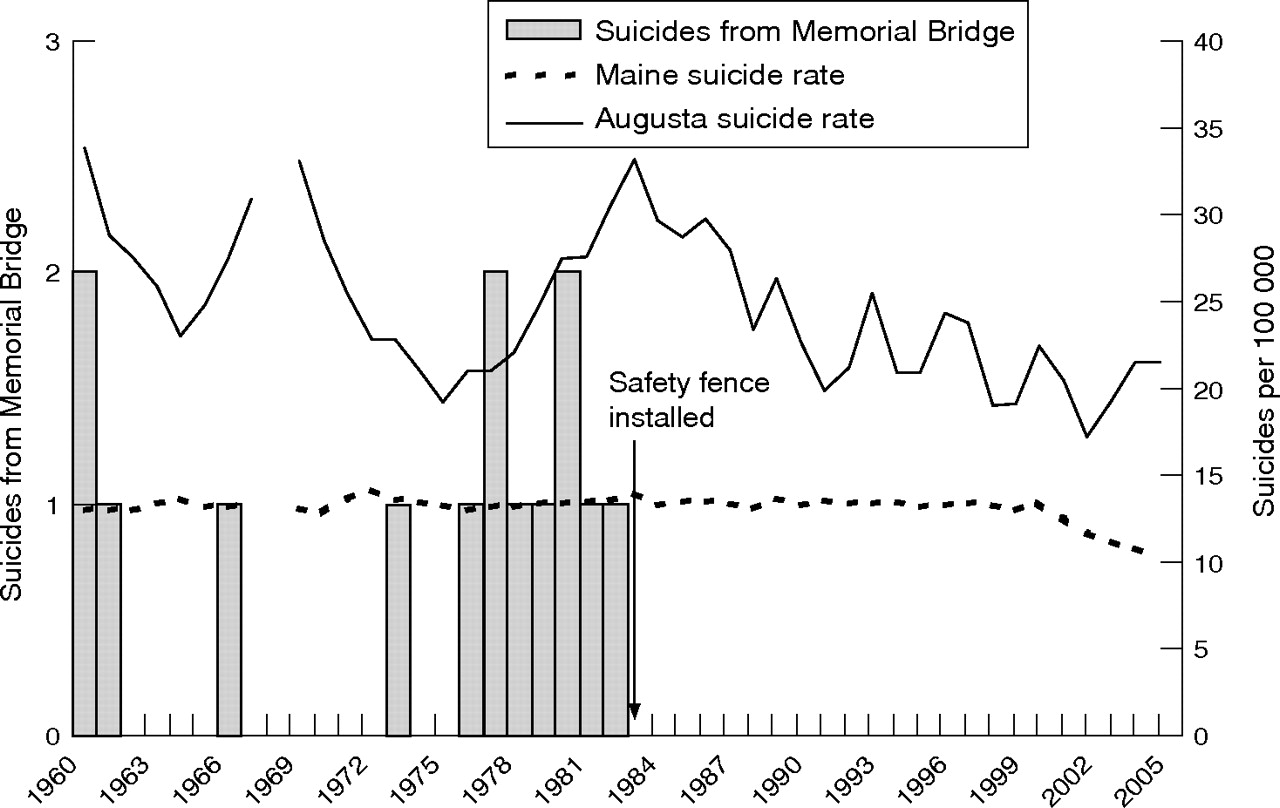
A total of 14 suicides involving the Memorial Bridge were identified; all occurred before installation of the safety fence (fig 2). These suicides represented 6% (14/232) of all suicides in Augusta during the study period: 14/126 (11%) before installation of the fence and 0/106 (0%) after installation of the fence. The median age of case patients was 39.5 years (range 21–72 years), and all were white; 11 (79%) case patients were male; 8 (57%) were single, 4 (29%) were married, 1 (7%) was divorced and 1 (7%) was widowed; 10 (71%) were living in Augusta at the time of their death; the other 4 (29%) lived in neighboring communities; 7 (50%) suicides occurred on a Friday or Saturday; 10 (71%) of the deaths were witnessed; 7 (50%) occurred between noon and 17:59 h. No more than two deaths occurred in any month of the year. No seasonal patterns were noted. Death was due to drowning in 8 (57%) cases and due to blunt trauma in 6 (43%) cases. All six cases attributed to blunt trauma were from striking the ground on either side of the river. A total of 10 (71%) case patients had a documented history of psychiatric illness; 9 (64%) had been previously admitted to the state psychiatric hospital in Augusta. Five of the case patients with a history of psychiatric illness had been diagnosed with schizophrenia and four with depression; information was unavailable for one. At the time of death, 6 (43%) case patients were hospitalized or living in a residential treatment facility. Tests for blood alcohol were performed in 2 (14%); both tested positive (0.21 and 0.03 g/dl).
{kind=link}
{kind=link}
Suicides from the Memorial Bridge and per 100 000 in Augusta and Maine, 1960–2005.
From 1960 until the installation of the safety fence, there were nine suicides in Augusta from jumping from a high place (n = 3) or drowning (n = 6) that were not associated with the Memorial Bridge. Only one of these deaths involved jumping from a bridge. After installation of the safety fence, until 2005, there were nine suicides in Augusta from jumping from a high place (n = 3) or drowning (n = 6) not associated with the Memorial Bridge. Two of these deaths involved jumping from a bridge.
The suicide rate in Maine from 1 April 1960 to 31 May 1983 was 13.4/100 000/year and from 1 June 1983 to 31 July 2005 was 13/100 000/year, a decrease of 3% (p = 0.26). The suicide rate in Augusta from 1 April 1960 to 31 May 1983 was 26/100 000/year and from 1 June 1983 to 31 July 2005 was 23.8/100 000/year, a decrease of 9% (p = 0.49). Suicides in Augusta accounted for 3% (232/6646) of all suicides in Maine during the study period.
CONCLUSIONS
The results of this study indicated that the safety fence installed in 1983 was effective in preventing further suicides from the Memorial Bridge. The number of suicides related to jumping from other structures in Augusta remained unchanged after installation of the fence, suggesting that suicidal individuals did not seek alternative sites. Although the decline in the suicide rate in Augusta after installation of the safety fence was not statistically significant, measuring the effect of a safety fence on the overall suicide rate in a community can be difficult because of the relatively small percentage of suicides from jumping.1
Numerous studies have shown that particular bridges can become attractive sites for attempting suicide.1–8 The Golden Gate Bridge in California is the best-known example.4,9,10 It seems that for certain individuals, both the method (ie, jumping from a high place) and the location of the attempt are important factors in the decision to commit suicide. Restricting access to certain lethal means has been found to prevent suicide.11 Interventions such as safety fences can be effective in preventing suicides at specific locations.1 Fencing may be especially effective in preventing impulsive acts. Persons who were restrained from jumping off from the Golden Gate Bridge infrequently went on to die by suicide.4
The demographics of persons committing suicide from the Memorial Bridge were affected by the nearby location of the state psychiatric hospital. Other studies involving suicide by jumping have noted similar findings when psychiatric facilities were adjacent to bridges.5,12
This study has at least three limitations. Firstly, data for 1968 were not available. However, it is unlikely that one year’s data would have had a substantial effect on the study results given the length of the overall time period examined. Secondly, electronic death records from 1960 to 1974 do not meet current data quality standards. This may have resulted in an underestimate of suicides from the Memorial Bridge during that time period. Thirdly, data were not available for non-fatal incidents involving the Memorial Bridge. Focusing only on deaths underestimates the public health effect of suicide attempts from the bridge.
On the basis of this study, the safety fence seemed to be effective in preventing suicides. After extensive community input, the Augusta City Council voted 7:1 on 18 April 2006 to support replacement of the safety fence after renovations to the bridge were completed. After the council’s vote, the Maine Department of Transportation, the agency responsible for the bridge renovation, agreed to reinstall the fence. Installation of the fence should be part of a comprehensive approach to suicide prevention that includes improving screening and treatment of persons at high risk as well as efforts aimed at building coping skills in children, adolescents and adults and strengthening community-based programs.
Acknowledgments
This report is based, in part, on contributions from U Jacobsohn, MD; B Corkum, C DiCara, W Nelson, MD, Maine Department of Health and Human Services; W Frankhauser, Maine Department of Transportation; M Greenwald, MD, Maine Office of Chief Medical Examiner; A Crosby, MD, M Kresnow, MS, Centers for Disease Control and Prevention.
REFERENCES
Footnotes
-
Funding: There was no external funding for this study. The work was conducted by a federal employee with the Centers for Disease Control and Prevention. The Centers for Disease Control and Prevention reviewed and approved the manuscript.
-
Competing interests: None.
-
As principal investigator, Dr Pelletier had full access to all the data in the study and had final responsibility for the decision to submit for publication.