Article Text

Abstract
Objective: To define health outcomes of whiplash associated disorders (WAD) at three months, six months, and two years after injury and to examine predictors of these outcomes.
Design: Prospective cohort study.
Setting: New South Wales, Australia.
Subjects: People with compensable motor crash injuries who reported whiplash as one of their injuries.
Interventions: None.
Main outcome measures: Functional Rating Index (FRI), Short Form 36 (SF-36) at three months, six months, and two years after injury, ascertained by telephone interview.
Results: At three months, 33.6% of the cohort was recovered (as defined by FRI⩽25), increasing marginally at six months (38.9% recovered), but more significantly at two years (51.7% recovered, p = 0.001). The mean physical component score of the SF-36 improved at each time point (p = 0.002), while the mean mental component score did not (p = 0.59). Predictors of recovery at two years (as defined by global perceived effect) included a lower FRI index at baseline (p = 0.001) and closure of the claim at two years (p = 0.02).
Conclusion: Whiplash injury had a large effect on the health of this Australian cohort of whiplash sufferers, with only 50% of the cohort recovered at two years. Physical measures of health appear to improve over time, whereas mental measures of health did not. Despite this, this cohort is largely able to participate in activities and work at two years. Prevention of chronic disability may lie with concentration of resources to those who score highly on the FRI at baseline. In addition, chronic psychological ill health may be prevented by directing treatment to those with poor scores on sensitive measures of psychological ill health at baseline.
- ANF, Accident Notification Form
- CTP, Compulsory Third Party
- CWOM, Cumberland Whiplash Outcome Measure
- FRI, Functional Rating Index
- IRSD, Index of Relative Socioeconomic Disadvantage
- MAA, Motor Accidents Authority
- MCS, mental component score
- PCS, physical component score
- QTF, Quebec Task Force
- SF-36, Short Form 36
- WAD, whiplash associated disorders
- whiplash associated disorder
- health outcomes
- cohort study
- prognosis
Statistics from Altmetric.com
- ANF, Accident Notification Form
- CTP, Compulsory Third Party
- CWOM, Cumberland Whiplash Outcome Measure
- FRI, Functional Rating Index
- IRSD, Index of Relative Socioeconomic Disadvantage
- MAA, Motor Accidents Authority
- MCS, mental component score
- PCS, physical component score
- QTF, Quebec Task Force
- SF-36, Short Form 36
- WAD, whiplash associated disorders
Whiplash associated disorders (WAD) were first defined by the Quebec Task Force (QTF) in 1995.1 Health outcomes for WAD have been reported to vary widely in the literature.2,3 Recovery in the short term is reported to vary from between 29%4 to 90%.5 Studies reporting long term follow up show that 76%6 to 97%7 are recovered by 12 months. Differences in health outcomes reported may arise from the difference in cohorts (for example, participants recruited from emergency clinics or insurer databases) and the participant’s insurance compensation status (compensation eligible versus ineligible).3 In addition, studies report health outcomes using different measures. Higher recovery rates are reported when outcome measures are based on finalization of the claim,1,8 and lower recovery rates when outcomes are reported in terms of symptoms or disability.9,10 Health outcomes reported according to more comprehensive and consistent outcome measures may allow for a more complete understanding of health outcomes following WAD.
Identifying WAD sufferers who are less likely to recover is important, in order to try to address the poor health outcomes of WAD. Factors associated with poor prognosis from WAD have differed over time. In Australia, clinical guidelines were released with poor prognostic indicators identified as sociodemographic, psychosocial, compensation, and symptom related factors.11 This categorization was based on the QTF findings1 and updated by a systematic review of research published since then. Subsequently published systematic reviews conclude that the consistent factor in determining poor recovery is initial symptom intensity, with psychosocial and compensation based factors concluded by these authors not to predict outcome.3,12 However, more recent prospective studies challenge this again, finding psychological factors such as the initial health status using the SF-3613 and acute post traumatic stress9 to be predictive of poor outcome in WAD. Clearly there is a need for further research to examine all of these potential prognostic indicators in order to determine which are more predictive of poor outcome in WAD.
This paper seeks to define the health outcomes of a prospective cohort of people with WAD using a comprehensive set of health outcome measures. In addition, we aim to examine relationships between poor outcome and the identified potential prognostic indicators,11 in order to present a more complete understanding of recovery and therefore assist in the prevention of chronic disability following WAD.
METHOD
Study population and design
The cohort was prospective, and claimants were selected from an insurance claims database maintained by the Motor Accidents Authority (MAA), the state government regulator of companies providing Compulsory Third Party (CTP) insurance in New South Wales (NSW), Australia. CTP insurers are legislatively bound to register motor vehicle crashes with the MAA for claimants not “at fault” in the crash. Usually, CTP insurers are informed of the accident from the claimant’s medical practitioner who completes an Accident Notification Form (ANF).14 The MAA database therefore holds baseline reported data on all registered crashes in NSW, with claimants not at fault, having sustained injuries as described above.
Claimants were included if they were injured in the period July to December 2001, and would have been affected by the first stage legislative changes introduced in 1999. These changes included the removal of non-economic loss payments for minor injuries, (which included most claims for whiplash injury), admission of provisional liability by the insurer within three months, and introducing fixed legal costs. Claimants classified with the injury code of “whiplash” were included. Claimants under 18 years of age, non-English speakers, bicyclists, and pedestrians, or those classified with injury codes other than the above, such as spinal injuries and fractures, were excluded.
Claimants were initially sent a letter by the MAA to seek permission to be contacted. Those who did not refuse participation in writing were contacted by an experienced health interview company, which was unaware of the study hypotheses, to collect health outcome data by telephone interview. Training of interview staff to administer the health outcome questionnaires was completed by the authors.
Health outcome measures
Health outcomes at baseline (three months), six months, and two years after injury were assessed by responses to questions from the Functional Rating Index (FRI),15 the Medical Outcomes Study Short Form 36 health status measure (SF-36),16 and the Cumberland Whiplash Outcome Measure (CWOM).
The FRI was used as the health outcome measure to quantify the patient’s state of pain and dysfunction, and to measure the initial severity of the WAD injury. It measures disability due to neck and back pain, with demonstrated good reliability and validity.15 The total possible raw score is 40, which converts to an index score of 100. Lower scores indicate lower pain and dysfunction. There are no published normative data for the FRI, therefore the authors considered an index score of 25 or less (lowest quartile) to be defined as recovered.
The CWOM was developed from a proposed core outcome measure.17 This six item questionnaire includes a measure of symptom bothersomeness, function, wellbeing, disability (work and social), and patient satisfaction with care. It was expanded to include a global perceived effect of recovery and a question regarding treatment provider satisfaction, to produce the CWOM.
The SF-36 was chosen as the outcome measure that was able to evaluate quality of life, mental health, and to allow comparison with the Australian population normative data.16,18 The eight dimensions of health measured by the SF-36 are expressed on a scale of 0 to 100, where a higher score indicates a better state of health or wellbeing. Physical and mental component scores (PCS and MCS, respectively) are summary component scores of the eight dimensions, and are compared with the Australian norms18 with a mean of 50 and standard deviation of 10.
Predictors of poor prognosis
Potential poor prognostic indicators as published in the MAA guidelines11 were identified from the claims database or from initial health outcome measures. Sociodemographic factors identified from the claims database included gender, age, employment status, occupation, and Index of Relative Socioeconomic Disadvantage (IRSD) score (based on education, occupation, income, family structure, ethnicity, and housing). High scores on the IRSD indicate less relative disadvantage.19 Compensation or claim related factors identified on the claims database included claim status (open or closed at two years), driver, time to admit liability, economic loss claim, and prior personal injury claim. The initial score of disability on the FRI was used as an indicator of initial injury severity, while the initial mental health component score was used as an indicator of baseline psychological health.
Statistical methods
The characteristics of participants at three months, six months, and two years after injury were compared with those of non-participants. For continuous measures (for example, IRSD) we used Student t statistics to test significant differences between means of these two mutually exclusive groups. In case of categorical data which were described proportionately (for example, gender) we used χ2 to test a difference in proportions between respondents and non-respondents.
Health outcomes (FRI and CWOM) at three months, six months, and two years after injury were described in terms of mean, SE (standard error of the mean), median, and interquartile range. The changes in means of health outcomes over time were tested using repeated measures analysis of variance (ANOVA). The proportion of claimants who were recovered at each time period was calculated using three cut-off points (25, 50, and 75) of the FRI index score. Significant changes in this categorical response between the three interviews were tested using Cochran’s Q statistic.
Simple and multiple linear regression were used to identify statistically significant predictors for recovery. The global perceived effect (scale: –5 vastly worse to +5 completely recovered) was used as the measure of recovery for this test. All analyses were performed using SPSS statistical software for Windows version 11.0, with p levels of 0.05 taken as statistically significant. Ethical approval for the study was obtained from the Western Sydney Area Health Service Ethics Committee.
RESULTS
There were 859 people who reported WAD as an injury in the period July to December 2001. Of these, 250 consented to participate in the study and were interviewed at three months for baseline data. This represented 29.1% of people reporting WAD during the study period. Non-participants included 309 who refused consent, 38 with a language barrier, and 262 who could not be contacted. One hundred and ninety eight (79.0%) completed the six month interview and 147 (59%) competed the two year interview. Dropouts at two years were due to no longer at the address (57), withdrawal from the study (11), “too busy” (13), insurance issues (8), and other (14). Data were analysed on 114 subjects who completed the interview at each time point.
Baseline characteristics of interviewed claimants (n = 114) were compared with non-interviewed claimants (n = 745) in the cohort (table 1), with no significant differences observed. The characteristics of subjects interviewed at all three time points (n = 114) and subjects not completing all three interviews (n = 136) were compared (table 1), with no significant differences observed.
Baseline characteristics (%) of claimants with WAD in NSW in July to December 2001
Health outcomes: disability and participation
The mean (SD) FRI total index score (max score = 100) at three months was 36.8 (2.09). There was a significant linear decreasing trend (p = 0.001, table 2) with the FRI reducing to 34.5 (2.28) by six months and 32.1 (2.40) by two years. At three months, 33.6% of people were considered recovered, measured by a score of <25/100 on the FRI. This increased marginally at six months (38.9% recovered), but more significantly at two years (51.7% recovered, p = 0.001, table 2).
Health outcome measures at baseline (three months) and at follow up (six months and two years) after sustaining whiplash injury
The mean (SD) global perceived effect of recovery (scale –5 (vastly worse) through to +5 (completely recovered) did not significantly change over time (p = 0.53). The days cut down on regular activity significantly reduced with each time period (p = 0.001, table 2). The mean number of days taken off from work due to the WAD injury over the previous month did not significantly reduce between three months and two years (p = 0.98, table 2). However, the percentage of participants taking days off work reduced from 24.4% (n = 61) at three months to 20.2% (n = 40) at six months and 16.3% (n = 24) at two years.
Health outcomes: health related quality of life (SF-36)
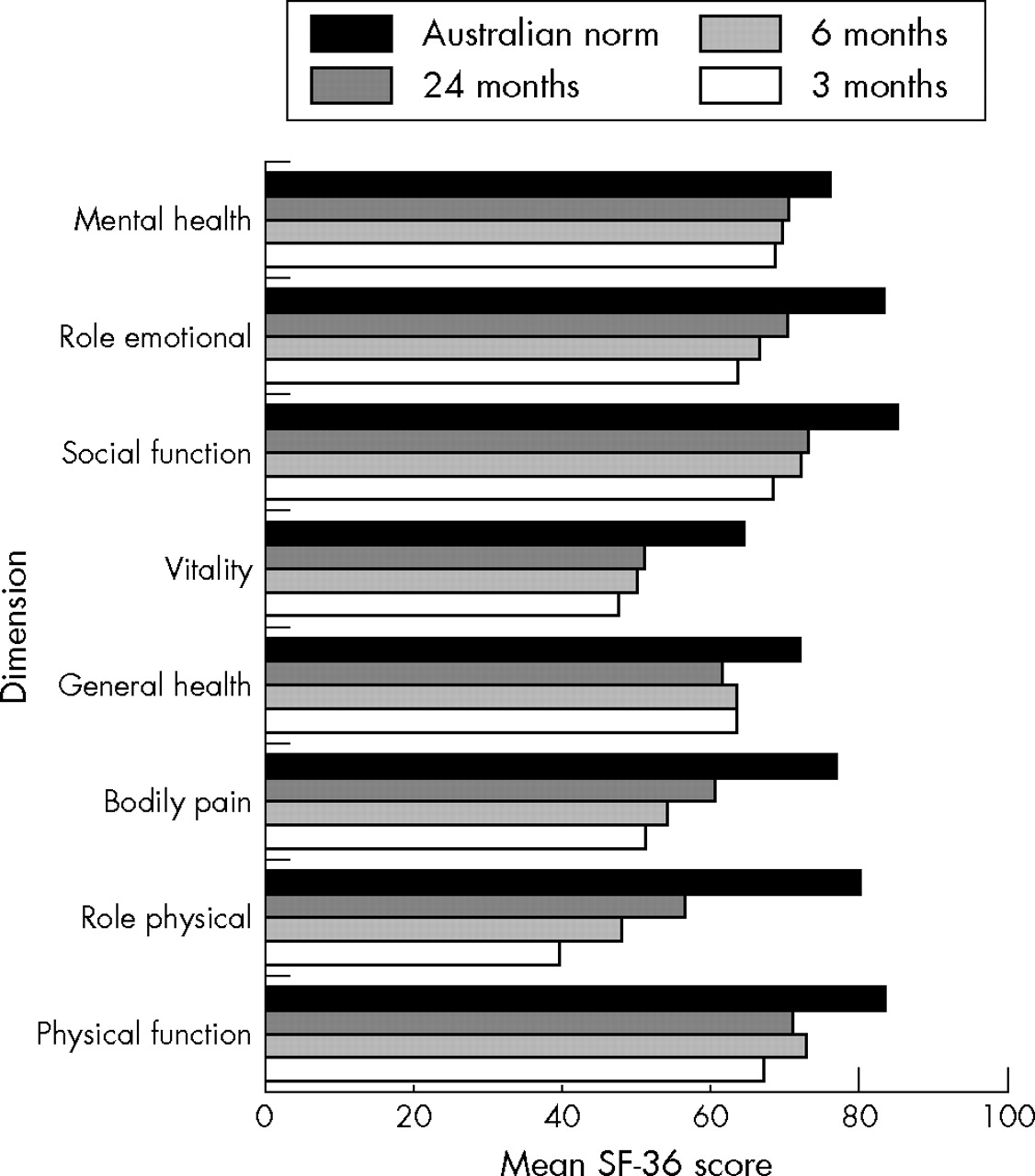
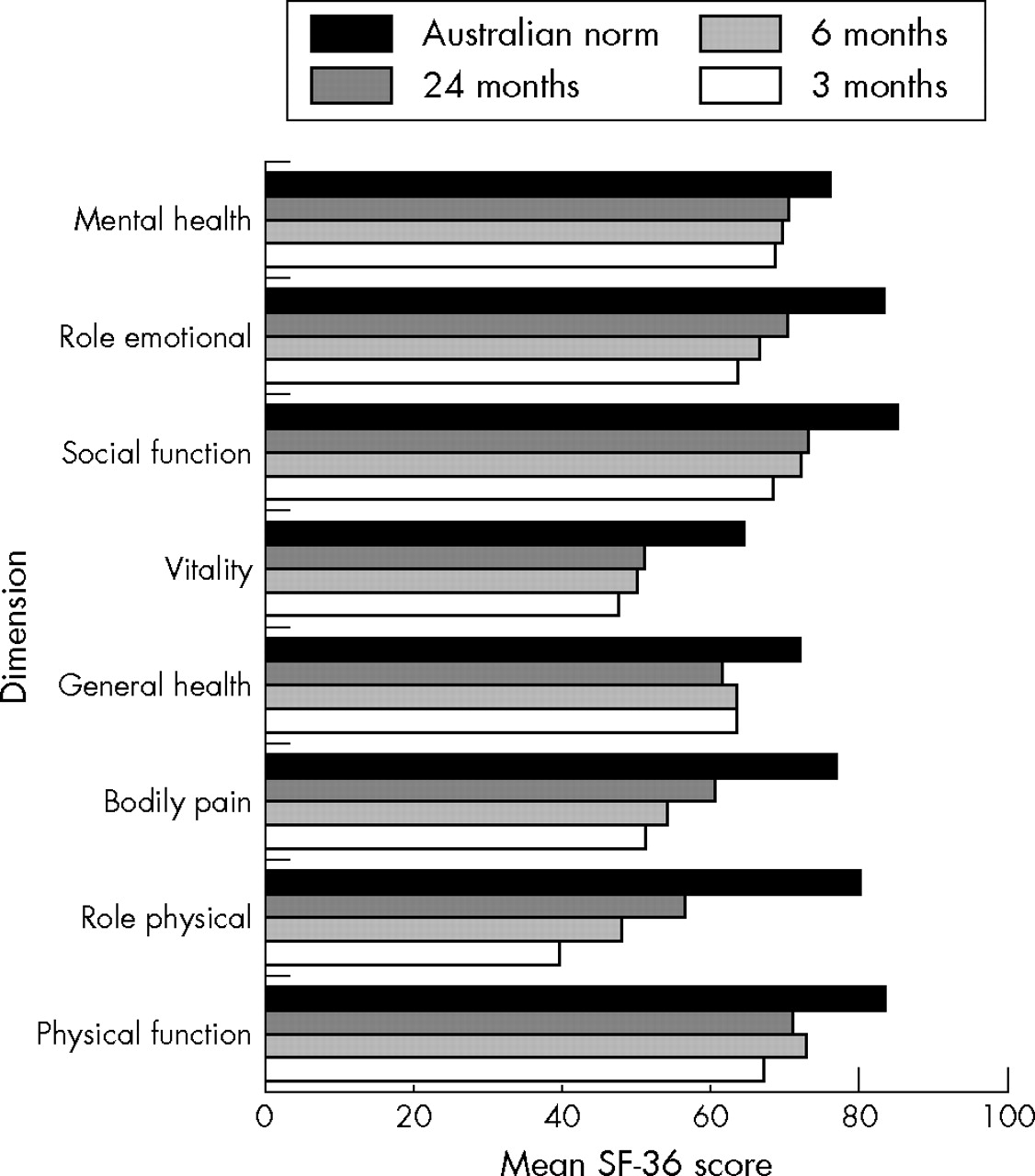
The mean (SD) physical component score for the SF-36 statistically improved at each time point; three months (40.6 (1.0)), six months (42.6 (1.0), and two years (43.7 (1.1), p = 0.002). However, the mean mental component score did not significantly change as time progressed, with the mean at three months 43.5 (1.2), at six months 44.0 (1.3), and two years 44.7 (1.3), p = 0.59. The profile of the eight domains of the SF-36 compared with the Australian normal population18 is shown in figure 1. Significant improvement occurred as time progressed for the dimensions of role physical (p = 0.001) and bodily pain (p = 0.001). In contrast, no significant improvement occurred over time for the dimensions of physical function (p = 0.08), general health (p = 0.51), role emotional (p = 0.25), vitality (p = 0.09), social function (p = 0.07), and mental health (p = 0.43).
{kind=link}
Short Form-36 scores of whiplash patients at three months, six months, and two years after injury, compared with the Australian normal population.18
Independent predictors of recovery
The global perceived effect was the measure of recovery for these analyses. The predictors of poor recovery using simple linear regression are outlined in table 3. In the final multiple linear regression model, the initial injury disability score (measured by the initial FRI index, p = 0.001) and the status of the claim (that is, open or finalised, p = 0.02) were the only significant predictors of recovery (table 4). Specifically, every 10% increase in the FRI index reduced the likelihood of recovery by 40%. The global perceived effect of claimants with opened or reopened claims was 1.41 times higher on the scale than those with finalised claims (table 4).
Potential predictors for recovery tested using simple linear regression
Potential predictors for recovery tested using multiple linear regression (r2 = 0.20)
DISCUSSION
Whiplash injury had a large effect on the health of this Australian cohort of whiplash sufferers, with only 50% of the cohort recovered at two years. Pain, disability, and physical functioning improve over time, with improvement continuing over two years. Mental health status did not change over time. Non-recovery is highly associated with initial levels of disability, suggesting that early identification of disability is important prognostically. Lastly, even with elements of compensation changed to expect better outcomes, claim closure at two years was associated with a higher report of recovery.
The comprehensive set of health outcome measures used have provided the opportunity to report on a detailed profile of recovery after whiplash, with respect of pain, disability, quality, and participation in daily life. A little over 30% of the cohort was recovered at three and six months, with this improving to 50% of the cohort by two years. Self reported physical measures of disability (FRI) and health related quality of life (SF-36 physical component score) improved significantly over time in this cohort, and continued to improve for at least two years. However, the physical health is still well below the Australian population norm at two years (fig 1). This has implications for treatment, particularly given that treatment guidelines11,20 in Australia have focussed on the management of acute WAD based on the assumption that most sufferers should recover in the acute phase of the condition. With recovery continuing into the chronic phase of the condition, clearly there is a need to monitor and manage some of these people for at least two years. Longer term follow up would be required in order to determine whether recovery and therefore ongoing monitoring is required beyond two years.
Clarification regarding the severity of disability following WAD is found with participation in daily life. Despite poor health in terms of disability and health related quality of life, the majority of this cohort are not restricted in their participation in daily life and work in the long term. By two years, only 16% of the cohort had some time off work in the previous month, and the median days of restriction of work activities were 0 days. Hence if recovery were to be reported in terms of work participation, we would be reporting an 84% recovery, which approximates studies that use similar measures of outcome.1 This highlights the importance of consistency of outcome measures used when reporting recovery in whiplash. More importantly, the implications for advice to patients may well be that we can expect that most people will not be limited at work in two years, despite the persistence of symptoms and some disability.
Non-recovery in this cohort was most significantly related to initial disability (as measured by the Functional Rating Index). High scores on other disability scales (such as the Neck Disability Index) have also been highly correlated with poor health outcomes9,10 in whiplash. The FRI measure used in this study also shows a similar predictive ability, and is able to measure disability due to back and neck pain and hence may be more useful in WAD. We suggest therefore, that early administration of the FRI may identify potential non-recoverers, who in turn may require more intense monitoring in order to prevent chronic disability. Further qualitative research focusing on whiplash sufferers with a high initial FRI score may offer a more detailed understanding of non-recovery.
Our observation that psychological health did not change over time in this cohort, and was not predictive of outcome, warrants further discussion. Firstly, we found that the mental health of this cohort of whiplash patients was low initially and did not change over time, despite recovery in the physical measures of health. This suggests the recovery of mental health is not related to the recovery of physical health in WAD. Pre-existing psychological ill health may explain our observation, and has been found in one other study. Kivioja et al (2004) found premorbid psychiatric ill health more common in patients with chronic WAD than in those who recovered.21 Therefore, we may be observing a group with certain psychological characteristics who are more likely to seek compensation after WAD. However, equally, lack of change in mental health status may reflect inadequate management of psychological factors in this cohort. Post hoc analysis of the proportion of funds allocated to psychological health at the time of the study was 1%, compared with the 99% directed at physical health. This implies that if poor psychological health is displayed at onset, more funding and management should be directed at psychological health, in order to prevent long term chonicity.
The validity of the mental health component score of the SF-36 as a tool to measure psychological health and predict outcome in WAD is brought into question by our data. In part this may be because we used a tool (the FRI) with a higher predictive ability in the multiple regression model. We note that many studies found psychological factors to predict recovery when measures of initial disability were not included in the analysis,13,21,22 or when multiple regression analysis were not performed.6 The exceptions are recent studies, which used different measures of psychological health at baseline and reported a greater predictive ability.9,23 For example, models have predicted 65%23 and 67%9 of the variance using measures of somatization and acute post traumatic stress respectively. However, in both these studies, the measure of outcome was also used as a predictor in the model, hence higher associations would be expected. Despite this, both authors concluded that the combination of symptoms and psychological variables predicted outcome. Therefore, the SF-36 measure of mental health is not predictive of poor outcome in WAD when an initial measure of disability is included in the analysis. However, more sensitive measures of psychological health as discussed should be considered in further studies.
Lastly the role of compensation process was found significant in this cohort, even in an environment where aspects of the compensation regulations have been altered to improve outcome. Compensation for “pain and suffering” was effectively abolished, and access to early treatment improved—factors which have been associated with better health outcomes in Canada8 and in our recent Australian study.24 Closing the claim was the additional compensation factor related to higher reports of recovery by this cohort. This supports conclusions of other studies that find compensation related to non-recovery,10,25 and that better rates of recovery were reported in cohorts where non-compensated patients were included.6,26 However, given that claim closure only increased the report of recovery by 1.4 on an 11 point scale, encouraging claim closure to improve health outcomes is only likely to have a marginal effect.
We are confident in the conclusions made in this study despite the weaknesses of capturing only 29% of the total cohort for the time period selected, and a loss to follow up of 46% at two years. The sample is representative of the whole cohort, as baseline characteristics between the interviewed and non-interviewed participants are similar. The dropout rate is random, because the baseline characteristics (including injury severity and claim status) of the dropouts did not differ from those completing all three interviews (table 1). The follow up rates are considered acceptable27 due to the random nature of dropouts and are similar to those reported in other recent studies.10,13
Key points
-
A comprehensive picture of the short and long term health of whiplash sufferers is presented.
-
Health outcomes are limited in this cohort of whiplash sufferers; 34% and 50% recovered at three months and two years respectively.
-
Recovery continues for two years.
-
Physical measures of health improve over time, mental health measures do not.
-
Predictors of recovery at two years are the initial disability (measured by the FRI) and closure of the claim at two years.
-
Prevention of chronic ill health after WAD may improve by directing resources to WAD sufferers with a high initial FRI and those with poor initial psychological health.
The strengths of this study include use of a database in which all WAD injuries are recorded for the state of New South Wales (Australia), a large prospective sample, assessment of outcomes by raters unaware of the study hypothesis, and the use of comprehensive, validated outcome measures. In addition, we have examined most of the potential poor prognostic indicators for WAD, so that a more complete picture of recovery after WAD is presented.
CONCLUSION
Health outcomes are limited in this cohort of Australian whiplash sufferers. Recovery continues for up to two years, with 50% of the cohort recovered at two years. Physical measures of health appear to improve over time, while mental measures of health did not. Despite this, this cohort is largely able to participate in activities and work at two years. Chronic disability may be prevented by identifying those who score highly with the FRI at baseline and directing more resources toward them. In addition chronic psychological ill health may be prevented by directing funding to those who are identified at baseline with poor scores on more sensitive measures of psychological ill health than the SF-36. Lastly, even with elements of compensation changed to anticipate better outcomes, claim closure was associated with a higher report of recovery.
Acknowledgments
The study was funded by the Motor Accidents Authority of New South Wales. This organization, which is the regulator of compulsory third party insurance companies, had no part in the analysis of the data or reporting of this study. The authors with to acknowledge Marnie Higlett of PriceWaterhouseCoopers, for her project management assistance.
REFERENCES
Footnotes
-
Competing interests: All authors received a portion of the research grant from the MAA (as stated in acknowledgements). The Rehabilitation Studies Unit receives infrastructure funding from the Motor Accidents Authority of NSW. IC is an employee of the Rehabilitation Studies Unit. TR receives funding from the MAA to educate CTP insurers.